Introduction
Sacrum is a large triangular fusion of five progressively smaller sacral vertebrae and their costal elements, maintaining the integrity of the spinal column [1]. It contributes to the stability of the pelvic ring by its situation, being wedged between the two hip bones and also endures weight transmission [2]. Sacrum is the target of lumbo-sacral fusion and instrumentation that are commonly done for metastatic, infectious, traumatic and degenerative diseases. Sacral screw insertion is commonly done at the S1 sacral wing (antero-laterally) or into the S1 promontory (antero-medially) [3]. S2 screw applications are usually chosen for sacral block fixations but rigid posterior S1 pedicle screw fixation enhanced by placement of S2 screws is becoming a common technique in lumbosacral fusion procedures [4,5].
Percutaneous fixation with ilio-sacral screws is a technically demanding technique and failure of sacral screw fixation may occur due to various factors, such as sacral anatomic variations and dysmorphism, insufficient sacral bone acquisition, inapt course of the screw or depth of the screw insertion and osteoporosis of the sacrum [3,4]. With the advance of minimally invasive surgical techniques, it is essential that the available implants are precontoured to the exact anatomical location which necessitates the comprehensive knowledge of morphometry of sacrum [6].
Differences exist in the morphometric values of sacrum across different study populations. So far, out of the studies available, few determine the morphometry of sacrum, especially in the Indian population. The present study was an attempt to quantify morphometric characteristics of the Indian sacra for safe screw placement during surgical instrumentation which is crucial for constructing a strategy to treat sacrum related diseases in Indian population.
Materials and Methods
A cross-sectional observation study was conducted on 108 dry adult human sacra in Department of Anatomy. Sacra showing damage, bony outgrowth which influences differentiation or measurement were excluded from the study. Linear measurements were taken with the help of digital verniercaliper which was accurate up to 0.01 mm. Angles were measured by a goniometer which was accurate up to 1°. Measurements were taken twice and average was taken.
The following parameters were observed and measured:
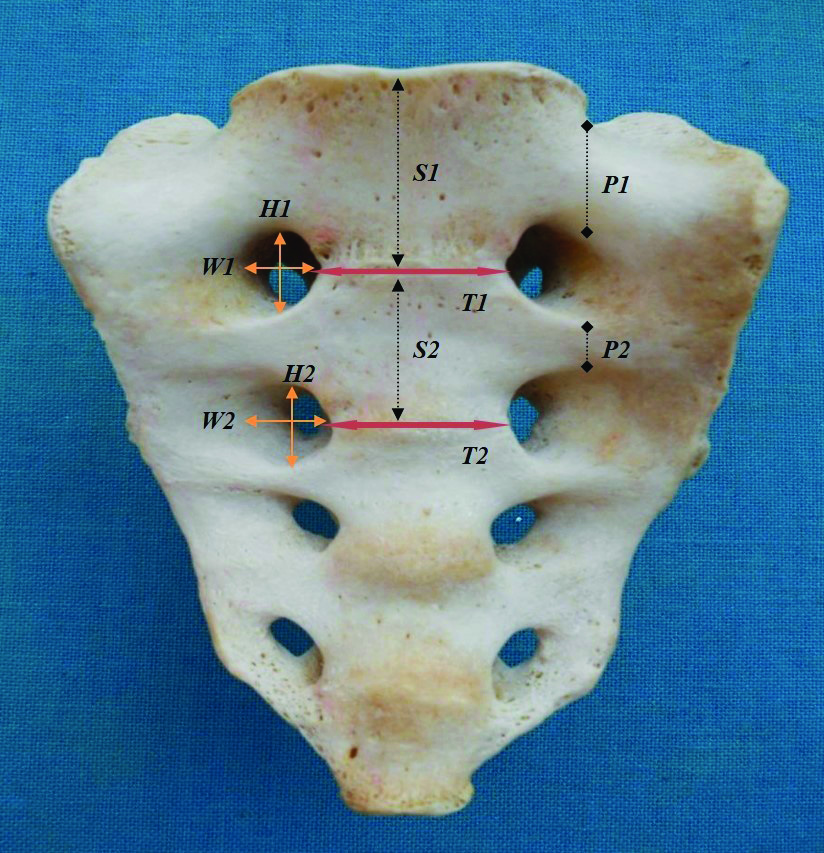
Anterior surface of sacrum showing linear parameters.
H1: Height of the first ASF
W1: Width of the first ASF
H2: Height of the second ASF
W2: Width of the second ASF
T1: Transverse distance between the first ASF
T2: Transverse distance between the second ASF
P1: Anterior pedicle height
P2: Distance between the inferior border of the first ASF and the superior border of the second ASF
S1: Height of the S1 vertebra body
S2: Height of the S2 vertebra body
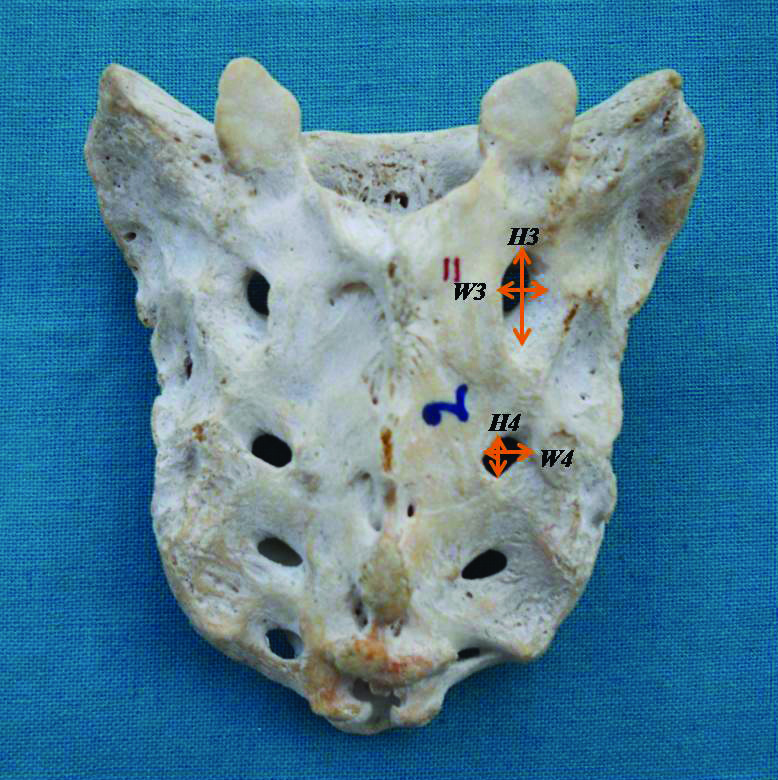
Posterior surface of sacrum showing linear parameters.
H3: Height of first posterior sacral foramina
W3: Width of first posterior sacral foramina
H4: Height of second posterior sacral foramina
W4: Width of second posterior sacral foramina
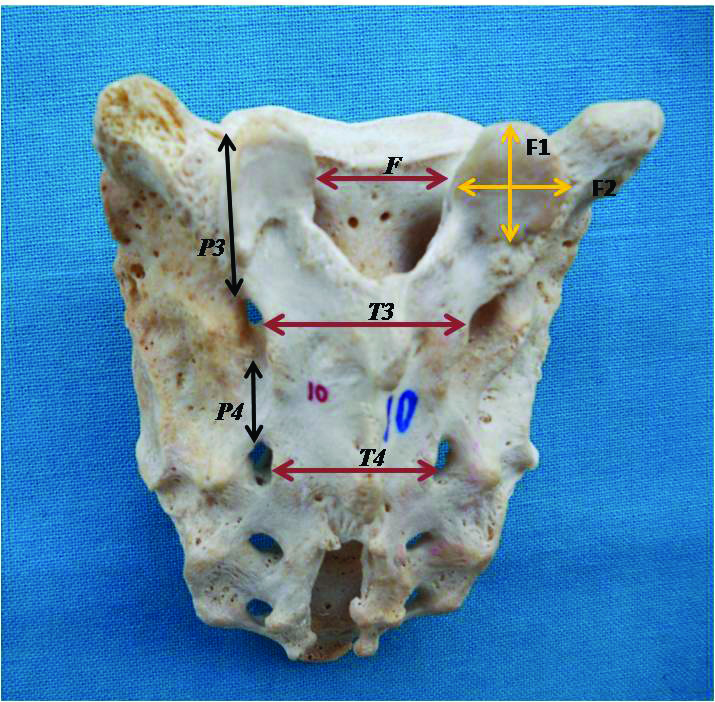
Posterior surface of sacrum showing linear parameters.
P3: Posterior pedicle height
P4: Distance between the inferior border of the first PSF and the superior border of the second PSF
T3: Transverse distance between the first PSF
T4: Transverse distance between the second PSF
F: Distance between the S1 facet joint
F1: Height of S1 facet joint
F2: Width of S1 facet joint
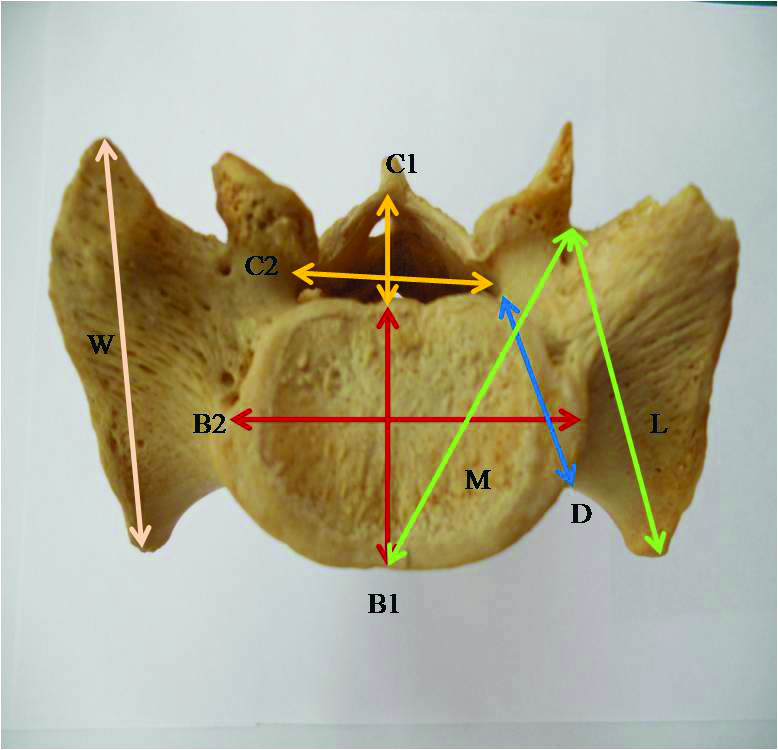
Superior surface of sacrum showing linear parameters.
C1: Sagittal diameter of the spinal canal
C2: Transverse diameter of the spinal canal
B1: S1 vertebral body APD
B2: S1 vertebral body TD
D: S1 pedicle depth
M: Anteromedial STD
L: Anterolateral STD
W: Sacral wing depth
Height of first Anterior Sacral Foramina (ASF): Maximum vertical distance between the superior and inferior border of first anterior sacral foramen.
Width of first ASF: Maximum transverse distance between the medial and lateral border of first anterior sacral foramen.
Height of first Posterior Sacral Foramina (PSF): Maximum vertical distance between the superior and inferior border of first posterior sacral foramen.
Width of first PSF: Maximum transverse distance between the medial and lateral border of first posterior sacral foramen.
Height of second ASF: Maximum vertical distance between the superior and inferior border of second anterior sacral foramen.
Width of second ASF: Maximum transverse distance between the medial and lateral border of second anterior sacral foramen.
Height of second PSF: Maximum vertical distance between the superior and inferior border of second posterior sacral foramen.
Width of second PSF: Maximum transverse distance between the medial and lateral border of second posterior sacral foramen.
Transverse distance between the first ASF: Measured as the transverse distance between the two points on the medial border of first anterior sacral foramina at the level of first transverse fusion line between the first anterior sacral foramina.
Transverse distance between the second ASF: Measured as the transverse distance between two points on the medial border of second anterior sacral foramina at the level of second transverse fusion line between the second anterior sacral foramina.
Transverse distance between the first PSF: Measured as the transverse distance between the two points marked on the medial border of first posterior sacral foramina at the level of first articular tubercle.
Transverse distance between the second PSF: Measured as the transverse distance between two points marked on the medial border of second posterior sacral foramina at the level of second articular tubercle.
Anterior pedicle height: The vertical distance between the superior border of first anterior sacral foramen and the superior border of the sacrum.
Distance between the inferior border of the first ASF and the superior border of the second ASF: The vertical distance between the inferior border of first anterior sacral foramen and the superior border of the second anterior sacral foramen.
Posterior pedicle height: Measured as the vertical distance between the superior border of first posterior sacral foramen and the superior border of the sacrum.
Distance between the inferior border of the first PSF and the superior border of the second PSF: Measured as the vertical distance between the inferior border of first posterior sacral foramen and the superior border of the second posterior sacral foramen.
Anteromedial Screw Trajectory Distance (STD): The distance between the infero-lateral aspect of S1 facet joint and the antero-medial point of S1 vertebra (middle of the promontory).
Anterolateral Screw Trajectory Distance (STD): The distance between the infero-lateral aspect of S1 facet joint and the junction of anterior and lateral border of the ala of sacrum.
S1 pedicle depth: Measured as the minimal distance between the anterior and posterior borders of the pedicle.
Sacral wing depth: Measured as the maximum antero-posterior distance between the most posterior point of the ala of sacrum and a point on the anterior surface of the ala.
Height of S1 facet joint: The maximum vertical distance between the superior and inferior border of S1 facet.
Width of S1 facet joint: Measured as the maximum transverse distance between the medial and lateral borders of S1 facet.
Distance between the S1 facet joints: The maximum transverse distance between the medial borders of S1 facets.
S1 vertebral body Antero-Posterior Diameter (APD): Measured as the midline antero-posterior distance between the anterior and posterior borders of S1 vertebral body.
S1 vertebral body Transverse Diameter (TD): Measured as the maximum transverse distance of S1 vertebral body.
Height of S1 vertebral body: The vertical distance between the middle of promontory and the middle of first transverse fusion line between the first anterior sacral foramina.
Height of S2 vertebral body: The vertical distance between the middle of first transverse fusion line between the first anterior sacral foramina and middle of second transverse fusion line between the second anterior sacral foramina.
Sagittal diameter of the spinal canal: Measured as the midline antero-posterior distance between the anterior and posterior borders of superior aperture of sacral canal.
Transverse diameter of the spinal canal: Measured as the maximum transverse distance of the superior aperture of sacral canal.
Superior surface of sacrum showing angular parameters.
1: S1 facet angle
2: Anteromedial STA
3: Anterolateral STA
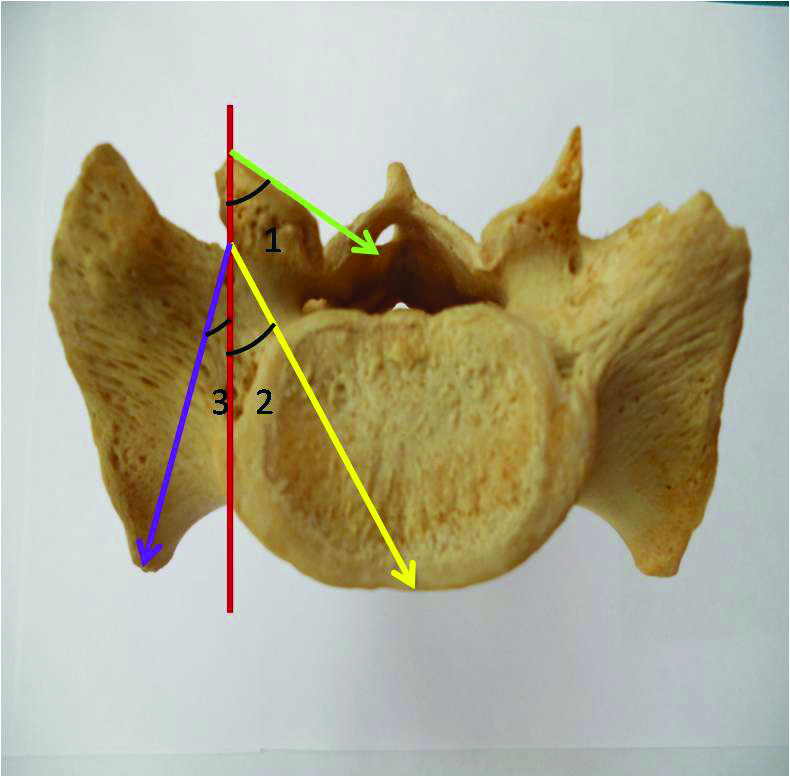
S1 facet angle: Measured as the angle formed between the articular surface of S1 facet and an antero-posterior line passing through the S1 pedicle entry point.
Anteromedial Screw Trajectory Angle (STA): Measured as the angle formed between an antero-posterior line passing through the S1 pedicle entry point and a line passing from the S1 pedicle entry point to the midpoint of promontory.
Anterolateral Screw Trajectory Angle (STA): Measured as the angle formed between antero-posterior line passing through the S1 pedicle entry point and a line passing from the S1 pedicle entry point to the junction of anterior and lateral border of the ala of sacrum.
Statistical Analysis
Statistical testing was conducted with the statistical package for the social science system version SPSS version 17.0. Results were expressed as mean±SD (standard deviation). The comparison of morphometric dimensions of the right and left sides was performed using Student’s t-test and p-value was calculated.
Results
Linear Parameters
The mean height and width of first ASF as well as height of the first PSF were comparable on both the sides but the width of the first PSF was found to be significantly greater on the right side. Furthermore, the height and width of the second ASF and second PSF were also analogous on both the sides. The height and width of the ASF were observed to be greater than the corresponding dimensions of the PSF. Although the transverse distances between the ASF were found to be lesser than the transverse distances between PSF [Table/Fig-6].
Morphometric measurements of sacral foramina (in mm).
| Parameters | Right | Left | Mean value | p-value |
|---|
| Height of first ASF | 12.95±1.65 | 12.99±1.59 | 12.97±1.03 | 0.702 |
| Width of first ASF | 12.28±1.69 | 12.18±1.80 | 12.23±1.63 | 0.40 |
| Height of first PSF | 10.40±2.75 | 10.32±2.67 | 10.36±2.63 | 0.47 |
| Width of first PSF | 7.81±1.54 | 7.51±1.41 | 7.66±1.37 | 0.005 |
| Height of second ASF | 12.75±1.85 | 12.95±1.84 | 12.85±1.76 | 0.056 |
| Width of second ASF | 13.11±2.05 | 13.15±2.15 | 13.13±2.01 | 0.77 |
| Height of second PSF | 7.03±1.56 | 7.06±1.56 | 7.05±1.47 | 0.80 |
| Width of second PSF | 7.34±1.49 | 7.27±1.47 | 7.30±1.39 | 0.49 |
| TD between 1st ASF | - | - | 30.10±3.19 | - |
| TD between 2nd ASF | - | - | 27.33±2.36 | - |
| TD between 1st PSF | - | - | 37.49±3.90 | - |
| TD between 2nd PSF | - | - | 30.47±3.18 | - |
Mean anterior pedicle height of the sacrum was 20.74±2.29 mm which was significantly greater on the left side. Mean posterior pedicle height was also observed to be slightly more on the left side. Distance between the first ASF and second ASF as well as the distance between the first PSF and second PSF were comparable on both the sides. Anteromedial STD was slightly larger on the right side whereas anterolateral STD was almost similar on both the sides. Likewise, S1 pedicle depth and S1 wing depth were also observed to be comparable on both the sides. Width of S1 facet joint was more on the right side, though the height of the S1 facet joint was analogous on both the sides [Table/Fig-7].
Morphometric measurements of sacrum (in mm).
| Parameters | Right | Left | Mean value | p-value |
|---|
| Anterior PedicleHeight | 20.40±2.39 | 21.07±2.43 | 20.74±2.29 | <0.001 |
| Distance between 1st ASF and 2nd ASF | 11.39±2.25 | 11.26±2.38 | 11.33±2.24 | 0.28 |
| Posterior Pedicle Height | 20.05±2.37 | 20.30±2.54 | 20.18±2.36 | 0.06 |
| Distance between 1st PSF and 2nd PSF | 14.22±2.37 | 14.14±2.34 | 14.18±2.29 | 0.43 |
| Anteromedial STD | 45.79±3.51 | 45.56±3.49 | 45.67±3.44 | 0.06 |
| Anterolateral STD | 44.62±3.96 | 44.57±3.79 | 44.60±3.77 | 0.79 |
| S1 pedicle depth | 23.43±2.45 | 23.53±2.45 | 23.48±2.36 | 0.42 |
| S1 wing Depth | 44.02±4.85 | 44.16±4.95 | 44.09±4.83 | 0.40 |
| Height of S1 facet joint | 14.78±1.69 | 14.69±1.68 | 14.73±1.57 | 0.46 |
| Width of S1 facet joint | 15.72±1.88 | 15.49±2.12 | 15.61±1.86 | 0.09 |
| Distance between S1facet joint | - | - | 25.46±3.53 | - |
| S1 body APD | - | - | 30.04±2.50 | - |
| S1 body TD | - | - | 47.64±4.98 | - |
| Height of S1body | - | - | 29.62±2.65 | - |
| Height of S2 body | - | - | 25.45±2.41 | - |
| Spinal canal SD | - | - | 12.99±3.11 | - |
| Spinal canal TD | - | - | 29.33±2.76 | - |
Angular Parameters
Mean S1 facet angle was 53.94±8.40 degree which was significantly larger on the left side. Anteromedial STA was also significantly greater on the left side but anterolateral STA was observed greater on the right side [Table/Fig-8].
Angular parameters of sacrum (in degrees).
| Parameters | Right | Left | Mean value | p-value |
|---|
| S1 facet angle | 52.55±9.02 | 55.32±9.16 | 53.94±8.40 | <0.001 |
| Anteromedial STA | 35.13±2.95 | 36.0±2.66 | 35.56±2.63 | <0.001 |
| Anterolateral STA | 32.18±3.09 | 30.67±2.75 | 31.42±2.75 | <0.001 |
Discussion
In the present study, we have attempted a comprehensive morphometric evaluation of sacra which can provide a reference database for designing customized sacral implants in Indian population. Such data also enables the comparison with other study populations and may serve as a tool for anthropological studies.
The dimensions (height and width) of the first and second ASF and PSF along with the transverse distances between these foramina were found to be less in our study as compared to Arman C et al., (Turkish population). In addition to importance in sacral instrumentation, these dimensions are crucial during electric stimulation of sacral nerve roots for modulating lower urinary tract neural reflexes in patients refractory to conventional treatment [Table/Fig-9,10] [3].
Comparison of morphometric measurements of sacrum between previous and present studies.
| Parameters (in mm) | Researchers |
|---|
| Arman C et al. [3], | Present study |
|---|
| 1st ASF | Height | Right | 13.58±2.16 | 12.95±1.65 |
| Left | 13.74±2.0 | 12.99±1.59 |
| Mean | 13.66±2.11 | 12.97±1.62 |
| Width | Right | 13.78±2.12 | 12.28±1.69 |
| Left | 14.13±2.1 | 12.18±1.80 |
| Mean | 13.95±2.12 | 12.23±1.74 |
| 1st PSF | Height | Right | 12.50±3.31 | 10.40±2.75 |
| Left | 12.44±3.01 | 10.32±2.67 |
| Mean | 12.47±3.16 | 10.36±2.70 |
| Width | Right | 8.14±1.97 | 7.81±1.54 |
| Left | 7.80±1.82 | 7.51±1.41 |
| Mean | 7.97±1.89 | 7.66±1.48 |
| 2ndASF | Height | Right | 13.48±2.26 | 12.75±1.85 |
| Left | 13.72±1.98 | 12.95±1.84 |
| Mean | 13.60±2.12 | 12.85±1.85 |
| Width | Right | 13.97±2.69 | 13.11±2.05 |
| Left | 14.46±2.27 | 13.15±2.15 |
| Mean | 14.22±2.48 | 13.13±2.09 |
| 2nd PSF | Height | Right | 7.62±1.54 | 7.03-1.56 |
| Left | 7.61±1.55 | 7.06-1.56 |
| Mean | 7.62+1.54 | 7.05-1.56 |
| Width | Right | 8.04±1.70 | 7.34±1.49 |
| Left | 7.81±1.78 | 7.27±1.47 |
| Mean | 7.92±1.74 | 7.30±1.48 |
Comparison of morphometric measurements of sacrum between previous and present studies.
| Parameters (in mm) | Researchers |
|---|
| Arman C et al. [3], | Present study |
|---|
| Transverse distance between 1st ASF | 30.48±2.78 | 30.10±3.19 |
| Transverse distance between 2nd ASF | 28.31±2.81 | 27.33±2.36 |
| Transverse distance between 1st PSF | 38.32±3.63 | 37.49±3.90 |
| Transverse distance between 2nd PSF | 31.62±3.27 | 30.47±3.18 |
Mean anterior pedicle height was found to be greater in the Indian population (20.74 mm) than the findings in Turkish, Greek, Chinese and Egyptian population [3,7-10]. But Ebraheim NA et al., in American population reported higher value (30.2 mm) than ours [11]. Furthermore, the distance between the first and second ASF was also observed to be greater in the Indian population. However, the posterior pedicle height and the distance between 1st and 2nd PSF were noted to be less in our study when compared to other investigators. Injury to sacral nerve roots associated with posterior sacral screw placement during internal fixation and fusion procedures can be minimised if the pedicle heights are adequate. With adequate anterior pedicle height, there are less chances of violation of neurovascular structures anterior to the sacrum. Thus, we emphasise that posterior sacral screw placement during internal fixation in Indian population, may be much safer due to greater anterior pedicle height as it would allow for manipulation of the screw and chances of breaching anterior neurovascular structures would be reduced [Table/Fig-11]. There are two important screw trajectories for posterior sacral fixation, including the anteromedial STD and the anterolateral STD. In the present study, mean anteromedial STD was found to be 45.67±3.49 mm. It was observed that in the present study, values were not in conformity with other studies. Similarly mean anterolateral STD as per the present study was 44.60±3.87 mm while Arman C et al., reported 50.30±3.57 mm. Thus, present study suggests a prudent measure to employ screws of shorter length during lumbo-sacral fixation, than those used in the Turkish population [Table/Fig-11].
Comparison of morphometric measurements of sacrum between previous and present studies.
| Parameters (in mm) | Researchers (Population) |
|---|
| Ebraheim NA et al., [11] | Arman C et al., [3] | Okutan O et al., [7] | Karachalios T et al., [8] | Liu W et al., [9] | Hassanein GH [10] | Present study |
|---|
| (American) | (Turkish) | (Turkish) | (Greek) | (Chinese) | (Egyptian) | (Indian) |
|---|
| Right | - | 14.88±2.38 | - | 19 | - | - | 20.40±2.39 |
| Anterior pedicle height | Left | - | 14.75±2.26 | - | 19.5 | - | - | 21.07±2.43 |
| Mean | 30.2 | 14.81±2.32 | 13.6 | 19.3 | 18.1±3.8 | 18.3±4.9 | 20.74±2.42 |
| Distance between inferior border of 1st ASF & superior border of 2nd ASF | Right | - | 10.79±2.38 | - | - | - | - | 11.39±2.25 |
| Left | - | 10.29±2.11 | - | - | - | - | 11.26±2.38 |
| Mean | - | 10.54±2.25 | - | - | - | - | 11.33±2.31 |
| Posterior pedicle height | Right | - | 20.74±2.50 | - | - | - | - | 20.05±2.37 |
| Left | - | 21.23±2.18 | - | - | - | - | 20.30±2.54 |
| Mean | 26.1 | 20.98±2.34 | - | - | 20.6±3.6 | 23.8±5.0 | 20.18±2.45 |
| Distance between inferior border of 1st PSF & superior border of 2nd PSF | Right | - | 15.92±2.05 | - | - | - | 14.22±2.37 |
| Left | - | 15.92±2.11 | - | - | - | - | 14.14±2.34 |
| Mean | - | 15.92±2.08 | - | - | - | - | 14.18±2.35 |
| Anteromedial STD | Right | - | 51.12±4.83 | - | - | - | - | 45.79±3.51 |
| Left | - | 51.26±4.72 | - | - | - | - | 45.56±3.49 |
| Mean | - | 51.19±4.77 | - | - | - | 52.3±5.2 | 45.67±3.49 |
| Anterolateral STD | Right | - | 50.13±3.63 | - | - | - | - | 44.62±3.96 |
| Left | - | 50.46±3.51 | - | - | - | - | 44.57±3.79 |
| Mean | - | 50.30±3.57 | - | - | - | - | 44.60±3.87 |
The mean S1 pedicle depth in present study was found to be 23.48±2.44 mm, while other researchers reported variable findings. Mean sacral wing depth was 44.09±4.89 mm, which is less than values obtained by Arman C et al., (53.90±4.39 mm). In the present study, findings do not corroborate with other researchers due to different populations under consideration and emphasise on the fact that Indian sacra are smaller in size, hence screws employed during lumbo-sacral fixation should be tailor made for Indian population [Table/Fig-12].
Comparison of morphometric measurements of sacrum between previous and present studies.
| Parameters (in mm) | Researchers (Population) |
|---|
| Ebraheim NA et al., [11] (American) | Arman C et al., [3] (Turkish) | Okutan O et al., [7] (Turkish) | Karachalios T et al., [8] (Greek) | Hassanein GH [10] (Egyptian) | Present study (Indian) |
|---|
| S1 pedicle depth | Right | | 24.69±3.92 | - | 18.2 | | 23.43±2.45 |
| Left | - | 24.60±3.75 | - | 18.2 | - | 23.53±2.45 |
| Mean | 27.8 | 24.65±3.84 | 22.4 | 18.2 | 29.9±5.3 | 23.48±2.44 |
| Sacral wing depth | Right | - | 53.88±4.65 | - | - | - | 44.02±4.85 |
| Left | - | 53.92±4.12 | - | - | - | 44.16±4.95 |
| Mean | 45.8 | 53.90±4.39 | - | - | - | 44.09±4.89 |
| S1 facet joint | | Right | - | 14.55±1.82 | - | - | - | 14.78±1.69 |
| Height | Left | - | 14.69±1.84 | - | - | - | 14.69±1.68 |
| Mean | - | 14.62±1.83 | - | - | - | 14.73±1.68 |
| Right | - | 16.44±2.20 | - | - | - | 15.72±1.88 |
| Width | Left | - | 16.30±2.08 | - | - | - | 15.49±2.12 |
| Mean | - | 16.37±2.14 | - | - | - | 15.61±2.0 |
| Distance between S1 facet joints | - | - | 25.68±3.80 | - | - | - | 25.46±3.53 |
| S1 vertebral body | A-P | - | - | 31.42±2.83 | - | 25.17 | - | 29.96±2.48 |
| diameter | Transverse | - | - | 49.40±5.89 | - | - | - | 46.98±5.12 |
| Height of vertebral body | S1 | - | - | 30.22±2.35 | - | 27.8 | - | 29.40±2.62 |
| S2 | - | 25.0 | 26.34±6.09 | - | 22.2 | - | 24.79±2.67 |
| Spinal canal diameter | Sagittal | - | - | 21.81±3.66 | - | - | 16.4±2.7 | 12.69±2.92 |
| Transverse | - | - | 31.31±3.16 | - | - | 29.4±3.9 | 29.62±2.72 |
The dimensions of S1 facet play a central role in weight distribution and in prevention of spondylolisthesis. The mean height and width of S1 facet joint were 14.73±1.68 mm and 15.61±2.0 mm respectively, distance between S1 facet joints was 25.46±3.53 mm and our findings corroborate with Arman C et al., [Table/Fig-12].
The dimensions of the S1 body play a vital role during posterior lumbar body fusion and anterior lumbar body fusion procedures [3]. Furthermore, the knowledge of anatomy of S2 vertebra is crucial during S2 lateral mass screw fixation which may intrude upon the iliac vessels or lumbosacral trunk while anchoring the anterior cortex of sacrum [12]. Arman C et al., reported higher values for the dimensions of S1 vertebra while Karachalios T et al., reported lower values than the present study. The height of S2 vertebral body was 24.79±2.67 mm according to present study and varied from the findings of other researchers [Table/Fig-12]. The sagittal diameter of spinal canal at superior aperture was found to be less than values obtained by other researchers and the transverse diameter was similar to study conducted by Hassanein GH. Reduced sacral spinal canal diameters may hinder lumbo-sacral procedures like thecaloscopy and play a crucial role in screw placement surgeries as the edge of the sacral canal forms the medial margin of the first sacral pedicle [10].
The STAs are of great significance as there is a risk of injury to neurovascular structures with poorly placed screws. Mirkovic S et al., detected that the internal iliac vein and the lumbosacral nerve trunk were the most probable injured structure in front of the sacrum during screw placement at 30 and 45 degrees angulation. Sigmoid colon, in spite of being adjacent to the S2 screw, was shielded by its mesentery. Additionally, S1 pedicle screw placement was detected to be least likely affecting the neurovascular structures [13]. In the present study, the mean S1 facet angle was greater (53.94°±9.17) than the finding of Arman C et al., (35.20°±9.62) [3]. Thus, the increased angulation of the facets in Indian population is a normal finding in all probability and it may be due to diverse population habits which affect weight distribution. In the present study estimated mean anteromedial STA to be 35.56°±2.83 mm which was more than that obtained by Arman C et al., (33.80°±4.34 mm) and anterolateral STA was almost similar in both studies. These above-mentioned angles are an important guide in pedicle screw placement at the sacrum and will allow characterisation of an optimal screw pathway in Indian population [Table/Fig-13].
Comparison of angular parameters of sacrum between previous and present studies.
| Parameters (in mm) | Researchers |
|---|
| Arman C et al. [3], | Present study |
|---|
| S1 facet angle | Right | 35.71°±9.5 | 52.55°±9.02 |
| Left | 34.70°±9.66 | 55.32°±9.16 |
| Mean | 35.20°±9.62 | 53.94±9.17 |
| Anteromedial STA | Right | 35.65°±4.73 | 35.13°±2.95 |
| Left | 31.95°±3.95 | 36.0°±2.66 |
| Mean | 33.80°±4.34 | 35.56°±2.83 |
| Anterolateral STA | Right | 32.65°±3.51 | 32.18°±3.09 |
| Left | 29.10°±3.14 | 30.67°±2.75 |
| Mean | 30.87°±3.32 | 31.42°±3.02 |
Ultimately, the other Indian researchers observed analogous results for screw trajectory distances and S1 vertebral body diameters but other parameters were observed to be variable [14-16]. [Table/Fig-14] illustrates the comparison between different Indian studies and provides a range of each parameter for Indians which should be considered during operative procedures of lumbosacral region.
Comparison of morphometric parametres of sacrum with other Indian studies.
| Parameters | Researchers |
|---|
| Padmavathi Devi SV et al., [14] | Sinha MB et al., [15] | Murugesan ND and Dharmalingham M [16] | Present study |
|---|
| Anterior pedicle height | 18.88 mm | - | 21.09 mm | 20.74 mm |
| Posterior pedicle height | - | 19.42 mm | 21.73 mm | 20.18 mm |
| Pedicle depth | - | 28.43 mm | - | 23.48 mm |
| Anteromedial STD | 45.11 mm | - | 46.05 mm | 45.67 mm |
| Anterolateral STD | 44.9 mm | - | - | 44.60 mm |
| S1 vertebral body APD | - | 29.47 mm | - | 29.96 mm |
| S1 vertebral body TD | - | 46.02 mm | - | 46.98 mm |
| Spinal Canal SD | - | 11.95 mm | - | 12.69 mm |
| Spinal canal TD | - | 27.77 mm | - | 29.62 mm |
| Anteromedial STA | 33.18° | - | 34.12° | 35.56° |
| Anterolateral STA | 26.95° | - | - | 31.42° |
Limitation
Present study was done on 108 dry adult human sacra due to limited availability in the institute. We propose further morphometric studies on large number of sacra to provide a reference database in Indian population.
Conclusion
The lesser dimensions of sacral foramina and larger anterior pedicle height in Indian population indicate a greater margin of safety for screw placement in this region. In spite of this observation, we propose the application of shorter length screws, as screw trajectory distances of the Indian sacra are lesser compared to other populations. The present comprehensive study yielded the morphometric characteristics of the Indian sacra which can minimize visceral and neurovascular injury during transpedicular and lateral mass sacral screw placement.
[1]. Standring S, Newell RLM, Gray’s Anatomy: The anatomical basis of clinical practice 2008 40th EditionSpainChurchill Livingstone Elsevier [Google Scholar]
[2]. Pal GP, Weight transmission through the sacrum in manJ Anat 1989 162:09-17. [Google Scholar]
[3]. Arman C, Naderi S, Kiray A, Aksu FT, Yilmaz HS, Tetic S, The human sacrum and safe approaches for screw placementJournal of Clinical Neuroscience 2009 16(8):1046-49.10.1016/j.jocn.2008.07.08119442524 [Google Scholar] [CrossRef] [PubMed]
[4]. Ergur I, Akcali O, Kiray A, Kosay C, Tayefi H, Neurovascular risks of sacral screws with bicortical purchase: an anatomical studyEur Spine J 2007 16(9):1519-23.10.1007/s00586-007-0326-x17846804 [Google Scholar] [CrossRef] [PubMed]
[5]. Kwan MK, Jeffry A, Chan CY, Saw LB, A radiological evaluation of the morphometry and safety of S1, S2 and S2-ilium screws in the Asian population using three dimensional computed tomography scan: an analysis of 180 pelvisSurg Radiol Anat 2012 34(3):217-27.10.1007/s00276-011-0919-222194086 [Google Scholar] [CrossRef] [PubMed]
[6]. Liao SH, Tong RF, Tang M, Computer aided design and evaluation of new anatomic fixation system on entire pelvic model. 2009 SIAM/ACM Joint Conference on Geometric and Physical Modeling; 2009 Oct 4-9; San Francisco, California 2009 New York, USAACM:331-336.10.1145/1629255.1629299 [Google Scholar] [CrossRef]
[7]. Okutan O, Kaptanoglu E, Solaroglu I, Beskonakli E, Tekdemir I, Pedicle morphology of the first sacral vertebraNeuroanatomy 2003 2:16-19. [Google Scholar]
[8]. Karachalios T, Zibis AH, Zintzaras E, Bargiotas K, Karantanas AH, Malizos KN, An anatomical update on the morphologic variations of S1 and S2Orthopedics 2010 33(10):73310.3928/01477447-20100826-1220954663 [Google Scholar] [CrossRef] [PubMed]
[9]. Liu W, Du XR, Yang LH, Wang R, Zhang JZ, Kong XC, The treatment of lumbosacral transitional vertebra using sacroiliac screws: clinical anatomic surveyChinese Journal of Clinical Anatomy 2011 29(5):520-23. [Google Scholar]
[10]. Hassanein GH, Metric study of Egyptian sacrum for lumbo-sacral fixation proceduresClin Anat 2011 24(2):218-24.10.1002/ca.2108221322044 [Google Scholar] [CrossRef] [PubMed]
[11]. Ebraheim NA, Xu R, Biyani A, Nadaud MC, Morphologic considerations of the first sacral pedicle for iliosacral screw placementSpine 1997 22(8):841-46.10.1097/00007632-199704150-000029127914 [Google Scholar] [CrossRef] [PubMed]
[12]. Ebraheim NA, Lu J, Yang H, Heck BE, Yeasting RA, Anatomic considerations of the second sacral vertebra and dorsal screw placementSurg Radiol Anat 1997 19(6):353-57.10.1007/BF016285009479708 [Google Scholar] [CrossRef] [PubMed]
[13]. Mirkovic S, Abitbol JJ, Steinman J, Edwards CC, Schaffler M, Massie J, Anatomic consideration for sacral screw placementSpine 1991 16(6S):S289-94.10.1097/00007632-199106001-00022 [Google Scholar] [CrossRef]
[14]. Padmavathi Devi SV, Rajini T, Mokhasi V, Morphometry of the first sacral pedicle in South Indian populationInternational Journal of Current Research and Review 2014 6(13):38-44. [Google Scholar]
[15]. Sinha MB, Mrithunjay R, Soumitra T, Siddiqui AU, Morphometry of first pedicle of sacrum and its clinical relevanceInternational J of Healthcare & Biomedical Research 2013 1(4):234-40. [Google Scholar]
[16]. Murugesan ND, Dharmalingam M, First sacral pedicle–a morphometric analysisIndian Journal of Clinical Anatomy and Physiology 2016 3(1):30-33.10.5958/2394-2126.2016.00009.8 [Google Scholar] [CrossRef]