Current and future trends in dental education require students to achieve a diverse set of competencies which make educational methodologies more challenging, complex and multifaceted [1]. In addition, the educational system is going through a transition from a conventional teacher-centered to contemporary student-centered learning [2]. Thus, ensuring student’s satisfaction with learning is one of the biggest challenges for the instructors in dentistry [3]. To that end, understanding the preferred learning styles of students can be valuable for students as well as teachers and can provide insight to the instructors about areas where students can improve their learning [4]. Knowing students learning style can encourage educators modify teaching styles to align with students learning preferences to help them to better understand the subject materials. Pedagogical researchers observed that aligning educator’s teaching style with the student’s learning style has been shown to improve the understanding and recollection of information presented to the students [5]. In addition, matching the methods of information transfer with the preferred learning style can bring more students into the loop of more motivated and better-performing students [6].
Visual, aural, read/write and kinesthetic are four learning preferences proposed by Fleming N [7]. Visual (V) learners prefer using graphs, flow charts, poster, and models as means to receive information. Aural (A) learners choose to learn by listening through discussions, dialogue, lectures, and tutorials. Read/Write (R) learners prefer written words and texts in the form of lists, textbooks, handouts, lecture notes and glossaries. Kinesthetic learners (K) like to learn through practice and experimentation such as life examples, case studies, role play and field trip etc. [7].
The term “unimodal” is for those individuals who have a preference for a single learning style and “multimodal” for individuals with a preference for more than one learning style. In 2013, a study among 113 undergraduate medical students in Sri Lanka found that the majority of them (69%) were multimodal [4]. While in Saudi Arabia, it was found that almost 63-73% of preclinical medical students had multimodal learning style preferences [8,9]. Among dental students, however, the prevalence of multimodal learning style preferences ranged from 55-59% as reported in studies conducted in Riyadh [10-12].
Different life experiences, clinical and educational challenges can make it more difficult for instructors to encourage students to learn the subject in a particular way. Lack of time, perception and knowledge about learning styles and training preclude educators to include active learning strategies in their routine teaching practices [13,14]. Nonetheless, the students are more motivated and their academic performance is reported to improve when information presented to them is tailored according to their preferred learning styles [15]. The attainment of learning outcomes is related to the ways in which individuals approach a learning situation [16]. Even, the lifelong learning patterns of students are influenced by their learning styles [14].
It is important for dental education researchers, administrators, academicians and faculty to learn the preferred learning styles of their students. Moreover, the educators need to understand the diversified learning needs of their students and develop appropriate teaching interventions to garner more interest and provide the most conducive and productive educational environment for their students. Nevertheless, there is a dearth of evidence on the learning styles among dental students in the Eastern Province of Saudi Arabia. There is also lack of information about a relationship between the socioeconomic statuses of dental students with their learning style preferences in didactic settings. Therefore, the present study aimed to evaluate the influence of gender, class year, academic performance, and paternal socioeconomic status on learning style preferences among dental students.
Materials and Methods
Study Participants
This cross-sectional study was conducted in the College of Dentistry Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia. The study was conducted from September 2016 to Feb 2017. All male and female students from second-year to six-year of undergraduate dentistry program participated in the study by filling out the self-administered questionnaire. The hard copies of the questionnaire were distributed among 452 students who voluntarily participated in the study. The first-year students take only one-year preparatory program which does not include any medical or dental courses; therefore, they were excluded from the present study.
Data Collection Methods
The VARK questionnaire version 7.8 was used to collect data about the preferences of students for VARK learning methods [7]. The questionnaire included 16 questions and each question had four options. The respondents could choose more than one option for each question that best explains their preference. These questions classify the respondents according to their learning style preferences. Moreover, questions about gender, paternal income and education, year of study, and academic performance assessed through last year’ GPA were included in the instrument. The validity and reliability of the VARK questionnaire have been proven to be satisfactory. Validation of the questionnaire resulted in mean factor loading of 0.51 for Visual, 0.47 for Auditory, 0.50 for Read/write, and 0.41 for kinaesthetic factors. The reliability estimate for subscales of VARK included Visual (0.85), Auditory (0.82), Read/write (0.84) and kinesthetic (0.77) [17]. Ethical approval of the study (application # 2014003) was obtained from the Scientific Research Unit at the College of Dentistry. The students were informed about the purpose of the study and they were given sufficient time to ask questions if they had any ambiguity in the questionnaire or query about the study. The completion of the questionnaire by the students implied their consent for the study.
Variable Description
In the present study, VARK learning style preferences were dependent variables, and gender, paternal education and income, academic performance represented by GPA, year of study, were independent variables.
Statistical Analysis
The descriptive statistical analysis was performed to display the proportions of students demonstrating different learning styles. The VARK questionnaire scoring chart was used to determine distribution of four categories of learning style preferences [7]. Kruskal Wallis H test was performed to assess the association of GPA with learning style preferences by comparing the GPA in different groups of students exhibiting various learning style preferences. Pearson’s chi-square test was conducted to observe differences in the proportions of learning styles between male and female students, students with different paternal income and education levels, and students with low and high GPA. Similarly, differences in learning styles of students in preclinical (second and third year) and clinical (fourth, fifth and sixth year) classes were evaluated using Pearson’s chi-square test. Statistical testing involved 0.05% level of significance. Statistical Package for Social Sciences (SPSS) software (IBM SPSS Statistics for Windows, Version 22. Armonk, NY: IBM Corp) was used to perform statistical analysis.
Results
Of the 452 questionnaires that were distributed, 389 were returned. The response rate was 86.06%. Male students were 181 (46.5%) while female students were 208 (53.5%). The age of students ranged from 19 to 23 years with mean age 20.42±0.99 years. Average last year’s GPA reported by students was 4.39±0.33 and it ranged from 3 to 5. About half of participants reported paternal income of ≥7000SAR and their fathers had university education [Table/Fig-1]. The survey results revealed that (76%) of dental students preferred unimodal learning style, of which (18.8%) chose Visual (V), (18.5%) selected Aural (A), (14.7%) indicated read/write (R) and (23.7%) preferred Kinesthetic (K) [Table/Fig-2].
Demographic information of study participants.
| Characteristics | N (%) |
|---|
| Gender |
|---|
| Male | 181 (46.5) |
| Female | 208 (53.5) |
| Academic year |
|---|
| Preclinical | 191 (49.1) |
| Clinical | 198 (50.9) |
| Paternal income |
|---|
| < 7,000 SR* | 27 (6.9) |
| 7,000-15,000 SR | 83 (21.3) |
| > 15,000 SR | 113 (29) |
| Do not know/not sure | 166 (42.7) |
| Paternal education |
|---|
| No formal schooling | 26 (6.7) |
| Primary school education | 23 (5.9) |
| Secondary school education | 41 (10.5) |
| High school education | 109 (28.0) |
| Undergraduate degree | 115 (29.6) |
| Graduate | 75 (19.3) |
| Age (mean±SD) | 20.42±0.994 |
| GPA (mean±SD) | 4.39 (0.33) |
* 1 US dollar is equivalent to SR 3.75
GPA: Grade point average
Distribution of learning style preferences among students.
| Learning style preferences | N (%) |
|---|
| Visual (V) | 73 (18.8) |
| Aural (A) | 72 (18.5) |
| Read/write (R) | 57 (14.7) |
| Kinesthetic (K) | 92 (23.7) |
| Visual and Aural (VA) | 11 (2.82) |
| Visual and Read/write (VR) | 2 (0.05) |
| Visual and Kinesthetic (VK) | 27 (6.94) |
| Aural and Read/write (AR) | 6 (1.5) |
| Aural and Kinesthetic (AK) | 20 (5.14) |
| Read/write and Kinesthetic (RK) | 7 (1.79) |
| Visual, Aural and Read/write (VAR) | 2 (0.05) |
| Visual, Aural and Kinesthetic (VAK) | 8 (2.05) |
| Visual, Read/write, and Kinesthetic (VRK) | 5 (1.28) |
| Aural, Read/write, and Kinesthetic (ARK) | 3 (0.07) |
| Visual, Aural, Read/write and kinesthetic (VARK) | 4 (1.02) |
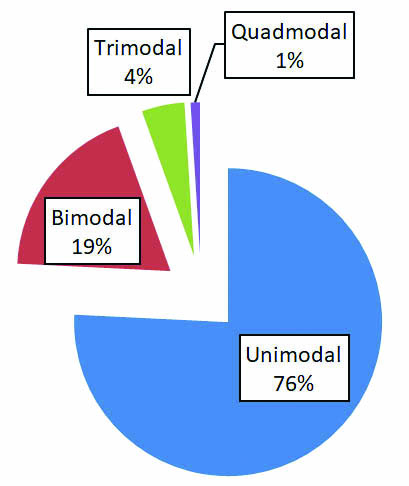
The [Table/Fig-3] shows the percentages of students (24%) who preferred more than one learning style (multimodal). Of which, (19%) preferred two learning style called bimodal (VA, VR, VK, AR, AK, RK), (4%) preferred three modes called tri-modal (VAR, VAK, VRK, ARK) and only (1%) students preferred all four modes as their learning style which is called quad-modal (VARK).
Distribution of students’ learning style preferences.
Among male students, the most preferred learning style was multimodal (29.3%), followed by Kinesthetic (K) (24.9%) and Aural (A) (17.1%). While among the female students, the most preferred learning styles were Kinesthetic (K) (22.6%) and Visual (V) (22.6%), followed by multimodal (20.2%). However, no significant association was found between male and female genders regarding their preferences for learning style (p=0.119) [Table/Fig-4].
Association of students’ learning style preferences with independent variables.
| Variables | Learning style preferences | p-value | Test |
|---|
| Visual N (%) | Aural N (%) | Read/write N (%) | Kinesthetic N (%) | Multimodal N (%) | |
|---|
| Gender |
|---|
| Male | 26 (14.4) | 31 (17.1) | 26 (14.4) | 45 (24.9) | 53 (29.3) | 0.119 | χ2 test |
| Female | 47 (22.6) | 41 (19.7) | 31 (14.9) | 47 (22.6) | 42 (20.2) |
| Academic year |
|---|
| Preclinical year | 25 (13.1) | 43 (22.5) | 27 (14.1) | 47 (24.6) | 49 (25.7) | 0.038* | χ2 test |
| Clinical year | 48 (24.2) | 29 (14.6) | 30 (15.2) | 45 (22.7) | 46 (23.2) |
| Paternal education |
|---|
| No schooling | 3 (11.5) | 5 (19.2) | 5 (19.2) | 3 (11.5) | 10 (38.5) | 0.412 | χ2 test |
| School education | 31 (17.9) | 33 (19.1) | 21 (12.1) | 48 (27.7) | 40 (23.1) |
| University education | 39 (20.5) | 34 (17.9) | 31 (16.3) | 41 (21.6) | 45(23.7) |
| Paternal income |
|---|
| <7000 SR | 4 (14.8) | 2 (7.4) | 5 (18.5) | 7 (25.9) | 9 (33.3) | 0.866 | χ2 test |
| 7000-15000 SR | 16 (19.3) | 9 (10.8) | 13 (15.7) | 26 (31.3) | 19 (22.9) |
| >15000 SR | 25 (22.1) | 16 (14.2) | 18 (15.9) | 26 (23) | 28 (24.8) |
| GPA |
|---|
| GPA ≤4 | 16 (22.9) | 8 (11.4) | 9 (12.9) | 23 (32.9) | 14 (20) | 0.136 | χ2 test |
| GPA >4 | 57 (17.9) | 64 (20.1) | 48 (15) | 69 (21.6) | 81 (25.4) |
| Mean ranks of GPA | 164.15 | 162.43 | 138.57 | 150.30 | 146.86 | 0.545 | Kruskal Wallis H test |
*Statistically significant
The analysis of a relationship between level of class year and learning styles showed, that multimodal (25.7%) was the most preferred learning style among pre-clinical students whereas clinical students preferred visual learning style (24.2%). The difference was statistically significant (p=0.038). The students with GPA ≤4 preferred kinesthetic learning style (32.9%) followed by visual (22.9%) whereas most of the students with GPA>4 (25.4%) learned through multimodal and kinesthetic (21.6%) and no significant relationship was found between the learning preferences and academic achievement [Table/Fig-4].
To examine the influence of socioeconomic factors on students learning style preferences, the students were classified into three groups based on their father’s income and education. Multimodal learning style was the most preferred (33.3%) among students who belonged to lower income group (<7,000 SAR) and with no paternal schooling background (38.5%). Kinesthetic (K) was the commonest preferred learning style among students from middle class (31.3%) and those with paternal school education (27.7%). Multimodal was the most common learning style among students with high paternal income (24.8%) and university education levels (23.7%). However, there were no significant relationships between learning style preferences and socioeconomic factors (p=0.412 for education; p=0.866 for income level) [Table/Fig-4].
Discussion
The findings of the present study can be utilised by the instructors and decision-makers in academia to create a conducive and congenial learning environment for students by incorporating appropriate teaching strategies while designing the courses. However, understanding of students learning style should not be used as the only information for their effective learning practices [18].
The present study found that unimodal learning style was the most preferred learning style and about one-quarter of dental students had multimodal style. These findings are close to the results of two studies of dental students conducted in Pakistan and one study of health sciences students in Australia [19-21]. Haq SM et al., conducted a study on medical and dental students and found that (69.3%) of dental students had a single learning style preference in Pakistan [20]. Similarly, Siddiqi KM et al., identified 52% of students exhibiting a single mode of learning [19]. Meehan-Andrews TA reported that 54% of students were unimodal learners who preferred single mode of information presentation [21]. In contrast, a Saudi Arabian study conducted in Riyadh reported that 58.4% of dental students preferred multimodal learning style and 41.6% had unimodal learning preference [11]. An earlier study in Riyadh pointed out that 59% of dental students preferred multi-modal learning style [12]. Another previous study of only female dental students in Riyadh found that 54.7% had a multi-modal preference [10]. These findings are contrary to our estimates. Similarly, Murphy RJ et al., showed that majority of dental students (56%) had a preference for multimodal learning in a dental institute in the USA [3]. It has been documented that learning preferences change over time and curricula can affect learning profile of students [22]. The students were subjected to a curriculum at King Saud University in two previous studies while different courses are taught to dental students at the College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam. These could explain the variations in learning style preferences among dental students in Saudi Arabia.
It has also been found that kinesthetic mode is the significant predictor of academic performance [23]. Kinesthetic learners obtain information by using all senses such as touch, sight, hearing, taste and smell etc., and field trips, practical sessions, hands-on computing experience, and case studies are best ways for them to take in information [7]. Dental students in the present study showed a strong preference for Kinesthetic (K) learning style which is consistent with the findings of previous studies reporting similar results [11,19,20]. It is quite possible that students from both clinical and pre-clinical classes in this study were exposed to a variety of teaching and learning methods in didactic and clinical courses and consequently, they were adapted to demonstrate kinesthetic learning.
The current body of evidence points to variations about the most common single learning style preference among students [3,8,12,24]. Aural learning preference was the most prevalent unimodal learning style among first-year dental students reported by Al-Saud [12]. Among medical students, Nuzhat A et al., observed aural as the dominant single learning style in Saudi Arabia [8]. Additionally, a study by Kaczmarek U et al., showed aural being the most common unimodal learning style among dental students in Poland [24]. Murphy RJ et al., found that dental students mostly preferred read/write learning as single mode followed by visual style in the U.S. [3].
It was expected that students in the preclinical class might have different learning styles than those in clinical years. The comparison of learning preferences between pre-clinical and clinical students revealed significant differences in the present study. The students in preclinical years demonstrated predominantly multimodal learning preference while visual was the most prevalent learning mode among students in clinical years. This disagrees with the findings of two previous studies which identified no significant differences in students’ responses from first year to final year of the undergraduate program [4,11]. The possible explanation for this could be that learning styles change with passage of time and so does the academic environment that influences the learning [22].
In the present study, both male and female students strongly preferred unimodal learning style (V, A, R or K). Upon further analysis of learning styles, slight variations were noted in male and female students. Learning preferences of male students were toward multimodal while kinesthetic was strongly preferred by females; however, these findings were not statistically significant. This is in agreement with the findings of many studies where no differences were observed in the learning style preferences between male and female students [3,12,25,26]. On the other hand, Wehrwein EA et al., reported significant gender differences where major fraction of male students’ preferred multimodal compared with female students who predominantly preferred unimodal instructions (kinesthetic) [27].
Lynch TG et al., reported the existence of a relationship between learning style and academic performance in medical students [28]. Al-Saud also investigated an association between dental students’ last year GPA (a proxy for academic achievement) and their learning style preference and found that students with low GPA demonstrated unimodal learning style whereas multimodal preference was observed among students with high GPA [12]. These findings are fairly in line with present results where the students with higher academic performance (GPA >4) had multimodal learning style preferences, and kinesthetic was the most prevalent learning style among students with low GPA (≤4), although there were no significant differences.
Socioeconomic status (SES) factors have been shown to be associated with physical, psychological, personal and professional enrichment in medical students [29]. It was also found that SES is associated with the academic performance of students evaluated by the grades obtained in previous years [30]. The influence of paternal SES on learning style preferences was not previously explored in dental students. The present study attempted to investigate an association between learning style preferences and paternal education and income. Different learning styles were observed among students with varying levels of paternal educational attainment and levels of income. However, statistically significant differences were not found.
Limitation
The present study provided meaningful contributions that can be utilised to improve student learning experience by understanding their preferred learning styles in dentistry. However, data were collected from a single dental college; therefore, caution should be taken while generalising the findings to other dental colleges in Saudi Arabia. Paternal income and education were used to assess socioeconomic status as financial and educational status of the family is mostly determined by the father in the country. Regardless, data of mother’s level of education might influence the results. Moreover, data may be limited due to self-reporting of students particularly about GPA and socioeconomic status. In future, a prospective study should be planned to observe changes in learning style preferences over years. The evaluation of academic performance of students can also be evaluated after aligning teaching styles of instructors with learning style preferences of students.
Conclusion
The study found that most students had a unimodal learning style. Kinesthetic was the most common learning style preference. Students in clinical years demonstrated visual learning preference and multimodal was dominating learning style among preclinical year students and significant association was found between learning style preferences and class year. No gender differences were observed regarding learning styles. Similarly, no influence of GPA and paternal income and education on learning style preferences was found. The study findings can be used to improve the quality of teaching and learning for the students. The instructors should use a variety of teaching methods to match the learning styles of students to facilitate their learning. Students should be encouraged to learn their learning style preferences to make their learning process more efficient. The institutions can develop policies to emphasize on different teaching methods.
* 1 US dollar is equivalent to SR 3.75GPA: Grade point average
*Statistically significant