Wilms’ Tumour in an Adult Female Complicating Pregnancy: A Case Report
Imran A Khan1, Supriya Basu2, Dawood Khan3, Arpan Choudhary4, Shaheen Khan5
1 Senior Resident, Department of Urology, R.G. Kar Medical College and Hospital, Kolkata, West Bengal, India.
2 Professor, Department of Urology, R.G. Kar Medical College and Hospital, Kolkata, West Bengal, India.
3 Senior Resident, Department of Urology, R.G. Kar Medical College and Hospital, Kolkata, West Bengal, India.
4 Senior Resident, Department of Urology, R.G. Kar Medical College and Hospital, Kolkata, West Bengal, India.
5 Senior Resident, Department of Obstetrics and Gynaecology, Bharat Ratna Dr. Babasaheb Ambedkar Municipal General Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Imran A. Khan, Room No. 8, MEB Hostel, R.G. Kar Medical College Campus, Kolkata, West Bengal, India.
E-mail: imrankhan.doc@gmail.com
Wilms’ tumour, also known as nephroblastoma, is the most common malignant renal tumour in children but rare in adults with significant difference in symptomatology. Here, we report a case of 23-year-old second-gravida female with 22 weeks of gestation with Wilms’ tumour. Gadolinium-based contrast enhanced magnetic resonance imaging was used, which revealed a heterogeneous space-occupying lesion involving right kidney. The patient was planned for nephron sparing surgery, however after open retroperitoneal exploration, partial nephrectomy was performed. We concluded that Wilms’ tumour in pregnancy can be dealt safely with partial nephrectomy with a retroperitoneal approach.
Gadolinium-based imaging, Nephroblastoma, Nephron sparing surgery, Partial nephrectomy
Case Report
A 23-year-old second-gravida female with 22 weeks of pregnancy was referred to Urology Department with chief complain of painless haematuria and dull aching pain in the right flank, three days prior to presentation. The general examination revealed severe pallor, with no icterus and lymphadenopathy. Abdominal examination revealed a mass palpable in the right lumbar region and a gravid uterus of 22 weeks of gestation.
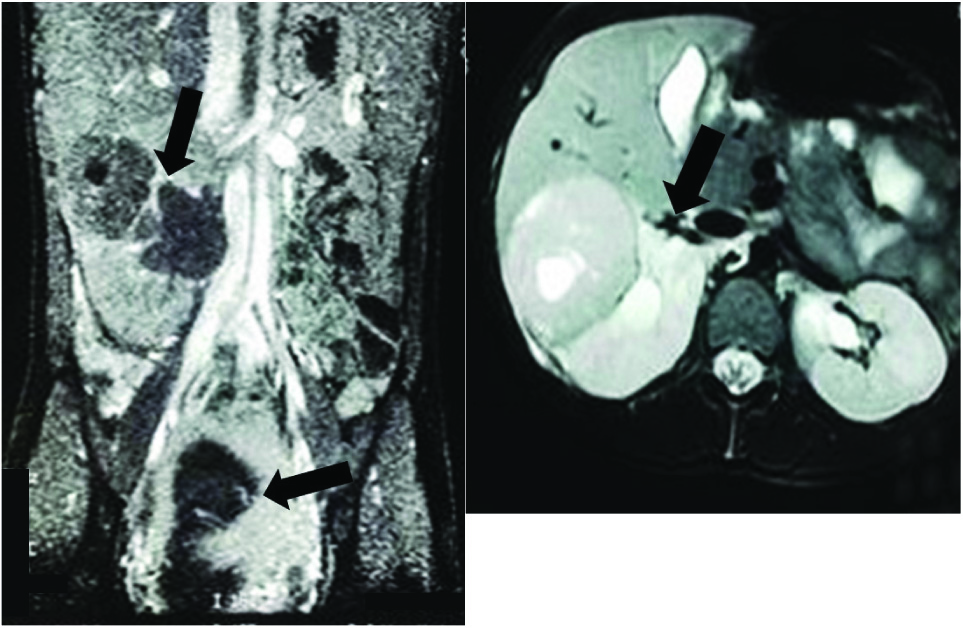
Complete blood count revealed severe anaemia {Haemoglobin: 6.9 gm/dL; Packed Cell Volume (PCV): 21.3%}. Liver and renal function tests were normal. Urine examination showed numerous red blood cells per high power field and urine culture was sterile. An ultrasound examination of the abdomen revealed an echogenic mass in the mid part of the right kidney measuring 5 cm × 5 cm and a single viable foetus. As Computed Tomography (CT) scan is contraindicated in pregnancy, gadolinium enhanced Magnetic Resonance Imaging (MRI) was taken after obtaining written informed consent. This revealed a heterogeneous space-occupying lesion involving right kidney (6.6 cm × 5.3 cm × 5.9 cm) with postcontrast enhancement and a normal functioning contralateral kidney [Table/Fig-1]. No retroperitoneal or pelvic lymphadenopathy was present and there was no involvement of renal vein and inferior vena cava. Renal nephrometry score of the tumour was calculated (R=1, E=2, N=3, A=a, L=2, total=8a).
MRI showing right-sided renal SOL with foetus in utero.
MRI: Magnetic resonance imaging; SOL: Space-occupying lesion
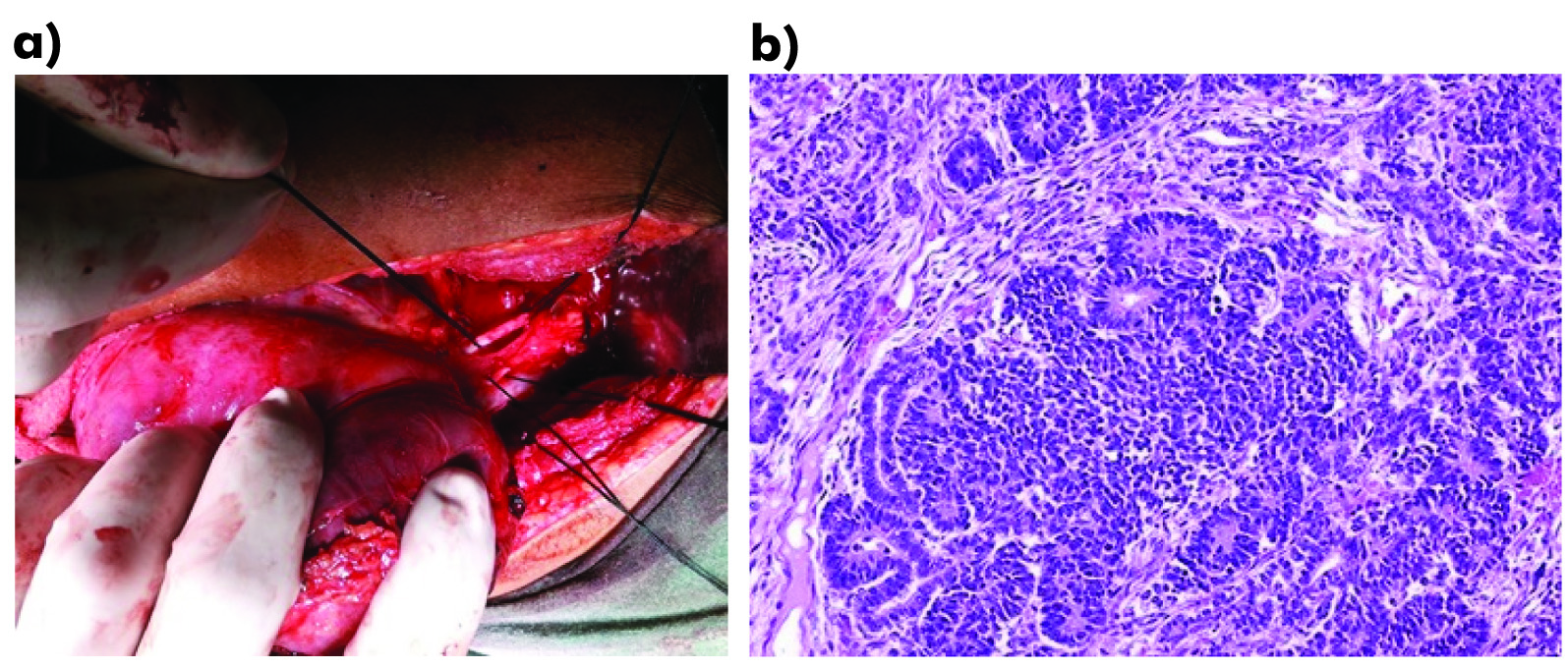
Considering the risk of disease progression (as the patient presented in early part of second trimester) and increase in haematuria, which could have further complicated pregnancy, decision to undertake the surgery was made. In consultation with a multidisciplinary team (urologists, nephrologist, gynaecologist, and radiologist), the patient was planned for Nephron Sparing Surgery (NSS). Partial nephrectomy was completed with a margin of approximate 1 cm using open retroperitoneal access [Table/Fig-2a]. Histopathologic examination of the mass revealed a triphasic Wilms’ tumour with predominance of blastemal element and favourable histology along with negative tumour margin [Table/Fig-2b]. The postoperative period was uneventful and the patient was discharged on seventh postoperative day under satisfactory condition with a viable foetus (ultrasound examination). She delivered a healthy child at term and until our last follow-up (one year postoperative) patient had no evidence of recurrence.
a) Intraoperative picture showing the renal SOL distinct from normal renal parenchyma and control of the renal pedicle during surgery; b) Triphasic Wilms’ tumour of favourable histology (Haematoxylin-eosin stain and magnification 100X).
SOL: Space-occupying lesion
Discussion
We report a case of an adult pregnant female presenting with renal mass, which came out to be Wilms’ tumour on histopathology and highlight the difficulties in management.
The preoperative diagnosis of an adult Wilms’ tumour is difficult as it has no typical clinical presentation, radiographic signs, or tumour markers that can distinguish it from a more common renal cell carcinoma. Although there are controversies on the use of gadolinium-based contrast agent during pregnancy, the only prospective study with 26 pregnant women, which evaluated the effect of antepartum gadolinium administration during first trimester, reported no adverse perinatal and neonatal outcomes [1]. American college of Obstetricians and Gynaecologists states that “given theoretical concerns and animal data, use of gadolinium enhanced MRI should be limited to situations in which the benefits clearly outweigh the risks [2]. Gadolinium enhanced MRI helps in preoperative staging, planning of surgery and assessing function of contralateral kidney, which are essential before embarking upon a surgery which might require removal of a kidney [2].
One of the most important considerations in the treatment of renal mass during pregnancy is the timing of the detection. It is recommended that, for renal cancer, nephrectomy must be done in the first or third trimester of gestation. Surgery should be postponed till 28th week of gestation if detected in second trimester, so that pulmonary maturation of the foetus would have occurred. In the present the patient was in early second trimester (22 weeks), hence considering the risk of disease progression it did not seemed prudent to do either medical termination or to wait till the third trimester. Therefore, the partial nephrectomy was planned after consultation with patient and family, after explaining the risk of premature labour and foetal loss.
Adult Wilms’ tumour is diagnosed based on the criteria given by Kilton L et al., which include: 1) the tumour under consideration should be a primary renal neoplasm; 2) presence of primitive blastemic spindle or round cell component; 3) formation of abortive or embryonal tubules or glomerular structures; 4) no area of tumour confirming the diagnosis of renal cell carcinoma; 5) pictorial confirmation of histology and 6) patient’s age >15 years [3]. As shown in [Table/Fig-3] [4-9], there are very limited cases of Wilms’ tumour during pregnancy. Maurer T et al., performed a radical nephrectomy [7] with adjuvant chemotherapy before and after delivering a healthy child. Rodrigues FA et al., reported a case in which the patient underwent radical nephrectomy during second trimester without any adjuvant therapy and was disease free at 24 months postpartum [8].
Summary of few previous cases [4-9]
| Author (year) | Country | Age (years) | Size of mass | Stage | Surgical procedure performed | Wilms’ tumour confirmed by |
|---|
| Wynn T et al., [4] | USA | 35 | 14 x 10 cm | NS | Right radical ureteronephrectomy | HPE (percutaneous needle biopsy) |
| Corapcioglu F et al. [5] | Turkey | 19 | NS | IIA | Left radical ureteronephrectomy | HPE |
| Rehman J et al., [6] | USA | 36 | 18 x 9 cm | II | Laparoscopic left radical nephrectomy | HPE |
| Maurer T et al., [7] | Germany | 31 | 8 x 6 x 4 cm | II | Right radical nephrectomy | HPE |
| Rodrigues FA et al., [8] | Brazil | 17 | 6 x 5 x 5 cm | I | Radical left nephrectomy and retroperitoneal lymphadenectomy | HPE |
| Byrd LM et al., [9] | UK | 31 | 10 x 11 cm | NS | Left nephrectomy (post-partum) | HPE |
| Present case | India | 23 | 6.6 x 5.3 x 5.9 cm | I | Partial nephrectomy | HPE |
HPE: Histopathological examination; NS: Not specified
As our patient showed most of the features of Very Low Risk Wilms Tumour (VLRWT; stage I favourable histology, <550 gm), we decided not to go for adjunctive chemotherapy in the patients, consistent with previous reports where VLRWT was successfully managed with surgery [10,11].
Conclusion
Wilms’ tumour in pregnancy can be dealt safely with partial nephrectomy with a retroperitoneal approach. The use of gadolinium-based imaging should be used judiciously during pregnancy where the benefits clearly outweigh the risks. Histology would guide the further course of management in these patients. Reporting of these unusual cases would help physicians to understand the biological nature of the disease and guide in the management and patient care.
HPE: Histopathological examination; NS: Not specified
[1]. De Santis M, Straface G, Cavaliere AF, Carducci B, Caruso A, Gadolinium periconceptional exposure: pregnancy and noenatal outcomeActa Obstet Gynecol Scand 2007 86:99-101./10.1080/0001634060080463917230297 [Google Scholar] [CrossRef] [PubMed]
[2]. A Watts, A Watts, A Watts, M Addy, Guidelines for diagnostic imaging during pregnancy and lactation. Committee opinion No. 656. American College of Obstetricians and GynecologistsObstet Gynecol 2016 127:e75-80.10.1097/AOG.000000000000131626942391 [Google Scholar] [CrossRef] [PubMed]
[3]. Kilton L, Matthews MJ, Cohen MH, Adult Wilms tumor: a report of prolonged survival and review of literatureJ Urol 1980 124(1):01-05.10.1016/S0022-5347(17)55264-7 [Google Scholar] [CrossRef]
[4]. Wynn T, Ruymann FB, King DR, Luquette M, Second pregnancy-associated Wilms tumor 16 years after the first oneMed Pediatr Oncol 2003 40:120-22.10.1002/mpo.1008612461798 [Google Scholar] [CrossRef] [PubMed]
[5]. Corapcioglu F, Dillioğlugil O, Sarper N, Akansel G, Calişkan N, Arisoy AE, Spinal cord compression and lung metastasis of Wilms’ tumor in a pregnant adolescentUrology 2004 64(4):807-10.10.1016/j.urology.2004.05.03215491732 [Google Scholar] [CrossRef] [PubMed]
[6]. Rehman J, Chughtai B, Guru K, Khan SA, Adler HL, Miller F, Wilm’s tumor during pregnancy: report of laparoscopic removal and review of literatureCan J Urol 2008 15:4180-83. [Google Scholar]
[7]. Maurer T, Zorn C, Klein E, Weirich G, Beer AJ, Gschwend JE, Multimodal tumor therapy in a 31-year-old pregnant woman with Wilms tumorUrol Int 2009 83:364-67.10.1159/00024168519829043 [Google Scholar] [CrossRef] [PubMed]
[8]. Rodrigues FA, Ribeiro EC, Maroccolo FR, Silva EA, Diaz FA, Adult Wilms tumor during gestational periodUrology 2009 73(1):929.e01-02.10.1016/j.urology.2008.05.01718722653 [Google Scholar] [CrossRef] [PubMed]
[9]. Byrd LM, Malay HK, Vause S, Management of a Wilms’ tumour, in a Jehovah’s Witness, 30+ weeks pregnantEur J Obstet Gynecol Reprod Biol 2006 126:129-31.10.1016/j.ejogrb.2005.10.03516356623 [Google Scholar] [CrossRef] [PubMed]
[10]. Shamberger RC, Anderson JR, Breslow NE, Perlman EJ, Beckwith JB, Ritchey ML, Long-term outcomes for infants with very low risk Wilms tumor treated with surgery alone in National Wilms Tumor Study-5Ann Surg 2010 251:555-58.10.1097/SLA.0b013e3181c0e5d720142733 [Google Scholar] [CrossRef] [PubMed]
[11]. Sredni ST, Gadd S, Huang CC, Breslow N, Grundy P, Green DM, Subsets of very low risk Wilms tumors show distinctive gene expression, histologic, and clinical featuresClin Cancer Res 2009 15:6800-09.10.1158/1078-0432.CCR-09-031219903788 [Google Scholar] [CrossRef] [PubMed]