Communication is increasingly understood to be a fundamental clinical skill critical to effective diagnosis and management, as well as to connect with patients on a cognitive and emotional level [1]. In addition, good communication has been found to be associated with better patient outcomes. These include patient satisfaction, adherence and even a decreased incidence of malpractice. This training generally begins in the pre-clinical years and extends into the clinical years, when increasing levels of sophistication is expected and direct experience with the patient can be taught. Evidence suggests that these skills deteriorate during the clinical years and teaching this skill is often neglected [2]. Considering that this aspect was not included in present day to day teaching and the increasing need of improvement in the doctor patient relationship through better communication, present university added this topic in the undergraduate curriculum.
For the last few years Communication Skills Training (CST) has been a part of the teaching. Modules for the first, second and third year MBBS students are made available by the university. Based on this, we prepared our own method of teaching and evaluation of the students, taking into consideration, the time constrains and other barriers which we may come across. The primary objective of the study was to assess the effectiveness of newly developed CST module, for the second year medical students for improvement in their knowledge, skills and attitude. The secondary objective was to identify the pitfalls and vital areas of implementation.
Materials and Methods
The present study was a medical education prospective observational study conducted by the Medical Education Unit of the Government Medical College, Pune, Maharashtra, India. The study was conducted over three year between June 2012 to December 2014.
The study was conducted on medical undergraduates in their second year of MBBS after Institutional Ethical Committee approval. Three such batches in the year 2012, 2013 and 2014 with an attendance of 165,189, and 187 respectively were considered. The inclusion criteria were those students who were present and participated in the pre-test and post-test both as well as feedback. Those who did not give the tests were excluded.
At the entry point, in the orientation given to first year undergraduate students, didactic lectures on basic communication skills, soft skills and etiquettes were included. This was just an introduction to sensitise the students. When the same batch entered the second year of MBBS and their clinical postings were to begin, a full day workshop based on the curriculum of the university was organised. The faculty was trained in the basics of medical education as well as communication skills and certified by the university. The faculty got together and prepared a blueprint for the programme. The lectures and role plays were discussed and prepared to the point avoiding an overlap between the topics. As per the curriculum, modules namely; rapport building, history taking, giving patient information, patient education, counselling and prescription writing were included. Duration of training was eight hours. The session began with a pre-test of 20 questions which were pre-validated with inputs from seniors, literature search, discussion with the faculty trained in the field of medical education and with those who had undergone training in communication skills. After the pre-test, the six modules were taught in the form of lectures lasting 20 minutes each, intercept with role plays by faculty thus making it interactive. At the end of the morning session the post-test was conducted. In the second session on the same day, the students were divided into six groups and further three subgroups. One facilitator was given charge of each group. Total 18 scenarios based on six modules along with check list (one for each subgroup) were distributed to students for performance in the form of role play. The scenarios were discussed and checklists prepared as per the essential elements communication checklist given by the Kalamazoo consensus statement [3]. This statement identifies seven key elements of communication in clinical situations namely building the relationship, an open discussion with the patient, gathering information, understanding the patient’s perspective, sharing information, reaching an agreement and providing a closure at the end. The relevance of each item in the checklist towards the said subject and scenario was assessed and discussed by the trained faculty with the students who were observers. The role plays were performed by each subgroup and the rest of students observed and assessed them with the help of the checklist provided (peer assessment). Thereafter, a written feedback was taken from the students regarding the overall training. The feedback form was prepared on each module, modified but based on a Likert’s scale, graded as poor, fair, average, good and excellent. It was anonymous and included open ended questions as well. Training assessment was done with the help of difference in the pre- test and post-test score assessment of psychomotor skill was done through direct observation of the performed role plays with the help of checklist assessed by peers.
Statistical Analysis
The data were entered in the excel sheet and analysed. The analysis was done in the form of percentages for evaluation of feedback. The pre- and post-test result was assessed for the number of respondents who showed progress or regress expressed in percentage. The respondents were those who gave the pre- and post-test both. The partial respondents were those who gave either the pre-test or post-test and complete non-respondents were those students who did not attempt both; again expressed in percentages. Student feedback was assessed in percentage.
Results
Demographic details were not comparable. Students who participated in pre- and post-test, namely the respondents were 121,149 and 167 in 2012, 2013 and 2014 respectively. The overall non-respondents gradually decreased from 26.67% in 2012; to 10.70% in 2014. These included the complete and partial non-respondents.
The results in the year 2012 revealed that there was a definite increase in the number of students between the score 81-90% in the post-test, a marginal fall in the 71-80% category, a definite fall in the 51-70%, with no student in the less than 50% category [Table/Fig-1,2]. Thus, 93 (76.86%) students showed improvement [Table/Fig-3].
Pre-test score in the second year MBBS students in three consecutive years.
| Marks (%) | % of students 2012 n=121 | % of students 2013 n=149 | % of students 2014 n=167 |
|---|
| 0-50 | 1.65 | 3.35 | 10.78 |
| 51-60 | 15.71 | 14.09 | 19.16 |
| 61-70 | 50.41 | 50.33 | 40.72 |
| 71-80 | 29.75 | 31.54 | 25.15 |
| 81-90 | 2.48 | 0.67 | 4.19 |
| 91-100 | 0 | 0 | 0 |
Post-test score of the second year MBBS students in three consecutive years.
| Marks (%) | % of students 2012 n=121 | % of students 2013 n=149 | % of students 2014 n=167 |
|---|
| 0-50 | 0 | 0 | 0 |
| 51-60 | 1.65 | 2.01 | 0 |
| 61-70 | 5.79 | 10.06 | 7.78 |
| 71-80 | 26.45 | 36.91 | 31.74 |
| 81-90 | 51.24 | 48.32 | 52.69 |
| 91-100 | 14.87 | 2.7 | 7.79 |
Post-test score of the second year MBBS students in three consecutive years.
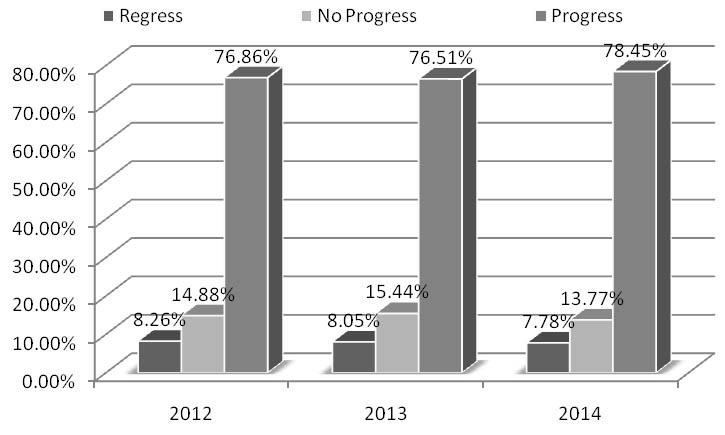
The results of pre and post-test in the year 2013 showed a definite increase in score in the in the 81-90% category with decline in the other categories. Here again those between 71-80% showed a marginal rise. [Table/Fig-1,2]. Thus, 113 (75.8%) students had progressed [Table/Fig-3].
The results of in the year 2014 showed that there was no student in the less than 60% group in the post-test. There was a marginal rise in the 71-80% category with more numbers in the 81-90% [Table/Fig-1,2]. Thus, 131 (78.45%) students had progressed [Table/Fig-3].
The number of students who participated in feedback increased by 7.6% from the year 2012 to 2014 [Table/Fig-4]. The feedback taken as per the students response on the questions asked over the three years showed that 80-90% students thought that objectives were well defined (good-excellent). Similarly 70-80% of students were happy with the speaker’s presentation skills (good-excellent).
Student feedback of second year MBBS students in three consecutive years.
| Year | Total number of students | Percentage feedback |
|---|
| 2012 | 165 | 81.82 (n=135) |
| 2013 | 189 | 80.95 (n=153) |
| 2014 | 189 | 89.42 (n=169) |
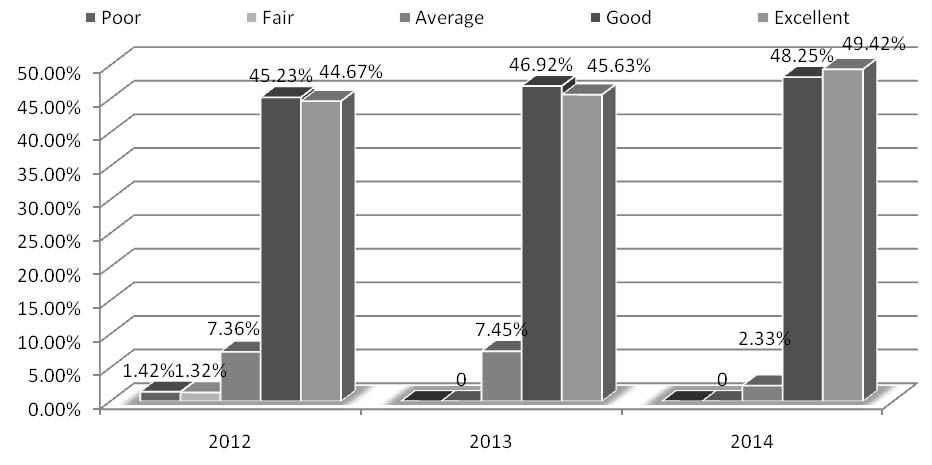
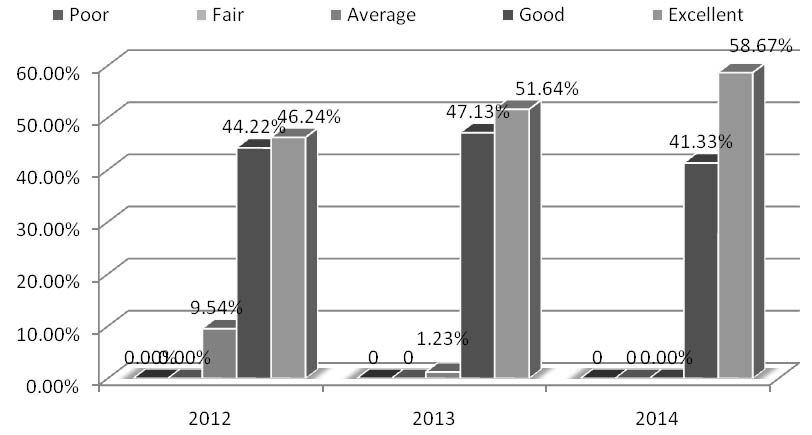
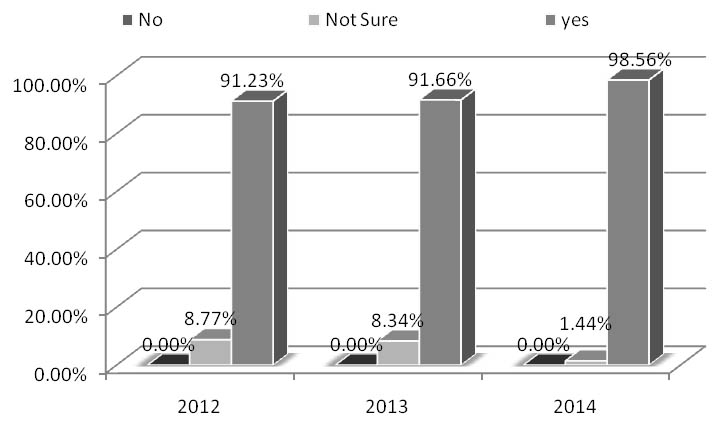
Speakers knowledge on the subject was found to be good to excellent according to 80-90% students and the number of students who thought it was average to poor declined from year 2012 to the year 2014 [Table/Fig-5]. Similarly, the lectures were more relevant to the subject; more than 90% gave a good to excellent feedback in the year 2014 as against 80-90% in the year 2012 [Table/Fig-6]. The number of students who assured that they would apply this knowledge on communication skills in their practice was >90%. The students who were “not sure”, declined from 8.77 to 1.44% from the year 2012 to the year 2014 [Table/Fig-7].
Feedback of second year MBBS students regarding-speakers subject knowledge.
Feedback of second year MBBS students regarding-relevance to your practice/profession.
Feedback of the second year MBBS students regarding-application of knowledge in future.
Discussion
An ability to communicate effectively with patients includes use of active listening skills, to gather and impart information, to empathise and develop a rapport. In addition, being professional and ethical is pivotal for a good medical practice [4]. A good communication with the patient decreases the distress and susceptibility of the patient to anxiety or depression [5-7]. Besides, a decrease in health care utilisation services related to inappropriate communication has recently been demonstrated [8]. These findings thus underline the importance of good communication techniques during consultations and thus the need to provide future medical doctors with the right kind of training in these skills. The first descriptions of communication training emerged in the early 1970s [9]. Most medical schools across the globe, more so the US and the UK have well established programmes on communication in their curriculum [10-14]. This subject was not included in regular teaching schedule. The realisation that improvement in the doctor patient relationship through better communication was the need of the day led to the addition of this topic in the undergraduate curriculum.
In one study, a well structured programme on effective communication skills was conducted on fourth year undergraduates; the communication skill attitude and standard patient satisfaction scale were evaluated using standardised patients. The scores showed improvement in the post-test [14]. In present study, the overall results for the three years showed a gradual progress, a more receptive student population and less reluctance towards attendance.
The latter could be because of better sensitisation over the years or compulsory attendance required by the university. Besides the student feedback too helped us in improvisation in present technique of presentation and delivery of knowledge as per expectations of stakeholders.
It has been found that fourth year medical students had a significantly more positive attitude towards communication skills training than first year suggesting repeated exposure to the training and actual clinical experiences [15].
In another study, a role play with simulated patient was used for training in communication skills approximately 96.5% students found this experience helpful [16]. The enthusiasm and learning through role play was apparent in present students. When specifically asked about the best part of the session the interaction in form of role plays was the answer. The overall feedback for the interactive lectures showed that overall rating for the sessions was good to excellent. The lectures interspersed with role play had a better impact on the students in the present study. A similar result was seen in a study where 90.30% students supported the conduction of role-play in the regular classes [17].
Limitation
Limitation of the present study was the time constraint. We could have had this session over two days. Besides this, we need to evaluate more number of batches to look into the drawbacks and further what changes need to be brought about in the existing module. Student participation though active in the study, reluctance was apparent. Besides this, the involvement of faculty in more numbers is expected through sensitisation programmes. Patient satisfaction with direct observation also needs to be studied.
Conclusion
Effective communication is a core competency for medical practitioners. A habit of good communication, when inculcated during formative years improves the attitude of the medical students towards the patient and definitely helps through future practice. Considering the above, this successful attempt at teaching communication skills to second year undergraduate medical students was made with the combined effort of the faculty as well as student participation. Student satisfaction as per the feedback was the key to present success.