Musculoskeletal neoplasms are one of the important entities in the present day clinical practice of orthopaedics which are most common around knee joint; Radiography followed by MRI is the most commonly used modality for evaluation [1]. USG is rapid, low cost, dynamic and easily available modality without radiation which can be used for evaluating tumours around knee joint; it is more useful in recurrent lesions with previous surgical implants, where other modalities produce artefacts; can able to differentiate cystic and solid lesions [2,3]. It is helpful in assessing local extent of the tumour. However, it is less frequently used for this purpose in India, because of most of tumours are bony lesions. Inspite of previous studies in literature, role of USG in knee tumours is not well described [1-4]. To the best of our knowledge, this is the first study in India which has compared the cross sectional imaging (CT/MRI) findings with USG and evaluated whether USG can be used as primary/ complementary investigation along with other imaging methods in patients with tumours and tumour like lesions around knee joint; mainly benign lesion like Giant Cell Tumour (GCT) and osteochondroma etc., were all referred in this study as tumour like lesions.
Materials and Methods
This was a prospective, descriptive study, conducted from January 2015 to June 2017 in the Department of Radiology and Imageology, Nizam’s Institute of Medical Sciences, Hyderabad, India. This study was approved by scientific and ethics committee of the institution and informed consent was taken from all patients. Subjects with clinical diagnosis/suspicion of tumours around knee joint based on clinical details, imaging and histopathological analysis were included; both bone tumours and soft tissue tumours were included irrespective of age and gender. Patients with traumatic, infective and inflammatory conditions around knee joint and Patients without histopathological diagnosis where histopathological examination was mandatory were excluded.
Methods
Plain radiograph and ultrasonographic examination was done for all patients. Plain radiograph of knee was done in minimum of two views (anteroposterior and lateral views) by computed radiography with standard methods. The following features were noted in radiographs: tumour location, margins, and zone of transition; periosteal reaction; mineralisation; size and number of lesions and soft-tissue component.
Ultrasonography was done for all patients, using linear probe of 5-12 MHz or curvilinear probe of 3-5 MHz, depending upon the size and location of lesion by Esatoe Mylab 40/60 machine. The following features were assessed: location, cortex, periosteum, adjacent neurovascular structures, soft tissue component, degree of ossification/calcification, joint space invasion, cartilaginous cap in case of osteochondroma, tumour vascularity with spectral wave analysis and regional lymph node involvement. Resistive Index (RI) was calculated in the lesions with vascularity by analysing pulse wave doppler wave forms taken from vascular areas of lesions and repeated for minimum three times.
Cross sectional imaging was done either with CT or MRI. Patients with contraindication to MRI (like metallic implants and defibrillator) were underwent CT (2/58); CT was obtained with MDCT 16 Slice Scanner Philips machine. MRI was obtained on 1.5 Tesla MRI machine -GE Signa‘using knee protocols (T1W, T2W, and STIR with/without Gadolinium enhanced sequences). Tumour location, size, number, matrix characterisation, extent of tumour, soft tissue component, enhancement pattern on contrast images, joint involvement, adjacent neurovascular invasion and regional spread were assessed in cross-sectional imaging. Staging of the tumours was also assessed with involvement of adjacent structures as well as distant metastasis for all modalities.
Final diagnosis was made in majority of patients by histopathological examination after surgical procedure/biopsy (56/59); In other three cases final diagnosis was made with pathognomic imaging features.
Statistical Analysis
Continuous variables were expressed as medians and ranges, and categorical variables were expressed as frequencies and percentages. Two-sided p-values less than 0.05 were considered to indicate statistical significance. All statistical analyses were performed using commercially available software (SPSS version 20, IBM). To assess for significant differences in resistive indices between benign and malignant lesions non parametric Mann-Whitney-Wilcoxon test was used. To identify the cut-off value of RI, receiver operator curve analysis was carried out.
Results
In total, 158 patients who presented to the orthopaedic department during the study period with complaints of swelling of knee were included. Based on clinical history of trauma, joint pain, fever, swelling of knee, restricted movements of knee, clinical examination of affected knee and radiography 58 patients with 59 lesions were included in this study.
Whereas 85 patients with traumatic, infective and inflammatory conditions were excluded; 15 patients without histopathological examination/classical imaging features were excluded.
The study population consisted of 58 patients (male-35; female-23) with mean age of 30.76 years (age range from 8 to 60 years); Total 59 lesions were identified and analysed from 58 patients and analysed where 46 (77.97%) were bone tumours and 13 (22.03%) were soft tissue tumours [Table/Fig-1]. One patient had two lesions (Ewing’s sarcoma of proximal tibia had metastatic lesion in distal femur).
Distribution of lesions (n=59).
| Bone tumours (n=46; 77.97%) | Soft tissue lesions (n=13; 22.03%) |
|---|
| Giant cell tumour | 21 (45.7%) | Backer’s cyst | 4 (30.7%) |
| Osteosarcoma | 13 (28.3%) | Synovial chondromatosis | 3 (23.1%) |
| Ewing’s sarcoma | 3 (6.5%) | Soft tissue sarcoma | 3 (23.1%) |
| Osteochondroma | 2 (4.3%) | Lipoma | 1 (7.6%) |
| Chondroblastoma | 2 (4.3%) | Angioleiomyoma | 1 (7.6%) |
| Metastasis | 2 (4.3%) | Neurofibroma | 1 (7.6%) |
| Aneurysmal bone cyst | 1 (2.2%) | |
| Lymphoma | 1 (2.2%) |
| Enchondroma | 1 (2.2%) |
Bone lesions
Bone lesions were more common than soft tissue lesions [Table/Fig-1]; benign lesions were more common than malignant lesions. Osteosarcoma was most common malignant bone lesion (n=13; 28.3%) and GCT was most common benign bone lesion (n=21; 45.7%).
Sonographic features of GCT and osteosarcoma are shown in [Table/Fig-2]. Among GCT, cortical break was noted in 90.5% cases whereas hypoechoic soft tissue component was noted in 95% of cases with 47.6% were showing medium sized soft tissue; 66.7% of GCT have RI <0.60 which indicates benign lesion; remaining 19% showed RI of >0.60 which may indicate local aggressiveness of lesions; Fluid-fluid level was seen in 9.5% of cases of GCT and 2 out of 21 had ABC component (2/21=9.5%).
Ultrasonographic features of giant cell tumour (n=21) and osteosarcoma (n=13).
| Features | Giant cell tumour | Osteosarcoma |
|---|
| Number of lesions (%) | Number of lesions (%) |
|---|
| Lysis | 21 (100%) | 10 (76.9%) |
| Cortical break |
| Present | 19 (90.5%) | 9 (69.2%) |
| Absent | 2 (9.5%) | 4 (30.8%) |
| Calcification | 0 (0%) | 12 (92.3%) |
| Ossification | 0 (0%) | 1 (7.7%) |
| Periosteal reaction | 3 (14.3%) | 13 (100%) |
| Soft Tissue Component |
| Appearance |
| Hyperechoic | 0 (0%) | 0 (0%) |
| Isoechoic | 1 (4.8%) | 0 (0%) |
| Hypoechoic | 20 (95.2%) | 0 (0%) |
| Mixed echoic | 0 (0%) | 13 (100%) |
| Size |
| Small (<2 cm) | 5 (23.8%) | 3 (23.1%) |
| Medium (2-5 cm) | 10 (47.6%) | 4 (30.8%) |
| Large (>5 cm) | 6 (28.6%) | 6 (46.1%) |
| Vascularity |
| Absent | 3 (14.3%) | 2 (9.5%) |
| Present | 18 (85.7%) | 11 (90.5%) |
| RI |
| <0.60 | 14 (66.7%) | 2 (15.4%) |
| >0.60 | 4 (19%) | 9 (69.2) |
| Cystic areas | 11 (52.4%) | 6 (46.1%) |
| Fluid level | 2 (9.5%) | 1 (7.7%) |
| Joint effusion | 5 (23.8%) | 5 (38.5%) |
| Neurovascular bundle involvement | 1 (4.7%) | 2 (15.4%) |
| Others (popliteal node involvement) | --- | 1 (7.7%) |
About 53.8% of osteosarcoma had lytic lesions with 69.2% had cortical break; USG demonstrated that 92.3% had ossification/calcification; All lesions showed mixed echoic soft tissue (100%) with 46.1% had large soft tissue component (>5 cm); among osteosarcomas, 90.5% of lesions were showing vascularity with 69.2% had RI > 0.60 and 15.4% of lesions had NVB involvement [Table/Fig-2].
Ultrasound was 95.6% sensitive for identifying periosteal reaction; Cortical thinning/break/fracture, soft tissue component, NVB involvement and joint effusion were identified in all cases (100% sensitivity) by USG and results were comparable with MRI [Table/Fig-2].
Cystic component and fluid-fluid levels (4/46)=100% demonstrated by USG and have high negative predictive value to assess ABC component in GCT; these features were also comparable to MRI [Table/Fig-2].
Among bone lesions, four lesions were not identified by USG because of intraosseous location; USG was comparable to CT and superior to MRI/radiography for assessing calcification. USG identified only 42 lesions all of which were differentiated as benign or malignant. Sensitivity of USG is 91.3% in comparison with cross-sectional imaging.
Among 46 lesions 11 lesions were avascular (23.9%); 66.7% of Ewing’s sarcoma, 15.4% of osteosarcoma and 14.3% of GCT are avascular on Doppler ultrasonography [Table/Fig-3].
Non vascular lesions on Doppler Ultrasonography.
| Lesions | Number | Percentage (%) |
|---|
| GCT* | 3 | 14.3 |
| Osteosarcoma | 2 | 15.4 |
| Ewing’s sarcoma | 2 | 66.7 |
| Chondroblastoma | 2 | 100 |
| Osteochondroma | 2 | 100 |
| Synovial chondromatosis | 3 | 100 |
| Backer’s cyst | 4 | 100 |
| Others | 5 | 45.4 |
*GCT: Giant cell tumour
Soft Tissue Lesions
Baker’s cyst was most common lesion (n=4; 30.7%), followed by synovial chondromatosis (n=3; 23.1%) and soft tissue sarcoma (n=3; 23.1%) as shown in [Table/Fig-1]. Most of the lesions were solid (53.9%) and 61.5% lesions had well defined margin; 53.9% lesions were showing vascularity with NVB bundle involvement in 15.4% of cases [Table/Fig-4]. Again USG was superior to MRI/radiography for assessing calcification, like bone lesions; Sensitivity of USG is 100 % in comparison with cross sectional imaging.
USG features of soft tissue lesions (n=13).
| Features | Number of lesions | Percentage (%) |
|---|
| Appearance |
| Cystic | 4 | 30.8 |
| Solid | 7 | 53.9 |
| Mixed | 2 | 15.3 |
| Margin |
| Well defined | 8 | 61.5 |
| Ill defined | 5 | 38.5 |
| Vascularity |
| Present |
| Minimal | 3 | 23.1 |
| Florid | 4 | 30.8 |
| Absent | 6 | 46.1 |
| RI |
| <0.60 | 2 | 15.4 |
| >0.60 | 2 | 15.4 |
| Calcifications |
| Present | 4 | 30.8 |
| Absent | 9 | 69.2 |
| Neurovascular bundle involvement | 2 | 15.4 |
Difference between benign and malignant lesions using Doppler USG: Doppler ultrasonogram was used to differentiate benign and malignant lesions by measuring RI; among 59 lesions, 36 lesions (61%) showed vascularity and 23 lesions (39%) did not show vascularity [Table/Fig-3]; resistive index was calculated for cases with vascularity; Non parametric Mann-Whitney Wilcoxon test was performed to evaluate the statistical significance of distribution of RI values among benign and malignant lesions [Table/Fig-5]. There was statistically significant difference in resistive index of benign and malignant lesions with Z score outside the 99% confidence limits.
Statistical analysis of RI values between benign and malignant Lesions.
| Index | Benign | Malignant | Uvalue | Wilcoxon W value | Z score | p value* |
|---|
| RI | Mean=0.71±0.12 | Mean=0.54±0.07 | 47.5 | 167.5 | -3.298 | 0.0009 |
*p value <0.05 is statistically significant.
Receiver Operator Curve (ROC) analysis was also done to identify cut off value with high sensitivity and specificity to differentiate benign and malignant lesions [Table/Fig-6].
Receiver operator curve for distribution of RI values between benign and malignant lesions.
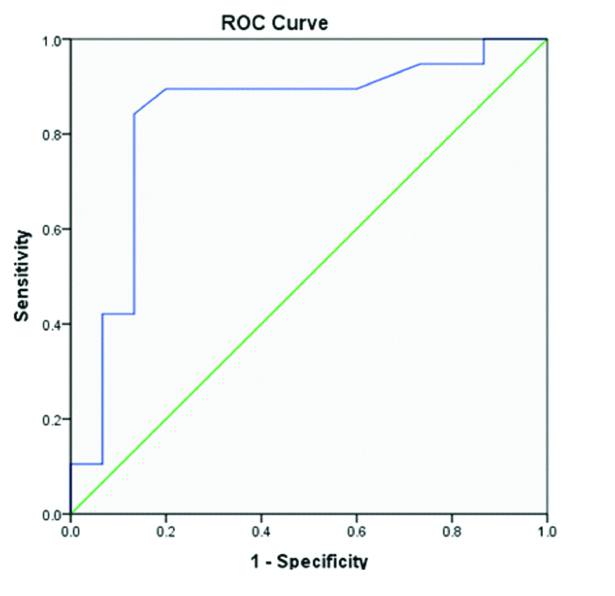
From the [Table/Fig-6], Doppler USG with resistive index had good accuracy in differentiating benign from malignant lesions with area under the curve was 0.833 and standard error of 0.079. From the curve we also derived a cut off value of 0.605 to differentiate benign from malignant lesions with high sensitivity (89.5%) and specificity (80.0%).
Discussion
Preoperative imaging for diagnosis and staging of musculoskeletal neoplasms is important for proper management [1]. So the choice of imaging method is crucial in radiological aspect. Role of ultrasonography which is less frequently used method for this purpose is studied and compared with other cross-sectional methods and radiography in this study [Table/Fig-7,8 and 9].
Comparison of radiography, ultrasonography and cross-sectional imaging (CT/MRI) for bone lesions.
| Parameters | Radiography | Ultrasonography | Cross sectional imaging (CT/MRI) |
|---|
| Number of identified lesions (n=46) | 46 (100%) | 42 (91.3%) | 46 (100%) |
| Periosteal reactions(n=23) | 22 (95.6%) | 22 (95.6%) | 23 (100%) |
| Cortical thinning/break/fracture (n=31) | 25 (80.6%) | 31 (100%) | 31 (100%) |
| Soft tissue component (n=40) | 27 (67.5%) | 40 (100%) | 37 (92.5%) |
| NVB involvement (n=4) | 0 (0%) | 4 (100%) | 4 (100%) |
| Joint effusion (n=12) | 4 (33.3%) | 12 (100%) | 12 (100%) |
| Calcification/ossification (n=12) | 11 (91.6%) | 12 (100%) | 11 (91.6)-for MRI only |
| Cystic component/fluid –fluid level (n=19) | 0 (0%) | 19 (100%) | 19 (100%) |
| Cartilagenous cap (n=2) | 0 (0%) | 2 (100%) | 2 (100%) |
| Popliteal node involvement (n=1) | 0 (0%) | 1 (100%) | 1 (100%) |
| Distant metastasis/ bone marrow involvement (n=11) | 0 (0%) | 0 (0%) | 11 (100%) |
| Differentiation of benign/malignant lesions (n=46) | 46 (100%) | 42 (91.3%) | 46 (100%) |
Comparison of radiography, ultrasonography and cross-sectional imaging (CT/MRI) for soft tissue lesions.
| Parameters | Radiography | Ultrasonography | Cross sectional imaging (CT/MRI) |
|---|
| Number of identified lesions (n=13) | 8 (61.5%) | 13 (100%) | 13 (100%) |
| NVB involvement (n=2) | 0 (0%) | 2 (100%) | 2 (100%) |
| Calcification (n=4) | 3 (75%) | 4 (100%) | 3 (75%)-for MRI only |
| Cystic/solid (n=13) | 0 (0%) | 13 (100%) | 13 (100%) |
| Differentiation of benign/malignant lesions (n=13) | 3 (23%) | 13 (100%) | 13 (100%) |
Comparison of USG with radiography and cross-sectional imaging.
| Modality/Parameter | Sensitivity | Specificity | PLR | NLR | Accuracy |
|---|
| USG | 93.2% | 97.9% | 46.1 | 0.07 | 96.2% |
| Radiography | 86.4% | 97.9% | 42.7 | 0.14 | 93.6% |
| Cross-sectional imaging | 98.3% | 98.9% | 97.3 | 0.02 | 98.7% |
*PLR-positive likelihood ratio
*NLR-negative likelihood ratio
Bone Lesions
USG showed abnormality in 42 cases (42/46) and less informative in 4/46 cases; (due to intraosseous location and purely sclerotic lesions); ultrasonic waves could not be transmitted beyond the bony cortex, so it is not diagnostic or less informative in intraosseous and purely/predominantly sclerotic lesions. Ultrasound was most sensitive (100%) and comparable to MRI to detect soft tissue changes [Table/Fig-10] associated with bone tumours (in contrast to radiography -50%) which is comparable with study of Saifuddin A et al., [2].
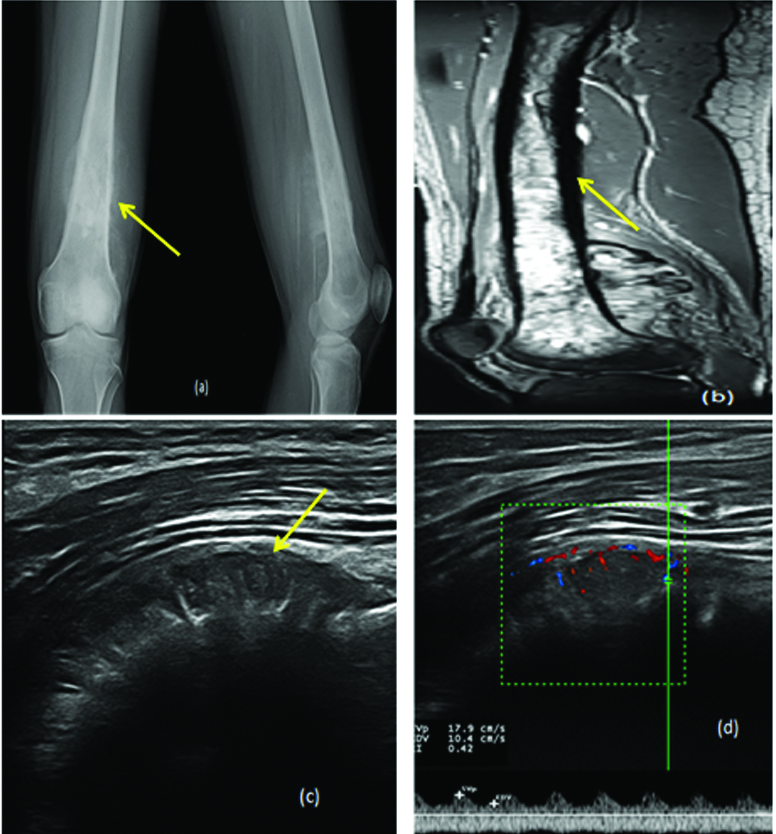
Osteosarcoma of lower end of femur in 17-year-old male. a) Plain radiograph showing mixed lytic sclerotic lesion with sunray type periosteal reaction and spiculation (arrows); b) Sagittal STIR MR image showing same lesion; c and d) USG showing same lesion with increased vascularity and RI of 0.42 (<0.60).
Demonstration of cystic areas with fluid-fluid level was comparable to cross sectional imaging and this was not demonstrated by radiography [Table/Fig-11]. This may be due to increased transmission of ultrasonic waves through cystic areas and haemorrhage also shown as mixed echoic cystic areas.
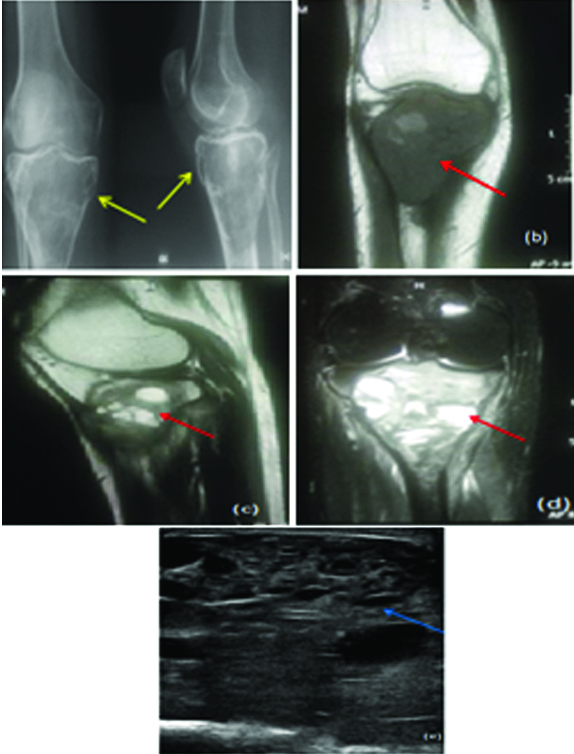
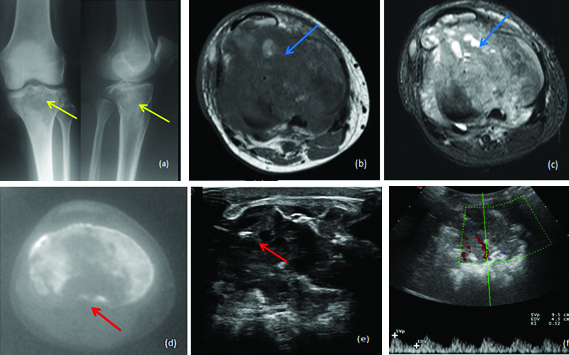
GCT of tibia with ABC component in a 25-year-old female. a) Radiograph showing expansile lytic lesion of tibia (yellow arrow); b, c and d) MRI showing same lesion with fluid-fluid level (red arrow) which is also demonstrated by e) USG (blue arrow).
USG is better than other modalities in recurrent lesions with surgical clips/fixators, because of the arifacts from implants degrading image quality in CT and MRI. In present study we encountered six recurrent lesions (mostly GCT), in which ultrasound demonstrated the lesion and associated features clearly. In this aspect Ultrasound was superior than MRI/CT [Table/Fig-12].
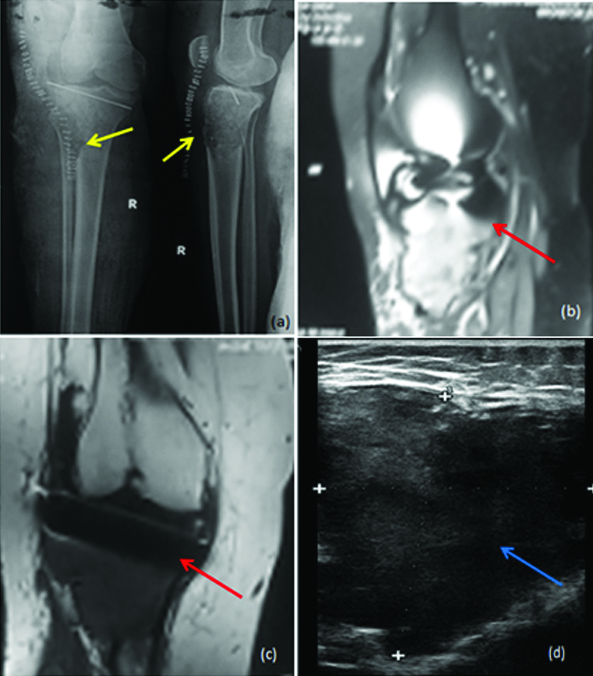
Recurrent tibial GCT in 35-year-old female. a) Plain radiograph showing lytic lesion in subarticular region of tibia with post-operative changes (yellow arrow); b) STIR coronal; c) T1 coronal MR images showing mainly artefacts (red arrow); d) USG showing large hypoechoic lesion clearly (blue arrow).
Demonstration of calcification by USG was comparable to CT and superior to MRI. In present study, one of the epiphyseal osteosarcoma was diagnosed as aggressive GCT due to epiphyseal location, increased vascularity of soft tissue component and low RI of 0.52, but finally histopathologically proven to be osteosarcoma of pleomorphic variety. In this case faint calcification in soft tissue is a clue to diagnosis identified on retrospective analysis and calcification is clearly demonstrated by USG and CT but not by MRI [Table/Fig-13]. In this study one case of osteosarcoma showed popliteal nodal metastasis, proved by pathological examination is demonstrated by MRI as well as USG [5,6].
Epiphyseal osteosarcoma of tibia in 26-year-old male, misdiagnosed as malignant GCT. a) Radiograph showing ill-defined lytic lesion in epiphysis of tibia (yellow arrow); b, c) MRI showing T1 hypo and STIR hyperintense lesion without new bone formation (blue arrow); d) CT and e,f) USG showing faint mineralisation (clue to diagnosis-red arrow) with low resistance flow on doppler USG (RI of 0.52).
Soft Tissue Lesions
Ultrasound is useful in all cases and identified all cases; USG is able to differentiate cystic and solid lesions, differentiate benign and malignant lesions (peritumoural oedema, necrosis, absent fat rim), plane of lesion, tissue of origin, NVB and joint involvement etc., and comparable with MRI [Table/Fig-8,9,14]. Calcifications were better demonstrated by USG than MRI (100% vs. 75% lesions) which is comparable to previous studies in literature [7,8].
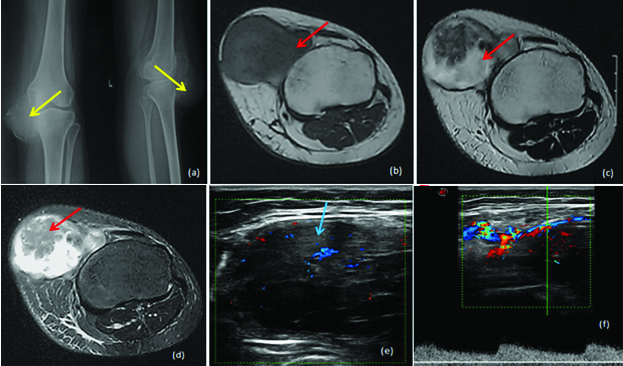
Spindle cell sarcoma of knee in 23-year-old female. a) Radiograph showing soft tissue swelling with calcification (yellow arrow); b) MRI showing T1 hypointense; c) T2; d) STIR hyperintense lesion on the lateral aspect infiltrating adjacent ligament (red arrow); e,f) USG showing ill-defined hypoechoic lesion (blue arrow) with low resistance flow (<0.60).
Difference between benign and malignant lesions: Statistically significant difference in resistive indices of benign and malignant lesions with Z score outside the 99% confidence limits and with p-value of 0.0009 (<0.05) which is comparable with study of Liu XM et al., however a study by Bodner G et al., did not showed any significant difference and comparable with a study by Belli P and Kaushik S [9-12]. Although Doppler USG has statistically good accuracy in differentiating benign and malignant lesions, only 61% (36/59) of lesions showed vascularity in present study; however doppler along with gray scale parameters was helpful in 88.1% (52/59) for diagnosis as well as differentiating benign from malignant lesions.
For staging of tumours, USG was useful only for assessing the local invasion into muscles, NVB and lymph node involvement; not useful to assess the bone marrow extension and distant metastasis into lung; In this study, one case of tibial Ewing’s sarcoma, showed metastasis into adjacent femur, which was demonstrated by all modalities. However, in this study no cases showed metastasis to liver or other abdominal organs, which can be demonstrated by USG.
To summarise, USG is >90% sensitive for periosteal reaction and 100% sensitive for cortical break, soft tissue component, NVB involvement and joint effusion in comparison to MRI; cystic component and fluid-fluid levels are better demonstrated by USG and have high negative predictive value to assess ABC component in GCT; Doppler USG and gray scale features like peritumoural oedema, necrosis, absent fat rim, size and heterogeneity of soft tissue component in bone lesions, invasion of adjacent joint, NVB and lymph node involvement were useful to differentiate benign and malignant lesions; very much useful in demonstrating lesions when fixators are in situ, it is better than CT to demonstrate cartilage cap of osteochondroma [13]; better than MRI to demonstrate calcifications. USG is useful for guiding biopsy/FNAC and assessing treatment response [14]; In this study for 6 cases, USG guided biopsy or FNAC was done and all were useful in diagnosis.
USG is not/less informative in purely sclerotic/intraosseous lesions without any cortical break and not useful to assess marrow involvement/distant metastasis especially to lung or other extra abdominal organs.
Limitation
There were limited numbers of subjects in present study. More number of subjects could have made the statistical analysis more accurate. One case of synovial osteochondromatosis and two cases of backer‘s cysts were not pathologically proven; However in these cases, imaging features were pathognomonic. Not all patients underwent uniform imaging protocols. Not all patients underwent image guided biopsy or followed up to assess treatment response. In Doppler ultrasonography we evaluated only resistive index; other indices (pulsality index, maximum and minimum velocities) were not evaluated. Similar type of study with inclusion of all doppler indices and large number of subjects is recommended.
Conclusion
To conclude, USG is useful in all types of soft tissue tumours whereas only useful in bone tumours with cortical discontinuity or superficial location with cortical thinning; less informative in intra-osseous lesions with intact cortex and sclerotic lesions. It is helpful to differentiate benign and malignant lesions by gray scale features and doppler parameters. It is very informative than any other modality in recurrent tumours with previous surgical implants producing artefacts; USG is useful and comparable to MRI in assessing local invasion, whereas less useful to evaluate distance metastasis and bone marrow involvement; It is useful to guide biopsy/Fine Needle Aspiration Cytology (FNAC) of the lesions. Therefore, USG can be used as initial as well as supplementary investigation in evaluating tumours around the knee joint. In the future, similar type of study with inclusion all doppler indices and large number of subjects is recommended.
*PLR-positive likelihood ratio*NLR-negative likelihood ratio