Classification of Root Canal Configurations: A Review and a New Proposal of Nomenclature System for Root Canal Configuration
Rashmi Bansal1, Sapna Hegde2, Madhu Sudan Astekar3
1 PhD Scholar, Department of Dentistry, Pacific Academy of Higher Education and Research University, Udaipur, Rajasthan, India.
2 Professor and Head, Department of Pedodontics and Preventive Dentistry, Pacific Dental College and Hospital, Udaipur, Rajasthan, India.
3 Professor and Head, Department of Oral Pathology and Microbiology, Institute of Dental Sciences, Bareilly, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rashmi Bansal, Flat No: A-4, Prof Qtrs, Rohilk Hand Medical College, Pilibhit Bypass Road, Bareilly, Uttar Pradesh, India.
E-mail: bansalrashmidr@rediffmail.com
Pulp space is complex, root canals may divide and rejoin. In the simplest form each root with one canal and single apical foramen is not observed always, other canal configurations are present which exit the root with two, three or more foramen. Several classifications have been proposed to describe root canal configurations for communication. With the advent of three dimensional imaging technique researchers are reporting newer configurations which cannot be classified using current system. Hence, newer classifications are proposed by each researcher. It is difficult to retain all classifications. Secondly, these newer classification are not the continuation of previous ones. Also, similar terminology has been used by different researchers for different configurations. Hence, in this paper instead of grouping root canal configurations into types, nomenclature system is proposed to identify each configuration individually.
Pulp space, Root canal morphology, Tooth anatomy, Vertucci classification, Weine classification
Introduction
Root canal morphology varies from tooth to tooth. The dental pulp is the soft tissue component of the root canal system. It occupies the internal cavities of the tooth [1]. The external boundary of pulp space resembles the shape of a root of the tooth [2].
Recent studies have demonstrated that root canal system is not a single canal running uniformly from orifice to apex infact it is very complex due to splitting and union of canals during its course to apex [3-6]. A root canal starts from orifice in the pulp chamber and opens apically into periodontium through apical foramen. During its course root canal presents a variety of configurations from teeth to teeth in different as well as in same individual [7].
As the configuration varies root canal classification is required to set terms for communication, diagnosis and treatment planning. Ideal requirement of a classification for root canal configuration is that it must define the tooth in terms of number of root, number of canal in each root and the course of canal from orifice to apex. At the same time it must be simple, accurate, reliable, easy to communicate and can be used in research, clinical practice and training. It can be applied in all types of root and root canal configuration in all groups of teeth.
Over the years, numerous root canal configurations have been identified resulting in the proposal of numerous classifications and their modifications. Clinical classification was given for the first time by studying root canal configuration in mesiobuccal root of maxillary first molar by Weine FS et al., [8]. It was further elaborated by Vertucci FJ in 1984 by including configurations for three canals also [9]. It is one of the most commonly used classifications in most of the studies [10]. Depending upon the configuration, root canal may exit apically through one or more than one apical foramen [8,9]. Advancement in non-destructive three dimensional imaging like cone beam computed tomography, micro-computed tomography as well as use of magnification have increased the number of reports on complex root canal anatomy [10,11]. Many root canal configurations reported now, using these techniques cannot be classified by Vertucci classification. Hence, various researchers also proposed newer classification [12-17]. Each classification is having its own advantages and limitations. In fact it is difficult to classify them into groups as number of groups represented by various types is increasing in each new study. Aim of this review was to overview various classification proposed till date according to the criteria, their applicability and limitations and to suggest a simple nomenclature system to identify each configuration individually.
Various morphological features on which root canal configurations are classified:
On the basis of number of canals from orifice to apex.
On the basis of number of roots and number of canals in each root.
On the basis of number of isthmus.
I. On the basis of number of canals from orifice to apex
Weine FS et al., was the first to categorize root canal configurations within a single root into four basic types [Table/Fig-1A] as [8]:
The root canal configurations from the pulp chamber to the root apex according to Weine FS et al., (A) and Vertucci FJ (B).

Type I (1-1): Single canal runs from orifice to apex.
Type II (2-1): Two canals arise from pulp chamber and during its course unite into one.
Type III (2-2): Two canals run separately from orifice to apex.
Type IV (1-2): One canal arises from floor of pulp chamber and during its course divides into two.
Vertucci FJ after studying the root canal morphology of maxillary first premolars by clearing technique [9], further elaborated Weine’s classification. He classified root canal systems into eight types [Table/Fig-1B] as:
Type I (1-1): Single canal runs from orifice to apex.
Type II (2-1): Two canals arises from pulp chamber which unite in its course into one.
Type III (1-2-1): One canal arises from pulp chamber and during its course splits into two. These two canals again unite into one before exiting from apex.
Type IV (2-2): Two canals run separately from orifice to apex.
Type V (1-2): One canal arises from floor of pulp chamber and during its course divides into two.
Type VI (2-1-2): Two canals start from pulp chamber, during its course; they unite into one and then again divide into two before exiting from root apex.
Type VII (1-2-1-2): One canal leave the pulp chamber which divide and again unite into in its course and finally divide into two before exiting from apex.
Type VIII (3-3): Three canals leave the pulp chamber and run independently towards the apex.
Kartal N et al., reported two new root canal configurations [Table/Fig-2A] in mandibular anterior teeth [10]:
The root canal configurations from the pulp chamber to the root apex according to Kartal N et al., (A) and Gulabivwala K et al., (B).
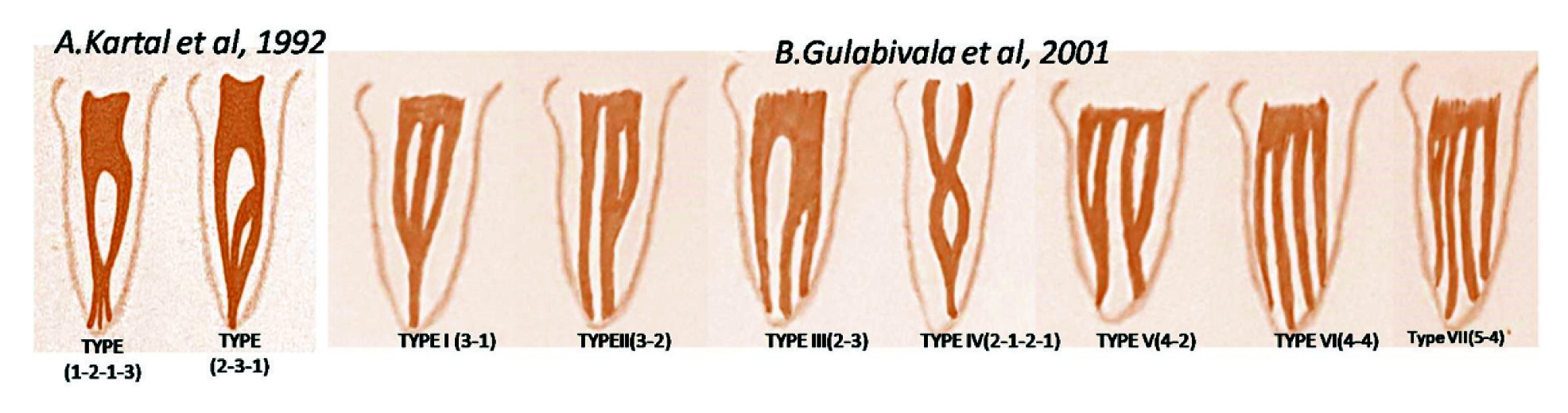
Root canal configuration (1-2-1-3): One canal starts from pulp chamber, divides into two in the middle third. These two canals join again into one canal and divides into three canals before exiting from root apex.
Root canal configuration (2-3-1): Two separate canals which extended from the pulp chamber to mid-root where the lingual canal divides into two; all three canals then joins in the apical third and exits as one canal.
Kartal N et al., divided Vertucci’s Type II into two subgroups [11]:
Type IIa: Two separate canals merge into one canal before reaching the apex.
Type IIb: Two separate canals joining within the apical foramen and then exited one apical foramen.
Gulabivala K et al., examined mandibular molars in a Burmese population and added seven additional configurations [Table/Fig-2B] to Vertucci’s classification as [12]: Type I to Type VII. These configurations classified 4 or 5 canals extending from the orifice also. These additional configurations were as follows:
Type I (3-1): The pulp space separates into three and joins in its course into one.
Type II (3-2): The pulp space separates into three and two of them join into one during its course to exit as two root canals.
Type III (2-3): The pulp space separates into two canals in the coronal portion and then one canal further divides into two and exit as three canals from the apex.
Type IV (2-1-2-1): The pulp space separates into two canals and joins into one during its course and then further divides into two canals and at the apex join into one and exit as one canal.
Type V (4-2): The pulp space in the coronal portion separates into four then during its course two canals joins together and exit as two canals at the apex.
Type VI (4-4): The pulp chamber near the coronal portion divides into four separate root canal extending till the apex of the root.
Type VII (5-4): The pulp chamber near the coronal portion divides into five separate canals and during its course one canal joins with other canal and exit as four canal.
Sert S and Bayirli GS evaluated root canal configurations in 2800 mandibular and maxillary permanent teeth in a Turkish population by clearing technique [13]. They also added fourteen new root canal configurations [Table/Fig-3] to Vertucci’s classification. They numbered them from Type IX to Type XXIII. These types were summarized as follows:
The root canal configurations from the pulp chamber to the root apex according to Sert S and Bayirli GS.

Type IX (1-3): The pulp space starts as a single canal and during its course divides into three canals.
Type X (1-2-3-2): The pulp space starts as a one canal divides into two out of which one canal further divides into two and later exit as two canals.
Type XI (1-2-3-4): The pulp space starts as a one canal divides into two out of which one canal further divides into two and run as three canals and later on other canals also divides and exit as four canals from the apex.
Type XII (2-3-1): Two canals leave the pulp chamber one canals gives off another branch, these three canals merge at the apex and exit as one canals.
Type XIII (1-2-1-3): One canal leaves the pulp chamber diverge into two canals then again merge into one canal and then divides into three canals to exit from the apex.
Type XIV (4-2): Four canals leaves the pulp chamber, two of each canal unites into one and exit as two canals from the apex.
Type XV (3-2): Three canals leave the pulp chamber and two canals unite into one and run as two canals and exit from the apex.
Type XVI (2-3): Two canals leave the pulp chamber, one canal gives off another branch and exit as three canals from the apex.
Type XVII (1-3-1): A wide canal leave the chamber and separates into three canals and then these three canals merge into one and exit as one canal from the apex.
Type XVIII (3-1): Three canals leave the pulp chamber and all of them join into one and exit from the pulp chamber.
Type XIX (2-1-2-1): Two canals leave the pulp chamber and then join into one then again divides into two and again unite into one.
Type XX (4): Four canals start from the pulp chamber and continue throughout the canal to exit as four canals.
Type XXI (4-1): Four canals leave the pulp chamber and later join into one.
Type XXII (5-4): Five canals leave the pulp chamber and one of them joins with other canals and exit as four canals from the apex.
Type XXIII (3-4): Three canals leave the pulp chamber one of them further divides into two and exit as four canal from the apex.
Peiris H et al., observed two additional root canal configurations (1-2-3) and (3-1-2) in their study [Table/Fig-4A] on permanent mandibular first molar of a Srilankan population [14].
The root canal configurations from the pulp chamber to the root apex according to Peiris H et al., (A) and Al-Qudah AA (B).
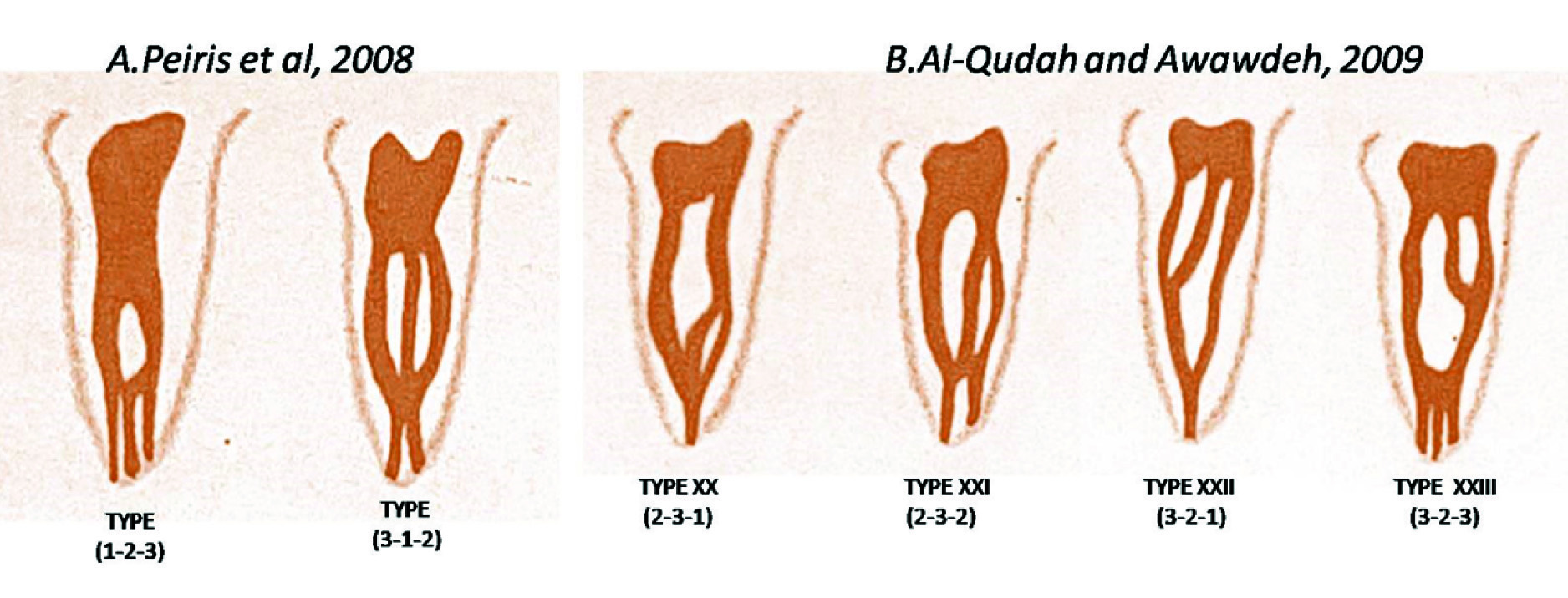
Al-Qudah AA observed four new types of configurations in their study [Table/Fig-4B] on root canal morphology of mandibular molars in a Jordanian population and assigned them as [15]:
Type XX (2-3-1): Two canal divides into three and then during its course unite into one,
Type XXI (2-3-2): Two canals divide into three and then during its course one canal unite into other resulting into two canal running towards the apex
Type XXII (3-2-1): Three canals originate from pulp chamber and unite first into two and then into one towards the apex
Type XXIII (3-2-3): Three canals divides into two running towards the apex and again divide into three.
II. On the Basis of Number of Roots and Number of Canals in Each Root:
Zhang R et al., gave classification for mandibular molars only according to the number of roots and the number of canals [Table/Fig-5A] in each root [16].
The root canal configurations from the pulp chamber to the root apex according to (A) Zhang R et al., (B) Silva EJNL et al.,.
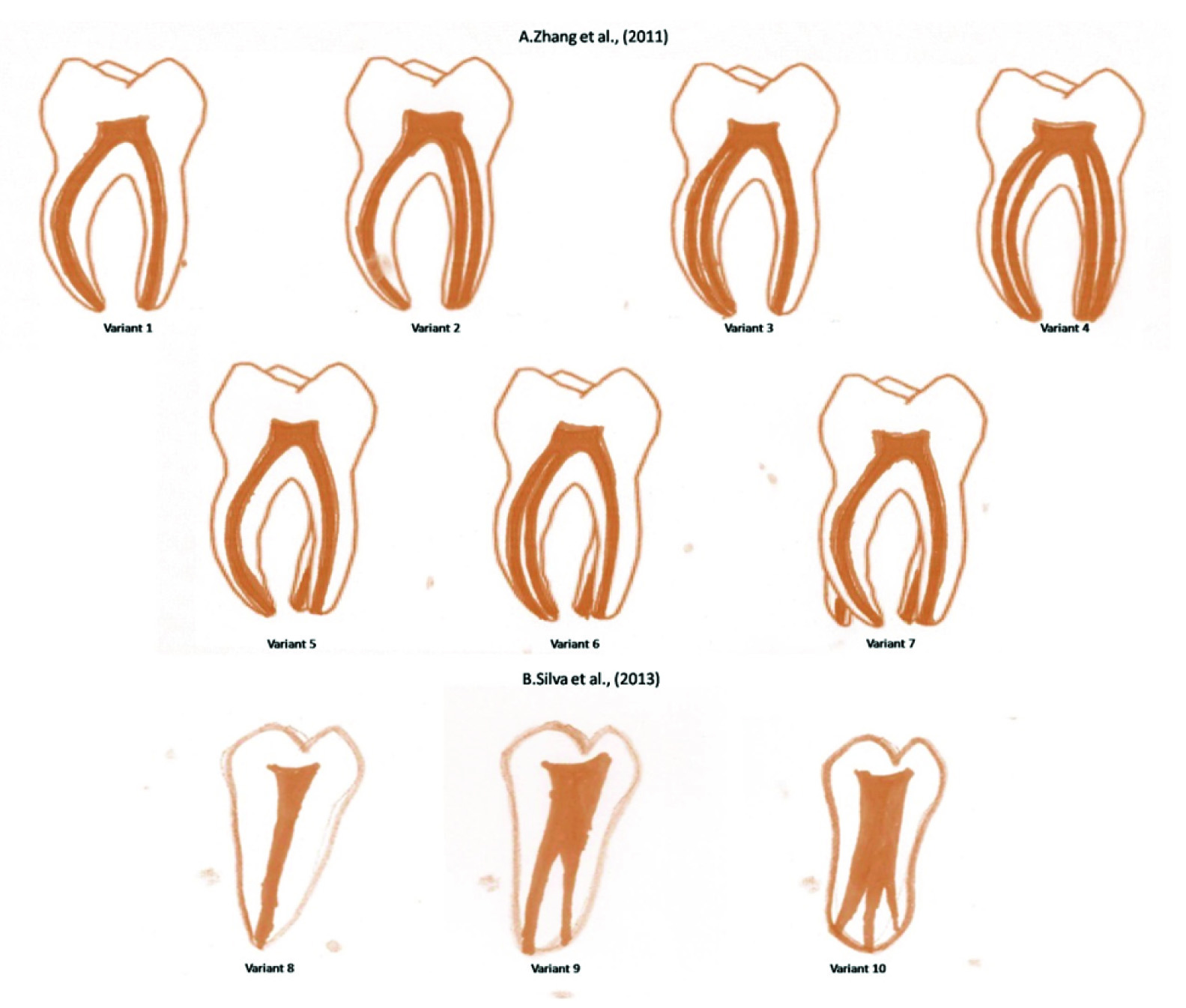
Variant 1: Two separate roots, a mesial and a distal root, with one canal in each root.
Variant 2: Two separate roots, a mesial and a distal root, with one canal in the mesial root and two canals in the distal root.
Variant 3: Two separate roots, a mesial and a distal root, with two canals in the mesial root and one canal in the distal root.
Variant 4: Two separate roots, a mesial and a distal root, with two canals in each root.
Variant 5: Three separate roots, mesial, distobuccal and distolingual, with one canal in each root.
Variant 6: Three separate roots, with two canals in the mesial root and one canal each in the distobuccal and distolingual roots.
Variant 7: Four separate roots, mesiobuccal, mesiolingual, distobuccal and distolingual, with one canal in each root.
Silva EJNL et al., added three more variants for mandibular molars [Table/Fig-5B] which were [17]:
Variant 8: One root with one canal,
Variant 9: One root with two canals
Variant 10: One root with three canals
III. On the Basis of Number of Isthmus: Kim SY Divided Apex Into Five Types [Table/Fig-6] [18]:
Classification according to isthmus by Kim SY
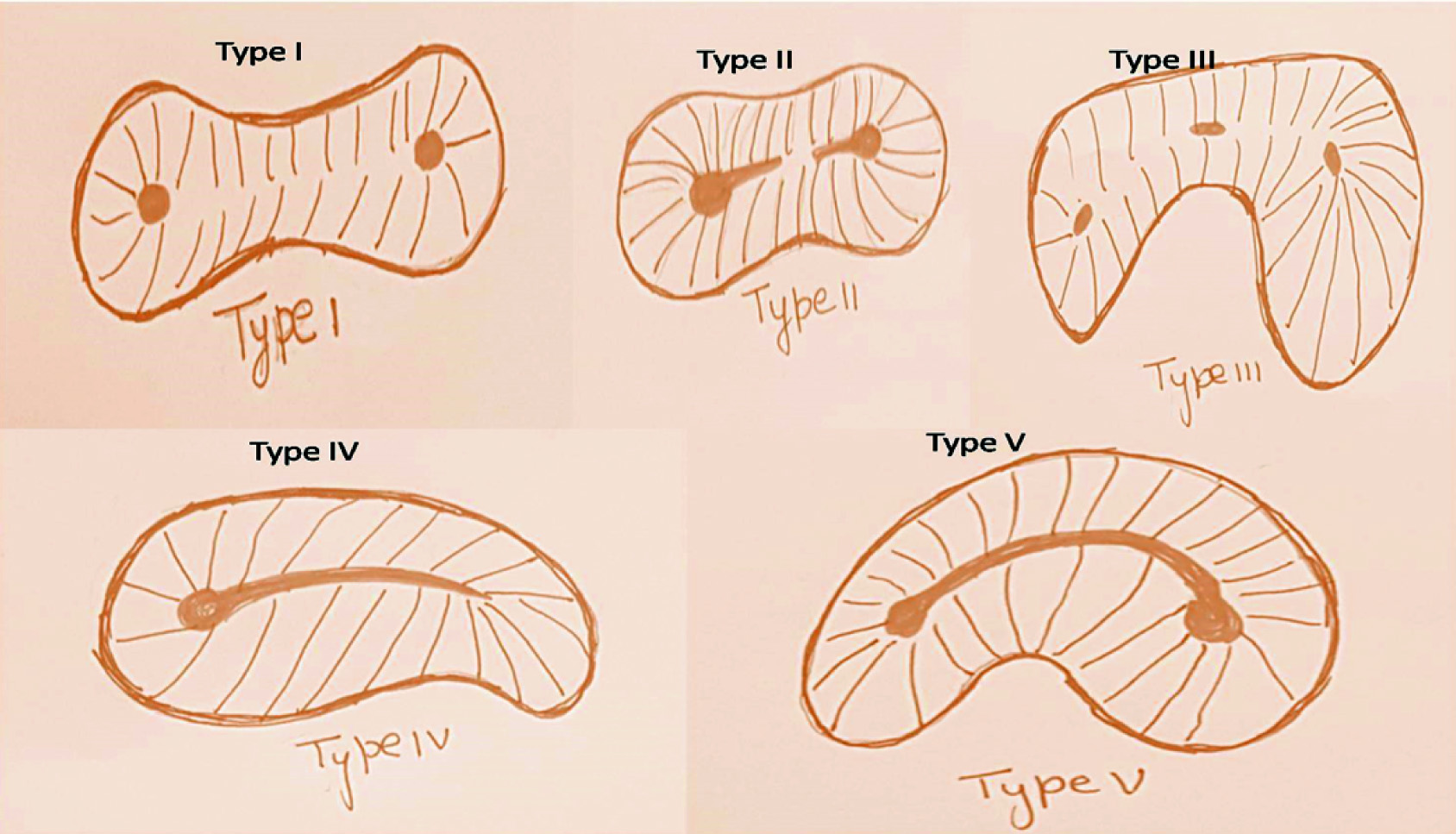
Type I: Two canals at root tip without any connection.
Type II: Two canals with incomplete connection between them.
Type III: Three canals at root tip without any connection.
Type IV: Extension of main canal resulting in a shape of tear.
Type V: Two canals with complete connection between them.
Limitation
Classification proposed by Weine FS et al., [8] Vertucci FJ et al., [9] were the most commonly used classification by various researchers in their studies [19], Apart from eight types of root canal configurations suggested by Vertucci FJ et al., additional types were reported in various studies [12-15,19,20].
Advanced 3D imaging technology has revealed that the morphological characteristics of root canal system are highly complex and many canal configuration cannot be described even by Gulabivala K classification [21-24].
Another limitation of these classifications is that it did not explain in which root of multi-rooted teeth canals are encased [25].
Division or union of canals is taking place in which part of rootcanal. Division of canal in the coronal, middle or apical third will be coded same e.g., 1-2-1 can be coded for all canals in which bifurcation is taking place at coronal third, middle third or apical third. In Weine FS [8] Type II/Vertucci FJ [9] Type II (2-1), Vertucci FJ [9] Type III (1-2-1), AlQudah AA [15] Type XXII (3-2-1) two canals are uniting into one, but in which part of root canal space two canals are uniting is not clear [26].
These classifications do not consider the position of apical foramen through which root canal exit [27].
The assessment of apical canal configurations may vary e.g., some apical bifurcations could either be classified as an apical delta/ramification or a division from the main canal (Type 1-2) [28].
It is difficult to memorize all classifications and hence Vertucci FJ [9] classification and additional configuration given by Gulabivala K [12] are the main classification used for communication purposes [29,30].
Further there was difference in nomenclature in other classification also for e.g., Al–Qudah AA [15] classified Type XX, Type XXI, Type XXII as (2-3-1),(2-3-2), (3-2-1) respectively; while Sert S [13] coined Type XX, Type XXI, Type XXII as (4-4), (4-1), (5-4) respectively [Table/Fig-7]
Different configuration assigned for same category
| Type | Sert S | Al–Qudah AA |
|---|
| Type XX | (4-4) | (2-3-1) |
| Type XXI | (4-1) | (2-3-2) |
| Type XXII | (5-4) | (3-2-1) |
Different types were assigned by different classification system to a same configuration e.g., 3-1 configuration was assigned Type I by Gulabivala K [12] and Type XVIII by Sert S [13] classification system [Table/Fig-8].
Different category assigned to same configuration
| Configuration | Gulabivala K et al | Sert S |
|---|
| 3-1 | Type I | Type XVIII |
| 3-2 | Type II | Type XV |
| 2-3 | Type III | Type XVI |
| 2-1-2-1 | Type IV | Type XIX |
| 4-2 | Type V | Type XIV |
| 4-4 | Type VI | Type XX |
| 5-4 | Type VII | Type XXII |
IV. Four digit formula according to course of canal in coronal, middle and apical third:
Briseno-Marroquin B et al., divided root canal into thirds and gave a digit to each third [31]. Fourth digit was given to number of foramina. But this classification was not clinically applicable, as it is not possible to divide root canal clinically into thirds on intraoral radiographs. Secondly number of foramen cannot be evaluated accurately by intraoral periapical radiographs.
As newer and newer configurations are reported in studies, it is difficult to classify them into groups by classifying them; instead they should be named individually by a simple nomenclature system which can define a particular configuration.
V. Morphological Features to be Considered while Giving a Nomenclature System:
Tooth type
Root in which configuration is encased
Root canal configuration from orifice to apex
Location at which root canal exit from root apex.
Anatomic variations like radix molar, C shaped canal etc
VI. New Proposal: [Table/Fig-9]
The proposed root canal configurations from the pulp chamber to the root apex.

Tooth number: The tooth number can be written using FDI system of nomenclature.
Nomenclature of root written on the right side of the tooth number.
The course of the canal in each root mentioned in round brackets written on right side of the nomenclature of each root.
Number of foramen through which canal is exiting at the apex is mentioned after putting slash to course of canal.
Proposal for anatomic variations:
C- Shape canal can be mentioned by letter “C” added to the left of the tooth number. The fusion between canals can be depicted (-) between canals
Taurodontism can be mentioned by adding letter “T” added to the left of the tooth number.
Single root can be mentioned by adding letter “R” added to the right of the tooth number.
Individual names like Radix paramolaris, Radixentomolaris, middle mesial canal etc., are not required. Additional root of Radix paramolaris can be written Mesiobuccal (MB) or Distobuccal (DB) and similarly additional root of Radix entomolaris as Mesiolingual (ML) or Distolingual (DL) depending on its anatomical position. Similarly middle mesial canal i.e., canal in between MB and ML canal can be written as 3-3, 3-2 or 3-1 depending on the course of middle canal from orifice to apex.
For example: 47M(1-2-1-2/2)D(1-1-1/1) can be represented as Right mandibular second molar with mesial root having configuration –one canal arise from pulp chamber, during its course divides into two and then again unite into one and then divide into two which exits through two foramen. In the distal root one canal continues from orifice to apex and exit by one foramen.
Conclusion
All classification reported till date has their advantages and limitations. The proposed nomenclature system takes into account the tooth type, number of roots and course of canal in each root. This classification is a simple, reliable, accurate and easy for communication as it is guided by course of canal. Further the proposed system can define any new configuration. Hence it can be used both for clinical and research work.
[1]. Toure B, Faye B, Kane AW, Lo CM, Niang B, Boucher Y, Analysis of reasons for extraction of endodontically treated teeth:a prospective studyJ Endod 2011 37:1512-15.10.1016/j.joen.2011.07.00222000453 [Google Scholar] [CrossRef] [PubMed]
[2]. Shetty A, A three dimensional study of variations in root canal morphology using cone-beam computed tomography of mandibular premolars in a south indian populationJ Clin Dent Res 2014 8:22-24.10.7860/JCDR/2014/8674.470725302261 [Google Scholar] [CrossRef] [PubMed]
[3]. Hess W, Formation of Root-Canals in Human Teeth “Zur Anatomie der Wurzelkanale des menschliches Gebisses,” Schweizerische Vierteljahrsschrift fur Zahnheilkunde, 1917. Translated by Newton G. Thomas, AB, MA, DDS, and Herman Redlich, Chicago, IllinoisThe Journal of the National Dental Association 1921 8:704-34.10.14219/jada.archive.1921.0179 [Google Scholar] [CrossRef]
[4]. Gu Y, Lu Q, Wang H, Ding Y, Wang P, Ni L, Root canal morphology of permanent three rooted mandibular first molars-part I:pulp floor and root canal systemJ Endod 2010 36:1341-46.10.1016/j.joen.2010.04.02520647093 [Google Scholar] [CrossRef] [PubMed]
[5]. Filpo–Perez C, Bramante CM, Villas-Boas MH, Duarte MAH, Versiani MA, Ordinola-Zapata R, Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molarsJ Endod 2015 41:231-36.10.1016/j.joen.2014.09.02425447505 [Google Scholar] [CrossRef] [PubMed]
[6]. Tahmasbi M, Jalali P, Nair K, Madhu KN, Sevin B, Nair UP, Prevalence of middle mesial canals and isthmi in the mesial root of mandibular molars:an in vivo cone-beam computed tomographic studyJ Endod 2017 43:1080-83.10.1016/j.joen.2017.02.00828527840 [Google Scholar] [CrossRef] [PubMed]
[7]. Ballullaya SV, Vemuri S, Kumar PR, Variable permanent mandibular first molar: review of literatureJ Conserv Dent 2013 16:99-110.10.4103/0972-0707.10817623716959 [Google Scholar] [CrossRef] [PubMed]
[8]. Weine FS, Pasiewicz RA, Rice RT, Canal configuration of the mandibular second molar using a clinically oriented in vitro methodJ Endod 1969 14:207-13.10.1016/S0099-2399(88)80171-7 [Google Scholar] [CrossRef]
[9]. Vertucci FJ, Root canal anatomy of the human permanent teethOral Surg, Oral Med, Oral Pathol 1984 58:589-99.10.1016/0030-4220(84)90085-9 [Google Scholar] [CrossRef]
[10]. Kartal N, Yanıkoğlu FÇ, Root canal morphology of mandibular incisorsJ Endod 1992 S18:562-64.10.1016/S0099-2399(06)81215-X [Google Scholar] [CrossRef]
[11]. Kartal N, Cimilli HK, The degrees and configurations of mesial canal curvatures of mandibular first molarsJ Endod 1997 23:358-62.10.1016/S0099-2399(97)80182-3 [Google Scholar] [CrossRef]
[12]. Gulabivala K, Aung T, Alavi A, Ng YL, Root and canal morphology of Burmese mandibular molarsInt Endod J 2001 34:359-70.10.1046/j.1365-2591.2001.00399.x11482719 [Google Scholar] [CrossRef] [PubMed]
[13]. Sert S, Bayirli GS, Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish populationJ Endod 2004 30:391-98.10.1097/00004770-200406000-0000415167464 [Google Scholar] [CrossRef] [PubMed]
[14]. Peiris H, Pitakotuwage T, Takahashi M, Sasaki K, Kanazawa E, Root canal morphology of mandibular permanent molars at different agesInt Endod J 2008 41:828-35.10.1111/j.1365-2591.2008.01428.x18822010 [Google Scholar] [CrossRef] [PubMed]
[15]. Al-Qudah AA, Awawdeh LA, Root and canal morphology of mandibular first and second molar teeth in a Jordanian populationInt Endod J 2009 42:775-84.10.1111/j.1365-2591.2009.01578.x19549153 [Google Scholar] [CrossRef] [PubMed]
[16]. Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PM, Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individualsInt Endod J 2011 44:990-99.10.1111/j.1365-2591.2011.01904.x21658074 [Google Scholar] [CrossRef] [PubMed]
[17]. Silva EJNL, Nejaim Y, Silva AV, Haiter-Neto F, Cohenca N, Evaluation of root canal configuration of mandibular molars in a Brazilian population by using cone-beam computed tomography: an in vivo studyJ Endod 2013 39:849-52.10.1016/j.joen.2013.04.03023791250 [Google Scholar] [CrossRef] [PubMed]
[18]. Kim SY, Kim BS, Woo J, Kim Y, Morphology of mandibular first molars analyzed by cone-beam computed tomography in a Korean population: variations in the number of roots and canalsJ Endod 2013 39:1516-21.10.1016/j.joen.2013.08.01524238439 [Google Scholar] [CrossRef] [PubMed]
[19]. Jung IY, Seo MA, Fouad AF, Spangberg LSW, Apical anatomy in mesial and mesiobuccal roots of permanent first molarsJ Endod 2005 31:364-68.10.1097/01.don.0000145425.73364.9115851930 [Google Scholar] [CrossRef] [PubMed]
[20]. Ratanajirasut R, Panichuttra A, Panmekiate S, A cone beam computed tomographic study of root and canal morphology of maxillary first and second permanent molars in a Thai populationJ Endod 2018 44:56-61.10.1016/j.joen.2017.08.02029061352 [Google Scholar] [CrossRef] [PubMed]
[21]. Wang Y, Zheng QH, Zhou XD, Tang L, Wang Q, Zheng GN, Evaluation of the root and canal morphology of mandibular first permanent molars in a western chinese population by cone beam computed tomographyJ Endod 2010 36:1786-89.10.1016/j.joen.2010.08.01620951288 [Google Scholar] [CrossRef] [PubMed]
[22]. Villas-Boas MH, Bernardineli N, Cavenago BC, Marciano M, Carpio-Perochena AD, de Moraes IG, Micro computed tomography study of the internal anatomy of mesial root canals of mandibular molarsJ Endod 2011 37:1682-86.10.1016/j.joen.2011.08.00122099905 [Google Scholar] [CrossRef] [PubMed]
[23]. Martins JN, Anderson C, Endodontic treatment of the mandibular first molar with six roots canals - two case reports and literature reviewJ Clin Dent Res 2015 9:ZD06-8.10.7860/JCDR/2015/11866.577926023651 [Google Scholar] [CrossRef] [PubMed]
[24]. Perez-Heredia M, Ferrer-Luque CM, Bravo M, Castelo-Baz P, Ruiz-Pinon M, Baca P, Cone beam computed tomographic study of root anatomy and canal configuration of molars in a Spanish populationJ Endod 2017 43:1511-16.10.1016/j.joen.2017.03.02628735786 [Google Scholar] [CrossRef] [PubMed]
[25]. Lee KW, Kim Y, Perinpanayagam H, Lee JK, Yoo YJ, Lim SM, Comparison of alternative image reformatting techniques in micro computed tomography and tooth clearing for detailed canal morphologyJ Endod 2014 40:417-22.10.1016/j.joen.2013.09.01424565663 [Google Scholar] [CrossRef] [PubMed]
[26]. Wolf TG, Paque F, Zeller M, Willershausen B, Briseno-Marroquin B, Root canal morphology and configuration of 118 mandibular first molars by means of micro-computed tomography:an ex-vivo studyJ Endod 2016 402:610-14.10.1016/j.joen.2016.01.00426906239 [Google Scholar] [CrossRef] [PubMed]
[27]. Somasundaram P, Rawtiya M, Wadhwani S, Uthappa R, Shivagange V, Khan S, Retrospective study of root canal configurations of mandibular third molars using CBCT-Part-IIJ Clin Dent Res 2017 11:ZC5510.7860/JCDR/2017/20153.1007228764294 [Google Scholar] [CrossRef] [PubMed]
[28]. Ghobashy AM, Nagy MM, Bayoumi AA, Evaluation of root and canal morphology of maxillary permanent molars in Egyptian population by cone beam computed tomographyJ Endod 2017 43:1089-92.10.1016/j.joen.2017.02.01428476465 [Google Scholar] [CrossRef] [PubMed]
[29]. Albuquerque DV, Kottor J, Dham S, Velmurugan N, Abarajithan M, Sudha R, Endodontic management of maxillary permanent first molar with 6 root canals: 3 case reportsOral Surg, Oral Med, Oral Pathol, Oral Radiol and Endod 2010 110:e79-83.10.1016/j.tripleo.2010.04.01720656533 [Google Scholar] [CrossRef] [PubMed]
[30]. Miloglu O, Arslan H, Barutcigil C, Cantekin K, Evaluating root and canal configuration of mandibular first molars with cone beam computed tomography in a Turkish populationJournal of Dental Sciences 2013 8:80-86.10.1016/j.jds.2012.09.002 [Google Scholar] [CrossRef]
[31]. Briseño-Marroquín B, Paqué F, Maier K, Willershausen B, Wolf TG, Root canal morphology and configuration of 179 maxillary first molars by means of micro-computed tomography: an ex vivo studyJ Endod 2015 41:2008-13.10.1016/j.joen.2015.09.00726518215 [Google Scholar] [CrossRef] [PubMed]