Synchronous Odontogenic Cysts in Mandible
Neha Agrawal1, Sunitha Carnelio2, Raghu Radhakrishnan3, Adarsh Kudva4, Gabriel Rodrigues5
1 Postgraduate, Department of Oral and Maxillofacial Pathology, Manipal College of Dental Sciences, MAHE, Manipal, Karnataka, India.
2 Professor, Department of Oral and Maxillofacial Pathology, Manipal College of Dental Sciences, MAHE, Manipal, Karnataka, India.
3 Professor, Department of Oral and Maxillofacial Pathology, Manipal College of Dental Sciences, MAHE, Manipal, Karnataka, India.
4 Associate Professor, Department of Oral and Maxillofacial Surgery, Manipal College of Dental Sciences, MAHE, Manipal, Karnataka, India.
5 Professor, Department of General Surgery, Kasturba Medical College, MAHE, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sunitha Carnelio, Professor, Department of Oral and Maxillofacial Pathology, Manipal College of Dental Sciences, MAHE, Manipal-576104, Karnataka, India.
E-mail: sunithacarnelio@yahoo.co.uk
Odontogenic cysts are derived from odontogenic apparatus which may develop before or after the formation of tooth. Most of these are developmental in origin. However, non-odontogenic cysts also exist in the jaw. Among the odontogenic cysts the most prevalent are periapical cyst followed by dentigerous and Odontogenic Keratocyst (OKC). OKC was also termed as Keratocystic Odontogenic Tumour (KCOT), well-known for its aggressive behaviour, varied origin, debated development and tendency to recur has been the focus of much research and discussion since four decades. It arises either from epithelial rests of the dental lamina or the tooth primordium and is generally aggressive and invasive, while dentigerous cysts are common odontogenic cysts that are related to the crown of the impacted tooth and known to arise from reduced enamel epithelium. It is rare to find both these entities occurring simultaneously in the same patient. Multiple OKC are generally associated with nevoid basal cell carcinoma syndrome, and accounts to the mutation in the PTCH, a tumour suppressor gene. However, this case reports a non-syndromic variant. A 13-year-old female patient with multiple cysts in the jaw that were evaluated, diagnosed and treated adequately based on clinical, radiographic and histopathological examination has been discussed.
Dentigerous cyst, Enucleation, Odontogenic keratocyst
Case Report
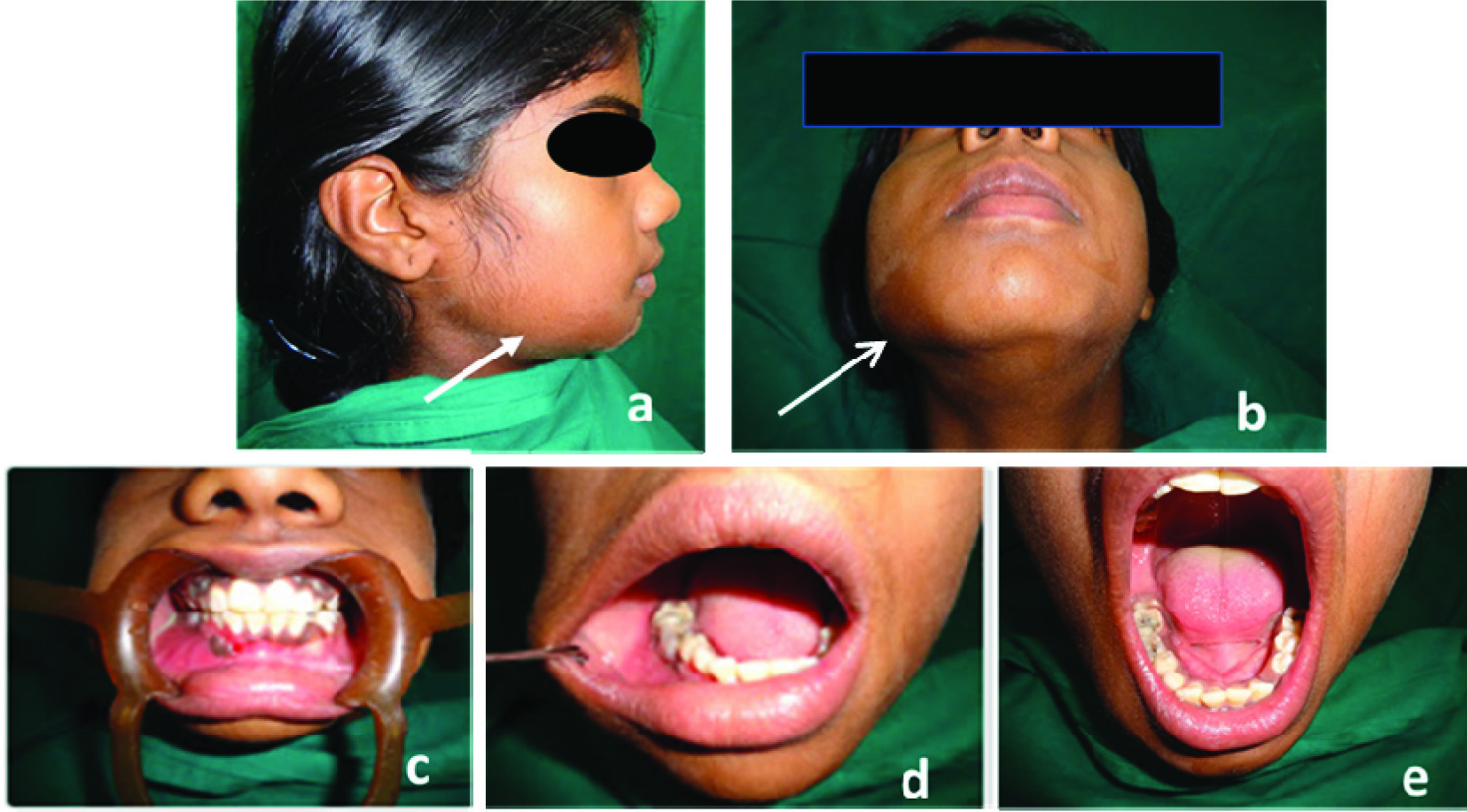
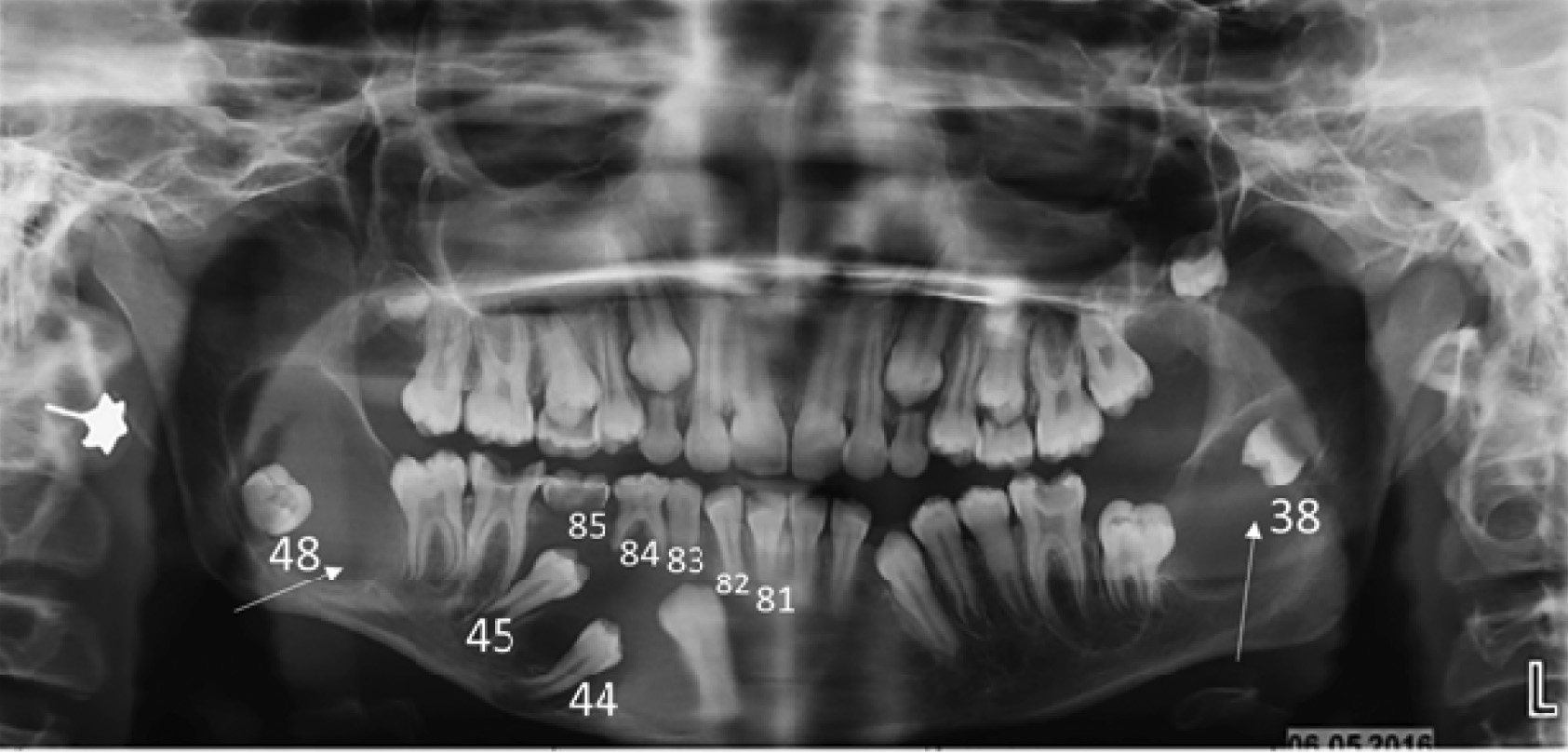
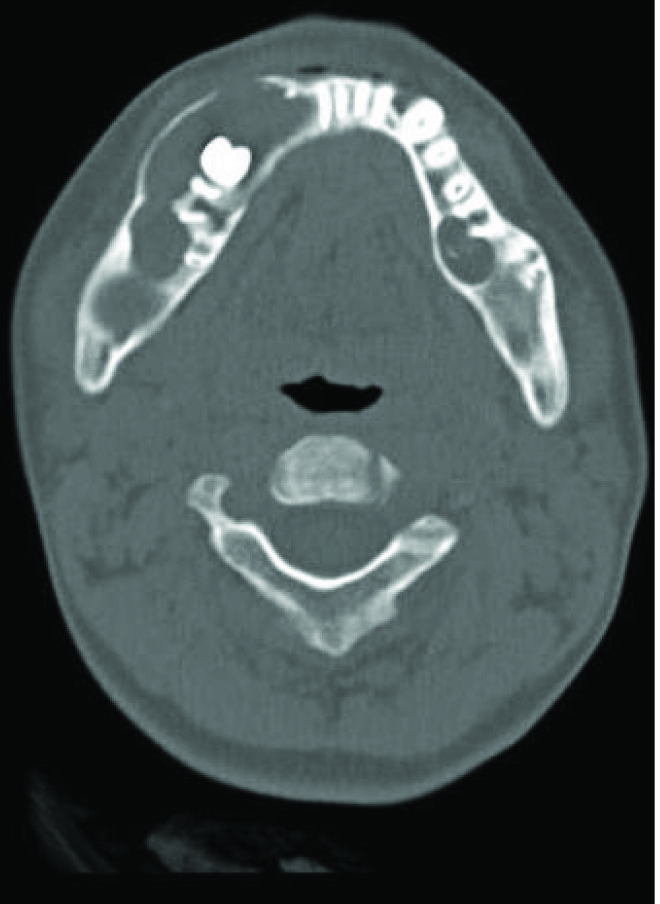
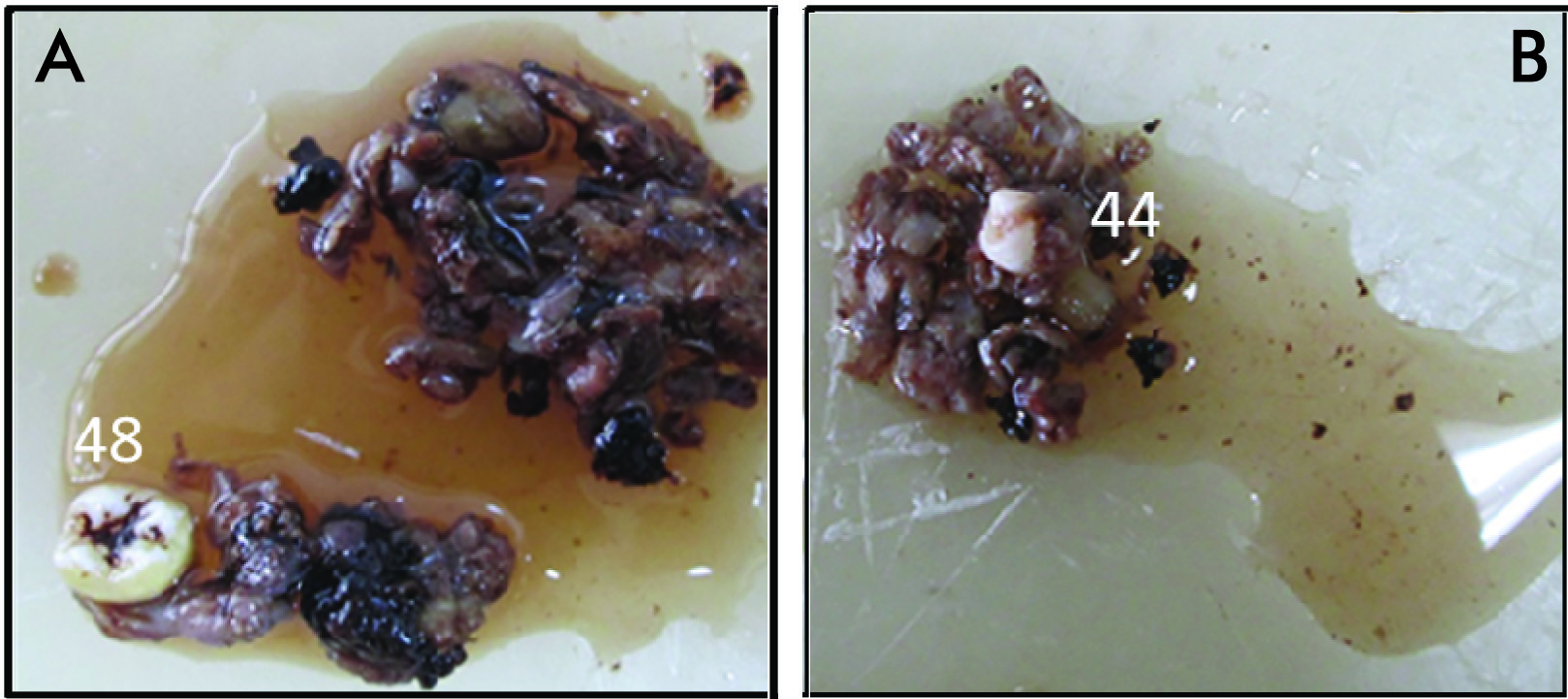
A 13-year-old female patient visited the Department of Oral and Maxillofacial Surgery with a complaint of pain and swelling in her lower jaw since one month. The pain was dull aching in nature and the swelling gradually increased in size, with pus discharge from lower anterior alveolus region. There was no history of trauma, tooth extraction, trismus and fever. Extraoral examination revealed a soft to firm swelling in relation to right lower border of mandible with mild tenderness and increase in temperature. Intraoral examination revealed a soft to firm swelling, mild tenderness and buccal cortical plate expansion in relation to right lower vestibule region with sulcus obliteration [Table/Fig-1]. Routine laboratory investigations (haematological and serological) were normal. Orthopantomogram (OPG) revealed a diffuse radiolucency seen in the periapical region of 83 to 85 with impacted 44,45. A well-defined unilocular radiolucency with corticated borders were seen at the peri coronal region of 38 and 48, extending from the anterior border of ramus till the mesial root of 36 with superior displacement of 38 and distal aspect of 47 with apical displacement of 48. There was complete effacement of inferior alveolar canal bilaterally [Table/Fig-2]. Chest and skull X-rays were unremarkable with no relevant dermatological findings. A plain CT (Computed Tomography) was performed which revealed multiple cysts of the jaw [Table/Fig-3]. A differential diagnosis of OKC, dentigerous cyst and a unicystic ameloblastoma were suggested. An informed consent form duly signed by the patient and her parents was obtained prior to surgery. The lesion was surgically enucleated [Table/Fig-4] followed by chemical treatment with Carnoy’s solution along with the extraction of impacted 38, 44, 84, 85 and 48. However, during enucleation of 38, involvement of 37 and its associated region was observed. Hence 37 was difficult to be salvaged and had to be extracted. The Haematoxylin and Eosin (H&E) stained section of the tissue attached to unerupted mandibular premolar 44 revealed a cystic lumen lined by parakeratinised stratified squamous epithelium of 4-6 cell layer thickness. The basal layer showed columnar cells with hyperchromatic palisading nuclei. However, in areas where it was near the neck of the teeth, it showed a layer of reduced enamel epithelium. The capsular tissue appeared to be delicate dense infiltrate of chronic inflammatory cells, i.e., lymphocytes and plasma cells. These features were suggestive of an OKC [Table/Fig-5]. In the enucleated cystic lining from the right ramus region, there was presence of multiple odontogenic rests resembling off shoots [Table/Fig-6]. Thus, a diagnosis of an OKC with secondary infection was made with respect to (w.r.t) 48 [Table/Fig-7].
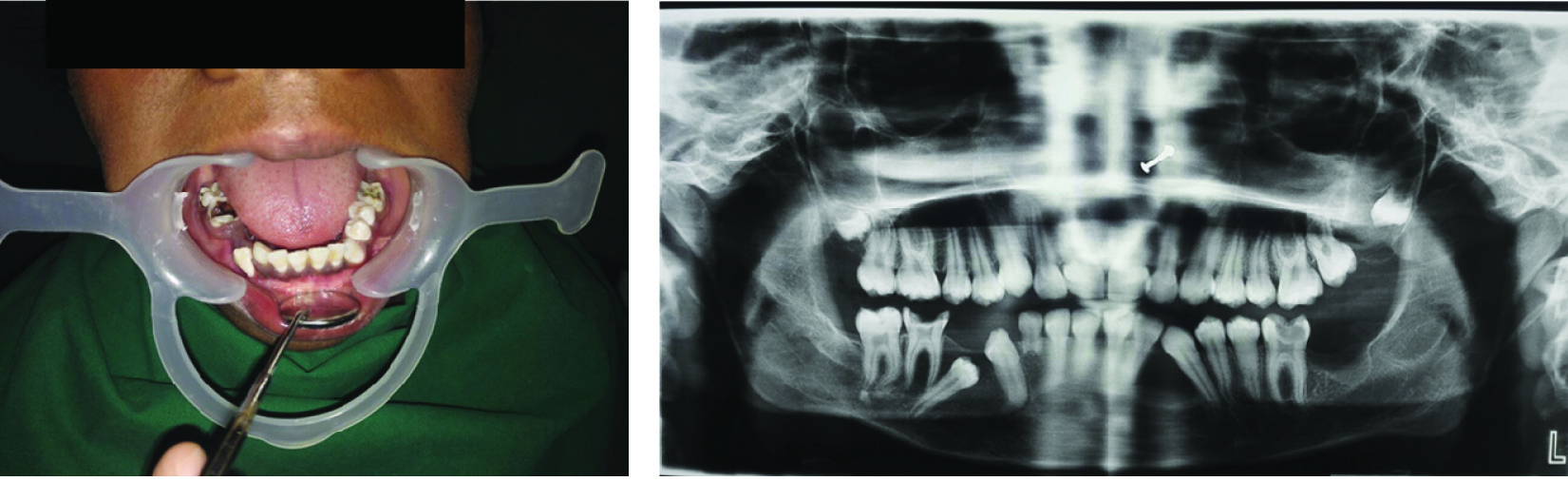
a,b) Extraorally, a diffuse swelling in relation to lower jaw in the region of premolar molar area. c-e) Intraorally, sulcus obliteration is evident in the same region.
Orthopantomogram showing radiolucencies in association with impacted 44, 45,38, 48.
CT skull showing multiple cysts of the jaw.
Excised lesional multiple soft tissue bits in relation to different teeth. (A) 48 and (B) 44.
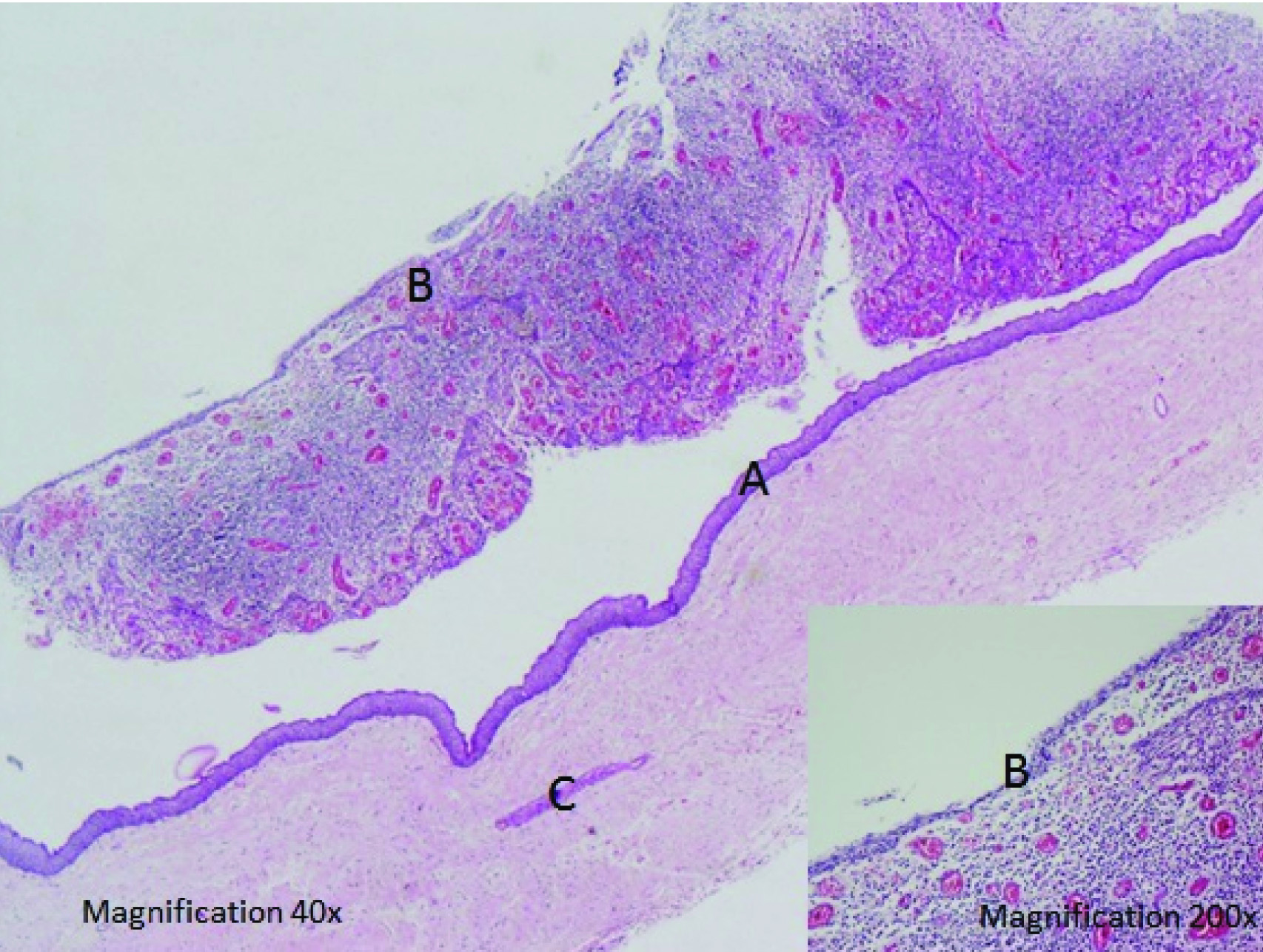
KCOT. Lining epithelium (A); reduced enamel epithelium (B); capsular tissue (C), insite shows the reduced enamel epithelium, w.r.t 44.
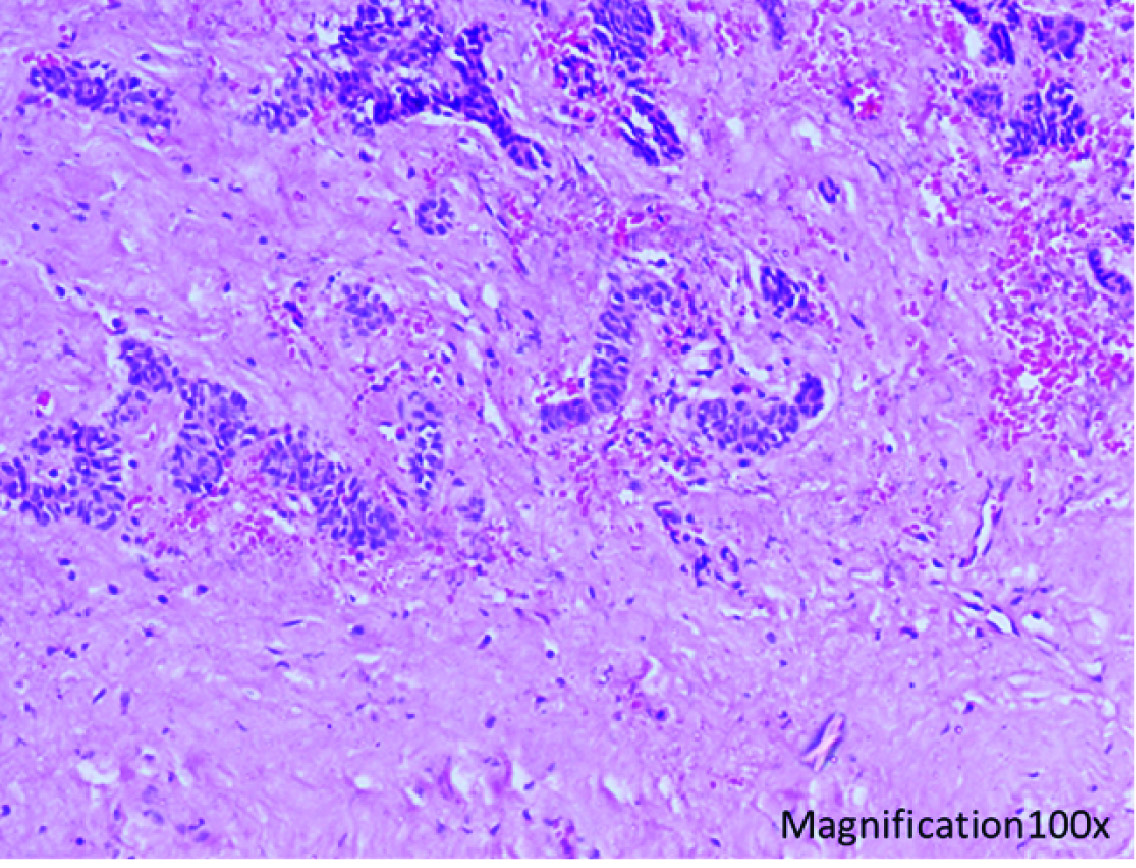
Photomicrograph (100X) showing numerous odontogenic rests in the right ramus region.
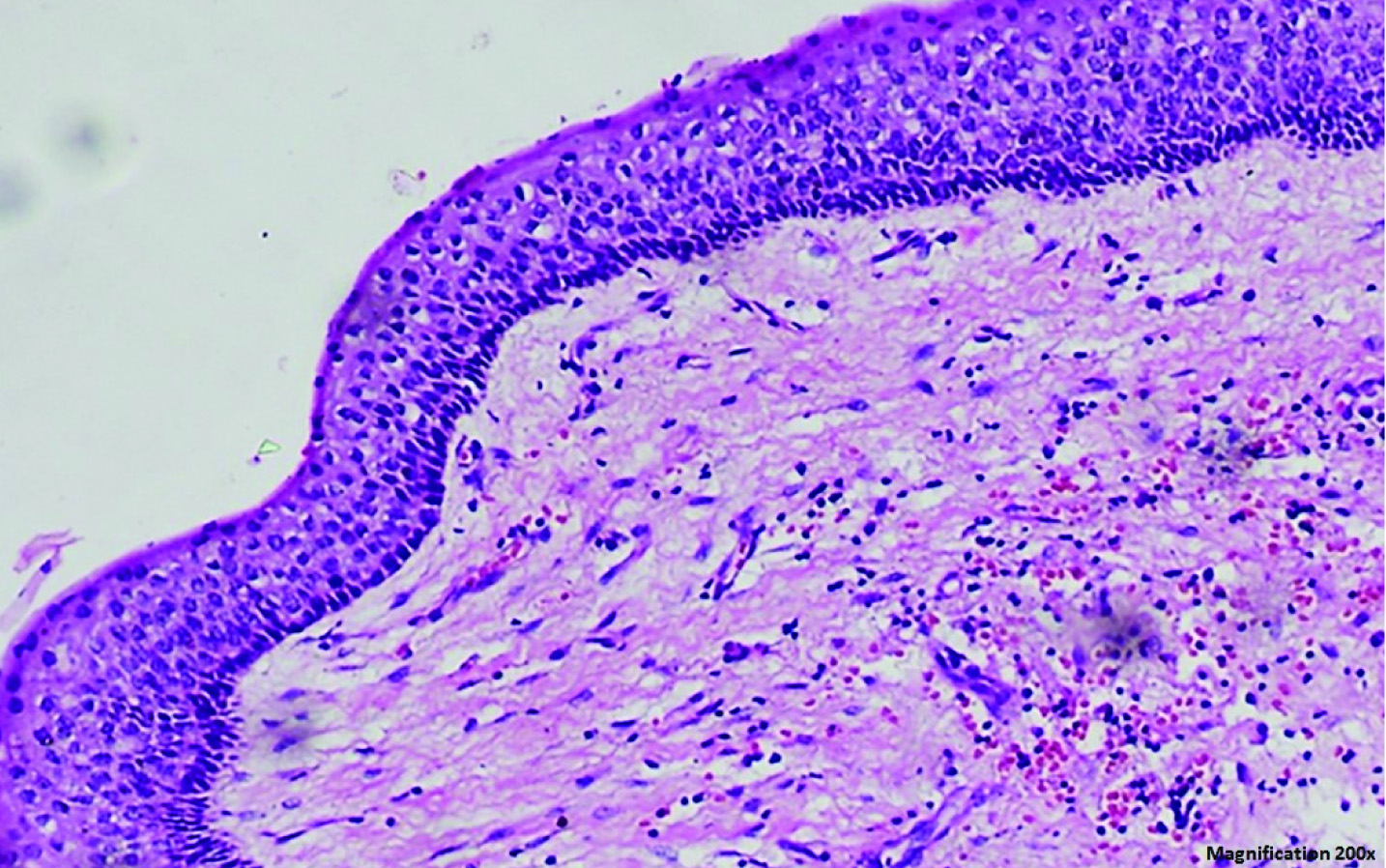
Photomicrograph (200X) showing parakeratinised stratified squamous epithelium with 4-6 layers of epithelium, w.r.t 48.
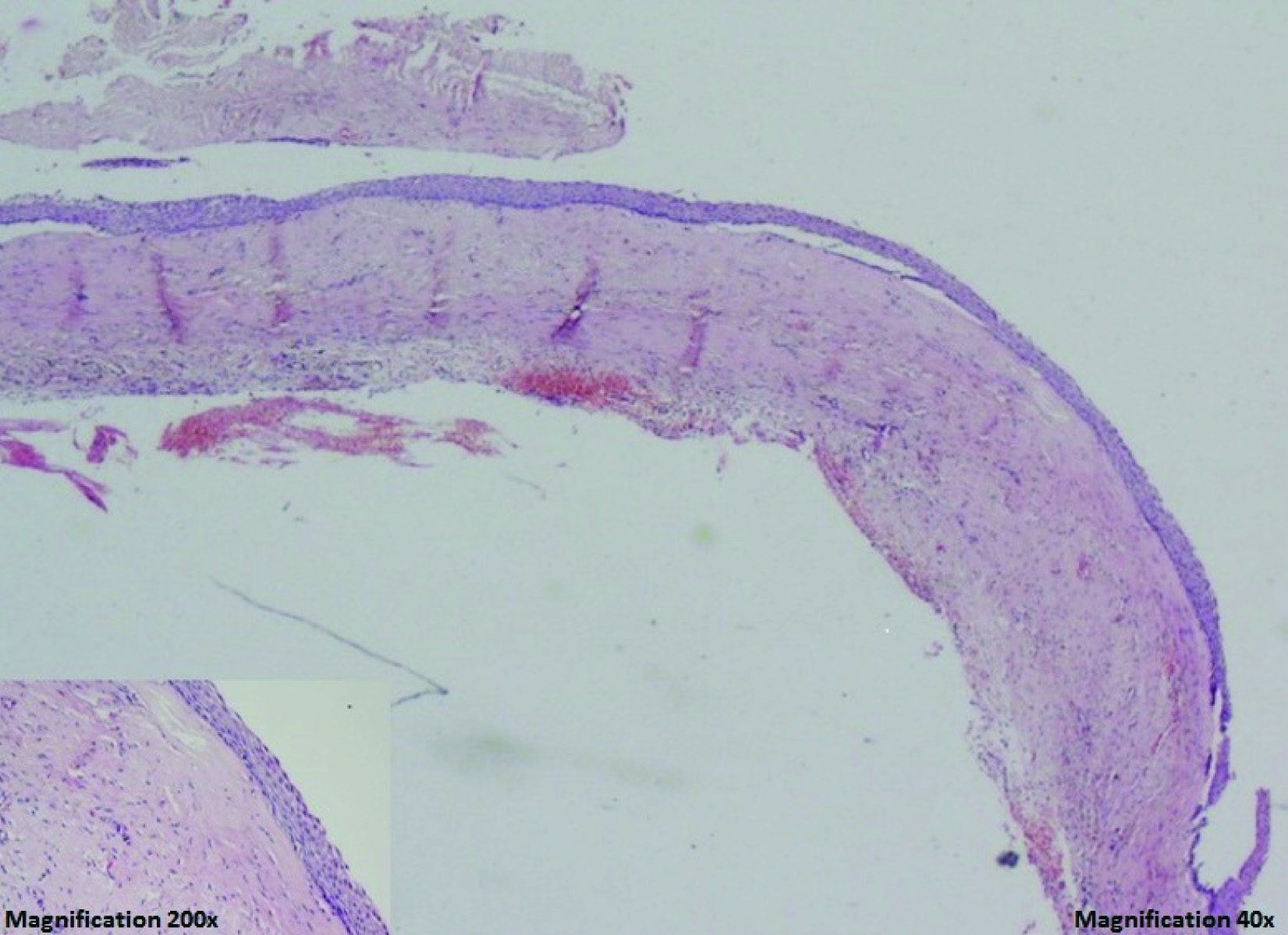
The H&E stained section of tissue attached to unerupted 38 at the Cemento-Enamel Junction (CEJ) revealed a cystic lumen lined by 2-3 layers of non-keratinised stratified squamous epithelium that at places was hyperplastic. Below the epithelium, the capsular tissue was edematous, delicate to dense with plump fibroblasts, blood vessels and focal aggregates of chronic inflammatory cells suggestive of a dentigerous cyst w.r.t to 38 [Table/Fig-8].
Photomicrograph (40X) showing lining epithelium of dentigerous cyst, w.r.t 38.
The dilemma of terming the OKC in relation to 44 as a follicular variant of OKC was ruled out after discussion, consensus, correlating the clinical, radiographic and histopathological findings and a final diagnosis of OKC in relation to 44, infected OKC in relation to 48 and a central variant of dentigerous cyst in relation to 38 were made. Patient was kept under close observation and at the end of two years of follow-up, there has been no recurrence [Table/Fig-9].
Postoperative X-ray and clinical photograph at the end of one year.
Discussion
WHO in its latest classification of odontogenic cysts, odontogenic and maxillofacial bone tumours published in 2017 has reinstalled the term ‘odontogenic cyst’. This classification has reconsidered KCOT as a cyst and renamed it as OKC. The authors justify the fact that OKC completely regress following decompression, and they also observed the lining epithelium of OKC to resemble to that of oral mucosa. The loss of heterozygosity observed in OKC was also observed in other cysts. The panel of scientists do not completely disagree OKC to be neoplastic, since evidences prove their aggressive behaviour [1].
Among the various odontogenic cysts of the jaw, OKC accounts for 3-11% [2]. Dentigerous cysts being developmental in origin is the second most common odontogenic cysts of the jaw and are most frequently associated with impacted mandibular third molar teeth at the cemento-enamel junction [3]. The present case was a unique case of synchronous multiple cysts occurring in the jaw of an individual with different histopathological presentations. Though occlusal radiographs are preferred to assess the buccal cortical expansion, in this case CT was the choice since patient had multiple cysts and the radiolucencies were extending beyond the body of the mandible. CT is also beneficial in determining cortical perforation and soft tissue involvement with its anteroposterior extent along the marrow in axial sections. A thorough literature search has been made and to the best of our knowledge we haven’t come across reports on two types of developmental cysts occurring in a single jaw. We have come across multiple lesions which could be syndromic or non-syndromic associated OKC or multiple dentigerous cysts in the jaws or siblings.
KCOT are developmental in origin but are considered aggressive because of their invasion into surrounding tissues and a high recurrence rate (3-60%), even after total surgical excision [3-5]. Dentigerous cysts are also developmental in origin arising from fluid accumulation between the reduced enamel epithelium and erupting tooth resulting from the obstruction of veins during eruption and are radiographically seen to be attached to the neck of the teeth. However, on histopathological examination the cyst is lined by 2 to 3 layers of reduced enamel epithelium as was seen in our patient in relation to 38. Studies have shown immunoreactivity to PCNA, Ki67, p53, carcino-embryogenic antigen and epithelial membrane antigen. These markers were more positive to KCOT when compared to other cysts viz., dentigerous cyst and radicular cyst [4]. However, cytokeratin profile done on these tumours was not of diagnostic relevance [6].
Conclusion
This case is unique in itself as it represents two different types of cysts in a single oral cavity although individual cysts or multiple cysts of same histopathological features have been reported in literature. It is difficult to differentiate follicular variant of KCOT from a dentigerous cyst as it mimics the latter but with the help of clinical findings, radiographic and histopathological features, we could arrive at a definitive diagnosis. Furthermore, surgeons should be aware of these entities occurring simultaneously in a single jaw and once surgically excised should keep such patients under close follow-up to detect recurrence.
[1]. Wright JM, Vered M, Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Odontogenic and Maxillofacial BoneTumorsHead and Neck Pathology 2017 11(1):68-77.10.1007/s12105-017-0794-128247226 [Google Scholar] [CrossRef] [PubMed]
[2]. Cunha JF, Gomes CC, de Mesquita RA, Goulart EM, de Castro WH, Gomez RS, Clinicopathologic features associated with recurrence of the odontogenic keratocyst: a cohort retrospective analysisOral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2016 121(6):629-35.10.1016/j.oooo.2016.01.01527050804 [Google Scholar] [CrossRef] [PubMed]
[3]. Regezi JA, Sciubba JJ, Jordan RC, Dentigerous cysts. In Oral pathology: clinical pathologic correlations 2016 7th EditionElsevier Health Sciences; Saunders:250-255. [Google Scholar]
[4]. Tekkesin MS, Tuna EB, Olgac V, Aksakalli N, Alatlı C, Odontogenic lesions in a pediatric population: Review of the literature and presentation of 745 casesInternational Journal of Pediatric Otorhinolaryngology 2016 86:196-9.10.1016/j.ijporl.2016.05.01027260607 [Google Scholar] [CrossRef] [PubMed]
[5]. Lai RF, Li ZJ, Valuable radiographic tool for odontogenic jaw keratocyst diagnosis and surgical planningWest Indian Med J 2014 63(4):364-67.10.7727/wimj.2012.27025429483 [Google Scholar] [CrossRef] [PubMed]
[6]. Rao K, Kumar S, The use of enucleation and chemical cauterization (Carnoy’s) in the management of odontogenic keratocyst of the jawsIndian J Otolaryngol Head Neck Surg 2014 66(1):08-12.10.1007/s12070-012-0523-824605293 [Google Scholar] [CrossRef] [PubMed]