Jaffe Lichtenstein Type Polyostotic Fibrous Dysplasia with Unilateral Absent Testis
Anand Ramakrishnan1, Radha Kumar2, Kishore Narayan3, Santhosh Kumar4
1 Senior Resident, Department of Paediatrics, Saveetha Medical College and Hospital, Chennai, Tamil Nadu, India.
2 Professor, Department of Paediatrics, Saveetha Medical College and Hospital, Chennai, Tamil Nadu, India.
3 Associate Professor, Department of Paediatrics, Saveetha Medical College and Hospital, Chennai, Tamil Nadu, India.
4 Senior Resident, Department of Paediatrics, Saveetha Medical College and Hospital, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anand Ramakrishnan, C1-606, Purva Windermere Apartments, Thiruvalluvar 2nd Street, Pallikaranai, Chennai, Tamil Nadu, India.
E-mail: anand160988@gmail.com
Fibrous dysplasias are developmental bone disorders in which the medullary cavity is replaced by fibrous tissue. It can be monostotic involving a single bone or polyostotic involving multiple bones. Unlike the monostotic type, the polyostotic type of fibrous dysplasia is associated with non skeletal manifestations like café au lait macule and/or endocrine hyperfunction. The presence of endocrine involvement differentiates McCune Albright syndrome from Jaffe Lichtenstein syndrome. We hereby report a case of an 11-year-old male child presenting with polyostotic type of fibrous dysplasia involving bilateral femurs with café au lait macule having no endocrine disease consistent with the diagnosis of Jaffe Lichtenstein disease. He also had unilateral absent testis which is rarely reported in this syndrome.
Anorchia, Bisphosphonate, Café au lait, Cortical bone grafting
Case Report
An 11-year-old boy presented to the Paediatrics Department with left sided knee pain and abnormal gait. The symptoms were noticed since three years of age. The onset was insidious with no antecedent trauma. The symptoms were localised to the left side and no other bone or joint was involved. He was born to a non consanguinous couple at term, by normal vaginal delivery and there were no difficulties during delivery/no birth trauma and no perinatal complications. He attained age appropriate milestones. He had no other illness requiring hospitalisation/long term medications. There was no significant family history.
On examination he had tenderness in the left thigh just above his knee. There was no obvious bony deformity or signs of inflammation on palpation. His left lower limb was 1 cm shorter than his right lower limb (thigh segment), hence the gait abnormality. Neurological examination showed normal tone, power and reflexes. He did not have any weakness and restriction of movement. Examination of the joints were normal. He was noticed to have a café au lait macule in his neck measuring 4×1cm with irregular margins [Table/Fig-1]. His left testis was not palpable and he had underwent diagnostic laporotomy for the same at five years of age which could not detect the testis. He had no secondary sexual characters and right testicular volume was prepubertal. His anthropometry and blood pressure were within normal limits. He did not have any other musculoskeletal abnormality (deformity/tenderness at any other site).
Showing café au lait macule on the neck.

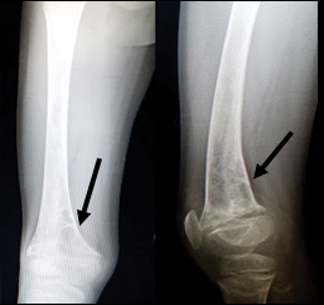
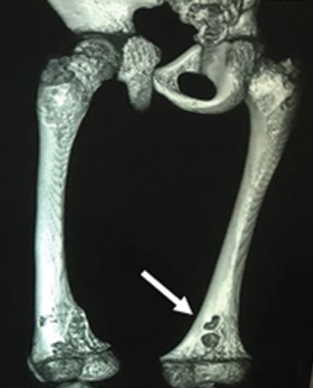
On radiological investigation, X-ray showed a radiolucent lytic lesion in his left and right femur [Table/Fig-2,3]. Differential diagnosis of a lytic bone lesion like adamantinoma, bone cyst, giant cell tumour, osteofibrous dyslasia and non ossifying fibroma were considered. Skeletal survey was normal ruling out other bone involvement. Computerised Tomograpy (CT) scan of the left lower limb showed diffuse sclerotic and lytic lesion with few areas of ground glass opacities in the left femur suggestive of fibrous dysplasia [Table/Fig-4]. Serum electrolytes including calcium and phosphate were normal. Serum alkaline phosphatase was elevated (581 mg/dL). He had no sexual precocity, normal height and weight and normal blood pressure ruling out endocrine (Gonodotrophins/Growth hormone and Cortisol respectively) involvement. Baseline thyroid function test and blood glucose were done which turned out to be normal. Hence, the patient was diagnosed as having Jaffe Lichtenstein syndrome (Polyostotic fibrous dysplasia with café au lait macule). The patient was started on calcium supplements and on bisphosphonate (weekly alendronate) therapy which was given for two months. The patient continued to be symptomatic with worsening pain and hence underwent cortical bone grafting. The patient was reviewed three weeks after surgery and had no surgery related complication. Limb mobilisation and rehabilitation will be started following his next visit.
X-ray showing radiolucent intra-medullary lesion in the metaphysis of left femur.

X-ray showing radiolucent lytic lesion in the distal metaphysis of right femur.
CT-scan showing lytic lesion in left femur.
Discussion
Fibrous dysplasias are benign lesions of the bone characterised by replacement of the normal medullary bone by immature bone and fibrous connective tissue due to abnormal osteoblast differentiation [1]. Von Recklinghausen first reported it in 1891 [2]. It was first described as a separate disease by Linchtenstein alone and Lichtenstein and Jaffe in 1938 and 1942 respectively [3,4].
It is a non inherited dysplastic disease of the bone which accounts for 2% of all bone tumours [5]. The defect has been localised to the long chain of chromosome 20, the affected gene being GNAS 1 (Guanine nucleotide binding protein α stimulating activity polypeptide). The main defect is the constitutional activation of the G protein encoded by GNAS 1. This results in overproduction of cAMP in the tissues affected [6]. cAMP affects the differentiation of osteoblast, melanocyte proliferation and endocrine function. Depending on the extent of involvement it is classified as monostotic and polyostotic types [7]. It is called monostotic when it involves a single bone and polyostotic when it involves multiple bones [8]. The monostotic form which is the commoner type accounts for 70% of the cases [9]. It frequently involves the ribs and the femur. The polyostotic form affects the craniofacial bones in addition to the ribs, tibia and femur [10]. The polyostotic type could be part of McCune Albright syndrome or Jaffe Lichtenstein syndrome.
The commoner monostotic type affects both sexes equally and is either incidentally detected or presents as gradually expanding bony swelling in the jaw, ribs or femur. The polyostotic type has a female predominance and can have varied presentations-
1. Multiple bone involvement with pathological fractures
2. Jaffe Lichtenstein syndrome- bony involvement with café au lait macule
3. McCune Albright syndrome- triad of polyostotic fibrous dysplasia, café au lait macule and endocrine hyperactivity characterised by precocious puberty, hyperthyroidism, acromegaly and hyperparathyroidism [11].
The café au lait macule is usually found ipsilateral to the bone involvement and is characterised by a jagged border (coast of Maine) which differentiates it from neurofibromatosis [11]. The present patient had polyostotic disease of both the right and left femurs along with a café au lait macule on the neck. There is no known association of testicular agenesis with fibrous dysplasia. Raus I et al., has reported a case of McCune Albright syndrome with unilateral testicular agenesis [12].
The disease is diagnosed by its clinical presentation and radiological findings. Kransdorf M et al., described the radiological features of fibrous dysplasia. The lesions are eccentrically located in the medullary cavity with a ground glass appearance. The lesion merges indistinctly with the surrounding normal bone and has a sclerotic reactive rind [13]. CT is the best imaging modality to detect these changes; however, even X-rays can be used, though they are less effective in delineating the lesions. Serum alkaline phosphatase is elevated in about a third of the cases and extensive bone involvement leads to hyperphosphaturia and hypophosphatemia [14].
Small monostotic lesions can be followed up without any treatment as they usually remain silent. Bisphosphonate therapy decreases the risk of fracture and reduces pain [7]. Surgical intervention is required for biopsy, stabilisation of fractures, correcting deformities and to perform cortical bone grafting [7].
A multicentric study conducted by European Paediatric Orthopaedic Society concluded that the outcome of monostotic fibrous dysplasia is usually good with or without treatment and polyostotic type particularly McCune Albright type had the worst outcome with a majority requiring multiple corrective surgeries [15].
Conclusion
Index case presented with symptomatic single bone disease and a café au lait macule. Evaluation showed involvement of both femur, active disease suggested by elevated alkaline phosphatase and absent endocrine involvement ruling out McCune Albright syndrome. The management and prognosis of fibrous dysplasia depends on its type and presence/absence of associated syndrome, highlighting the need for detailed clinical, laboratory and radiological evaluation in all children with fibrous dysplasia.
[1]. Hanifi B, Samil KS, Yasar C, Cengiz C, Ercan A, Ramazan D, Craniofacial fibrous dysplasiaClin Imaging 2013 37(6):1109-15.10.1016/j.clinimag.2013.01.01023993753 [Google Scholar] [CrossRef] [PubMed]
[2]. Von Recklinghausen, Die fibroseoderdeformierendeOstitis, die Osteomalacie und die osteoplastischeCarcinose in ihrengegenseitigenBeziehungenIn: Festschrift Rudolf Virchow zum 13 1891 Berlin, GermanyGeorg Reimer Verlag [Google Scholar]
[3]. Lichtenstein L, Polyostotic fibrous dysplasiaArch Surg 1938 36(5):874-98.10.1001/archsurg.1938.01190230153012 [Google Scholar] [CrossRef]
[4]. Lichtenstein L, Jaffe HL, Fibrous dysplasia of bone: a condition affecting one, several or many bones, the graver cases of which may present abnormal pigmentation of skin, premature sexual development, hyperthyroidism or still other extraskeletal abnormalitiesArch Pathol 1942 33:777-816. [Google Scholar]
[5]. Tinoco P, Carlos J, Pereira O, Boechat de Carmo FS, Ruela KP, Fibrous dysplasia of maxillary sinusInternational Archives of Otorhinolaryngology 2009 13:02 [Google Scholar]
[6]. Rajendran R, Sivapathasundharam B, Shafer’sTextbook of Oral Pathology 2012 7th editionElsevier Publication [Google Scholar]
[7]. DiCaprio MR, Enneking William F, Fibrous dysplasia. Pathophysiology, evaluation, and treatmentJ Bone Joint Surg Am 2005 87:1848-64.10.2106/00004623-200508000-00028 [Google Scholar] [CrossRef]
[8]. Feller L, Wood NH, Khammissa RAG, Lemmer J, Raubenheimer EJ, The nature of fibrous dysplasiaHead Face Med 2009 5:2210.1186/1746-160X-5-2219895712 [Google Scholar] [CrossRef] [PubMed]
[9]. Ricalde P, Horswell BB, Craniofacial fibrous dysplasia of the fronto-orbital region: a case series andliterature reviewJ Oral Maxillofac Surg 2001 59(2):157-67.10.1053/joms.2001.2048711213984 [Google Scholar] [CrossRef] [PubMed]
[10]. Favus MJ, Vokes TJ, Paget disease and other dysplasias of bone. In: Fauci AS, Longo DL, Kasper DL, et al., edsHarrison’s Principles of Internal Medicine 2008 17th edNew York, NYThe McGraw-Hill Companies,Inc [Google Scholar]
[11]. Dumitrescu CE, Collins MT, McCune-AlbrightSyndromeOrphanet Journal of Rare Diseases 2008 3:01-12.10.1186/1750-1172-3-1218489744 [Google Scholar] [CrossRef] [PubMed]
[12]. Raus I, Coroiu RE, Mccune Albright syndrome-association of fibrous dysplasia, café-au-lait skin spots and hyperthyroidism-case reportClujul Med 2016 89:559-64.10.15386/cjmed-62427857528 [Google Scholar] [CrossRef] [PubMed]
[13]. Kransdorf M, Moser RP, GIlkey FW, From the archives of AFIPRadiographics 1990 10:310.1148/radiographics.10.3.21883112188311 [Google Scholar] [CrossRef] [PubMed]
[14]. Regezi Scuba Jordan, Oral Pathology Clinical Pathologic Correlations5th editionElsevier Publication:289-308. [Google Scholar]
[15]. Ippolito E, Bray EW, Corsi A, De Maio F, Exner UG, Robey PG, Natural history and treatment of fibrous dysplasia of bone: a multicenter clinicopathologic study promoted by the European Peadiatric Orthopaedic SocietyJ Pediatr Orthop B 2003 12:155-77.10.1097/01202412-200305000-00001 [Google Scholar] [CrossRef]