Communication through speech is a multi-dimensional signal that elicits a linguistic association [1]. Speech is an important function of the stomatognathic system, which uses the oral cavity as an instrument. Teeth, alveolus, palate are static components of speech articulation whereas tongue, lip and velum are dynamic components [2,3]. Any alteration or loss of these structures therein will adversely affect speech sounds produced. This problem exacerbates many folds in edentulous patients as there will be loss of all teeth and associated structures, resulting in poor speech sounds, aesthetics along with difficulty in mastication [4].
The complete denturer is the most common dental treatment modality for the completely edentulous situation [4], but it alters the intraoral anatomy, physiology and even brain function activity [5]. During its fabrication phonetic evaluation is frequently neglected and more emphasis is placed on other key elements of denture treatment such as aesthetics, function, and comfort [6-9]. This results in unpleasant and embarrassing situation to patient while using complete dentures due to improper speech. It is generally assumed that patients will successfully adapt to new dentures within few weeks [10-14]. But, it may take longer to adopt for changes in palatal contours of maxillary complete dentures, especially for elderly patients [13]. Unfortunately, some patients never acclimate to the new dentures and continue to experience difficulties in pronouncing intelligible sounds, especially the sibilant sounds [15-18].
Few methods were proposed in the literature to improve the speech intelligibility in complete denture patients, which includes duplication of palatal rugae, palatographic recontouring of the palate, incorporation of roughness in the anterior part of palate [3]. Since the palate is completely covered, the oral environment gets altered, the space available to the tongue gets reduced along with masticatory efficiency and disturb sensorimotor function [19]. Various oral sensory receptors such as mechanoreceptors, receptors for algethesia, thermesthesia is present in the anterior region of the palate [20]. While speaking the tongue is not contacting the palate directly, thus resulting in reduced speech intelligibility. Various researchers had conducted studies [12,14,21-23] on phonetics in relation to complete denture, in an attempt to improvise the clarity and intelligibility of speech of the edentulous patients who are acclimatising to new dentures.
Of all above methods, functionally modified palatal surface complete denture had proved to be of little help in improving speech. But still, no significant progresses have been made in this field. However, Koike T et al., described that the small-opening type of palatal coverage complete denture improved the oral perception and demonstrated sufficient retention force [24]. This opening extended from the incisive papilla to the third palatal rugae, as a large number of tactile and pressure sensory points are located in this area [24-26], so while speaking when tongue comes in direct contact with the palate, the brain would be activated and the speech produced would be clearer.
Taking this into consideration present study was planned with the aim to compare the speech intelligibility of complete dentures wearers having Small Opening (SO) in anterior palatal base, with the conventional complete denture, without denture and with Functionally Contoured Modified Palate (FCMP) complete denture.
Materials and Methods
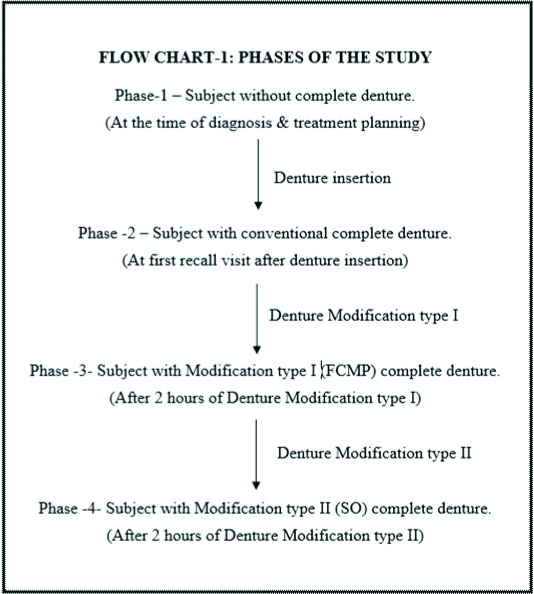
The present in vivo study was carried out in the Department of Prosthodontics, Career P G Institute of Dental Sciences and Hospital, Lucknow, Uttar Pradesh, India, for a period of 24 months (July 2014 to July 2016). In this study, the quality of speech sounds (i.e., pitch and intensity) was tested in completely edentulous patients in four phases (phase one without denture, phase two with conventional complete denture, phase three with functionally contoured palatal base denture and phase four with dentures having small opening in the anterior part of the palatal base). Forty completely edentulous patients participated. During the period of patient selection total 70 patients were selected following inclusion and exclusion criteria.
Inclusion Criteria
Cooperative patient, completely edentulous patients of same ethnicity and area, patients with completely healed well rounded ridges (evaluated using the method described by Ohnuki M et al., [27]), no history of tongue tie and related treatment, edentulous patient with moderate level of education, patients with good hearing (thresholds better than 20 dB in their poorer ear).
Exclusion Criteria
Uncooperative patient; patient with any congenital or acquired maxillofacial defects; patient with any intraoral or extraoral pathology; edentulous patients with any neuro-muscular defects; patients with visual disabilities. With five subjects the pilot study was conducted and following this sample size was calculated by fixing the confidence interval (10) and confidence level (95%). On the basis of above decision, sample size was calculated as 40. Then the subjects were divided into two groups. Group A: 60 to 70 years and Group B: Above 70 years [Table/Fig-1] with 20 subjects in each.
Distribution of subjects.
| Group | Age group | N | % |
|---|
| Group A | 60-70 years | 20 | 50.0 |
| Group B | ≥70 years | 20 | 50.0 |
| Total | 40 | 100.0 |
Written informed consent was obtained from each patient and the ethical clearance was obtained from the Institutional Ethical Committee. For all the subjects complete dentures (maxillary and mandibular) were constructed following standardised protocol suggested by Boucher [4]. The shape of artificial acrylic teeth were modified and arranged in Lingualized Occlusion (LO) to reduce and minimise horizontal forces on the dentures [28,29].
Speech Stimulus, for sounds recording, used in the study were linguopalatal sounds e.g., t, d, l, n in which the tongue made active contact with the palate and other linguopalatal sounds s, sh, ch, jh, which are formed by passive contact of tongue with the palate. These speech sounds were in local language (Hindi) and consists of-Phrases, words loaded with phonemes. eg. Saraswati, Salma, Tata, Drum, Damru, Nal.
Recording of Speech Samples
Recording was done in a sound proof room (semi-anechoic room) using a microphone (Logitech Pvt. ltd., - Logitech Audio Group-Business Office, 4700 NW Camas Meadows Drive Camas, WA 98607) at a sampling frequency of 16 kHz and quantized with 16 bit and MP3 recording system (Praat sound System software-Praat is a scientific tool for studying linguistics). The subjects were asked to sit at distance of about 30 cm in front of the microphone in a sound proof room. Before starting recording; training was given to each patient with the help of pictorial representation chart.
Modifications made in Complete Denture
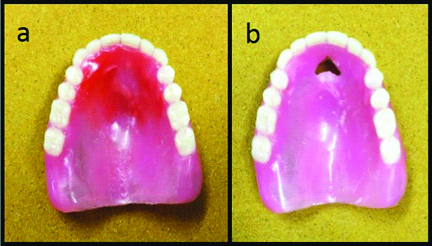
Modification Type I- FCMP [Table/Fig-2a]. Mouth temperature wax (Korecta No.4 (extra soft) {Kerr Restoratives 1717 West Collins Orange, CA 92867} - Thermoplastic materials, which flow readily at mouth temperature and are relatively soft even at room temperature) was used to functionally contour the palatal vault of the maxillary complete denture. For this patients were asked to swallow and close and were involved in conversation.
Modification Type II- Small-Opening (SO) in the anterior region of the palatal base [Table/Fig-2b]. This opening extended from the incisive papilla to the third palatal rugae [24]. The opening was made with the acrylic trimming burs and edges of the opening were bevelled towards the tissue and corners were rounded. All subjects were tested for speech analysis in four phases [Table/Fig-3].
a) Modification Type I- Functionally Contoured Modified Palate (FCMP) of the maxillary complete denture; b) Modification Type II-Small-Opening (SO) in the anterior region of the palatal base of the maxillary complete denture.
Assessment of the Sound Samples
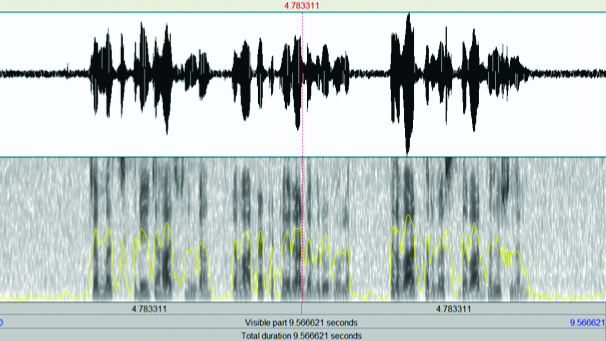
The recorded sound samples of each subject at different phases were analysed by using-Objective method (Quantitative analysis) and Subjective method (Qualitative analysis). Quantitative analysis was performed using Praat software which was used for recording the sound samples. It displays each sample in the form of a spectrograph [Table/Fig-4] (sound waves). The spectrograph provided the details of the mean frequencies (pitch of sound) and mean decibel (intensity/loudness of sound) of each of the recordings. These sound frequencies and sound decibels were tabulated and analysed statistically to determine at which phase the intelligibility of the sound was best. Qualitative analysis was done by a group of experienced speech analysts, consists of ENT surgeon, speech therapist and prosthodontist. The 5 point Likert’s scale was used for judging the clarity of the speech sounds at each phase. To avoid individual bias the sound samples were played randomly without informing the phase. Likert’s scale used for speech assessment consists of 5 points –with rating from 0 to 4. Clear Sounds were marked by 4 followed by 3 –Normal but Slightly Unclear Sounds, 2 – Requires Effort to Understand, 1 – Can Understand Only If Content Is Known, 0- Indistinct Sounds.
Spectrograph of sound sample.
Statistical Analysis
The data so obtained was tabulated and statistically analysed. In statistical analysis, the data was summarised as Mean±SD (Standard Deviation). The Groups were compared by one-way analysis of variance (ANOVA) of repeated measures and the F- and p-values were calculated. A two-sided (α=2) p-value less than 0.05 (p<0.05) was considered statistically significant. Qualitative data was analysed with Mann-Whitney U test. The statistical analyses were performed on SPSS software (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp).
Results
After statistical analysis, on analysing the results of Pitch in group A and B, it was found that the value of pitch was maximum in phase four SO Modification type II (187.93±24.22 and 191.48±23.98 respectively) with more clarity in sound compared to the other phases. One-way ANOVA (repeated measures) showed that mean pitch difference among four phases was statistically significant (F=23.70 and F=13.70, d.f=3, p<0.001). Post-hoc multiple comparison depicts the significant difference (p<0.05) in various pairs [Table/Fig-5,6].
Comparison of pitch in Group A and B between different phases.
| Variable | Without denture (N=20) | With denture (N=20) | FCMP modification I (N=20) | SO modification II (N=20) | Significance |
|---|
| Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B |
|---|
| Pitch | 168.29±24.15 | 177.77±27.20 | 173.94±22.57 | 181.12±24.66 | 179.65±23.33 | 184.30±26.18 | 187.93±24.22 | 191.48±23.98 | F=23.70,d.f=3,p<0.001 | F=13.70,d.f=3,p<0.001 |
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
Post-hoc multiple comparisons of pitch in Group A and B between different phases.
| BiComparisons using Bonferroni Post-Hoc test | Without denture | With denture | FCMP modification I (N=20) | SO modification II (N=20) |
|---|
| Mean Diff. | p-value | Mean Diff. | p-value | Mean Diff. | p-value | Mean Diff. | p-value |
|---|
| Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B |
|---|
| Without denture | | | 5.65 | 3.349 | 0.005 | 0.454 | 11.354 | 6.532 | 0.006 | 0.115 | 19.637 | 13.711 | <0.001 | 0.002 |
| With denture | | | | | 5.704 | 3.183 | 0.073 | 0.388 | 13.987 | 10.362 | <0.001 | 0.001 |
| FCMP modification I | | | | | | | 8.282 | 7.179 | <0.001 | 0.003 |
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
Similarly, Intensity was also highest in phase four SO Modification type II in both group (group A- 75.84±6.34 and group B -74.99±6.74). One-way ANOVA (repeated measures) shows that the mean pitch difference among four phases was statistically significant (F=10.12 and F=3.66, d.f=3,p<0.001). Post-hoc multiple comparison depicts the significant difference (p<0.05) in various pairs as mentioned in [Table/Fig-7,8].
Comparison of intensity in Group A and B between different phases.
| Variable | Without denture (N=20) | With denture (N=20) | FCMP modification I (N=20) | SO modification II (N=20) | Significance |
|---|
| Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B |
|---|
| Intensity | 68.24±6.83 | 70.13±7.59 | 69.13±4.37 | 71.62±5.90 | 72.18±8.63 | 72.80±8.12 | 75.84±6.34 | 74.99±6.74 | F=10.12,d.f=3, p<0.001 | F=3.66,d.f=3, p<0.017 |
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
Post-hoc multiple comparisons of intensity in Group A and B between different phases.
| BiComparisons using Bonferroni Post-Hoc test | Without denture | With denture | FCMP modification I (N=20) | SO modification II (N=20) |
|---|
| Mean Diff. | p-value | Mean Diff. | p-value | Mean Diff. | p-value | Mean Diff. | p-value |
|---|
| | Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B | Group A | Group B |
|---|
| Without denture | | | 0.887 | 1.486 | 0.001 | 0.001 | 3.937 | 2.667 | 0.211 | 0.001 | 7.603 | 4.862 | <0.001 | 0.027 |
| With denture | | | | | 3.05 | 1.182 | 0.709 | 0.001 | 6.716 | 3.377 | <0.001 | 0.065 |
| FCMP modification I | | | | | | | 3.667 | 2.196 | 0.075 | 0.405 |
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
The qualitative analysis of speech sound was done by evaluating the Likert scale ratings, given by group of experts, using Mann-Whitney U test. The scores given by experts to sound samples of different phases differ significantly from each other but there was no significant difference between the ratings by judges to the sound samples of group A and B in a particular phase (p>.05) [Table/Fig-9]. On comparing the ratings for group A and B shows that phase four ratings were highest for both groups (3.18, 3.20 respectively).
Mann-Whitney U comparisons of Likert scale rating by experts for Group A and B.
| Groups | Without denture (N=20) | With denture (N=20) | FCMP modification I (N=20) | SO modification II (N=20) |
|---|
| Group A | 1.32±0.83 | 1.92±0.74 | 2.40±0.81 | 3.18±0.97 |
| Group B | 1.27±0.82 | 1.97±0.82 | 2.53±0.57 | 3.20±0.73 |
| Mean Rank of Group A and Group B | 61.38and 59.62 | 59.93and 61.08 | 59.10and 61.90 | 61.91and 59.09 |
| Significance(Mann-Whitney U) | =1747.00,p=0.765 | 1765.50,p=0.845 | 1716.00,p=0.616 | 1715.50,p=0.628 |
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
Discussion
The knowledge of speech phenomenon and mechanism of its production are essential features of comprehensive dental treatment, especially, in completely edentulous patient due to altered articulatory cavity which produces a marked effect on the speech pattern. Speech is basically combination of sounds, consists of Vowels, Diphthongs, Consonants and Combinations [17,28]. Exploration of linguistic research has revealed documentation on tongue-palate contact importance for phonation. Eslamian and Leilazpour, analysed the importance of tongue-palate contact and confirmed that contact between the tongue-palate was mostly at the anterior and lateral parts of the palate and least at mid palatal area [30]. Fiona Gibbon FE et al., compared tongue-palate contact patterns for alveolar (/t/,/d/) with those for the nasal stop/n/using Electropalatography (EPG) and found “t” “d” “n” was under anterior constriction EPG frames [31]. Different studies refer to an increase of the quality of speech production after a period of habituation to prostheses [14,32-34]. Ninety per cent of the patients seem to reach a steady state of speech quality after a period of at least 4 weeks [14, 34].
Other studies assume complete loss of teeth can cause a persistent speech disorder by altering dental articulation areas. This severely reduces the quality of speech [35]. Particularly, the alteration of frontal maxillary morphology leads to impairment of speech production [36].
Several authors suggested that missing proprioceptors [20], change in sensory stimulus, change in oral cavity dimension, gradual loss of hearing (ageing process) might be responsible for problems in speech sound production immediately post denture insertion [37-41].
After realising this authors emphasised upon the importance of modifying palatal vaults of maxillary complete dentures to improve speech [9,11,13-17,25,26,42-47]. Some of them have suggested arbitrary changes in shape and thickness [26], incorporation of palatal rugae [3,46,47] change in material of palatal part of the denture and functionally modify [11,14,25,26,43] palatal surfaces of the maxillary denture.
However, most of the authors advocated that in functionally modified palatal surfaces of the maxillary denture, tongue does not “have” to adapt itself to the changed environment to produce normal speech [14,25,26,48]. After analysing the literature it can be impressed that the functionally modified palatal surface of maxillary denture proved to be beneficial in enhancing the quality of speech production with certain period of adaptation [14,34,49]. But the conventional denture covers whole of the palate, and it prevents the direct contact of the tongue with the anterior part of the palate during speech and other oral functions. As a result slowly the proprioceptors present there gets deteriorated because of continuous pressure, there is loss and degeneration of Merkel cells, mechanoreceptors, disturb sensorimotor function [19], prolonged bolus propulsion time, decreased oral perception [25] and above all reduced speech intelligibility. Koike T et al., demonstrated that a small-opening in the palatal surface of maxillary denture improve the oral perception and demonstrated sufficient retention force [24].
In the present study, hypothesis was proposed and attempt was made to improve the quality of speech sounds produced immediately post denture insertion by making a small opening as suggested by the Koike T et al., and its effectiveness was compared with conventional complete denture and denture with functionally contoured palatal vault in four phases.
In this study to compare speech intelligibility Praat Linguistic Software (version 5.3.56) was used. This software helped in spectral analysis of the sound samples similar to the previous studies based on linguistic software for speech analysis by Adaki R et al., Runte C et al., and Hamada JM and Kusai B [3,36,47]. Spectral analysis had been used to examine the effects of dental prostheses on speech sound production. Sound event can be split into three dimensions: frequency (pitch), amplitude (intensity), and chronologic sequence. The data obtained can be visualized in 2-dimensional Cartesian coordinates with the colour or grey shade as the third dimension [47,50]. In this study the pitch and intensity of sound samples were assessed for quantitative analysis. The use of Praat software provided objective information in relation to the sound samples recorded at different phases of the study.
The frequency of a sound wave is measured as the number of complete back-and-forth vibrations of a particle of the medium per unit of time. On comparing the values of four phases it was depicted that the frequency of sound was least without denture i.e., phase one, than any other phase. Similarly, the scale for measuring intensity/loudness of sound is the decibel scale. It was observed that in both the groups in phase one the intensity of sound was least i.e., without denture.
Without a dental prosthesis inserted, in both groups the speech intelligibility (frequency and intensity) was significantly lower compared to any other phase with dentures inserted. When the phase two was analysed with phase three the speech intelligibility was less and it showed that functional contouring (modification type I) of the palate improved the speech sound quality. The configuration of the palatal contour functionally developed in this study conforms to the one observed by Tanaka in his study [14]. These findings were in association with the previous studies conducted by Zakkula S et al., Kong HJ and Hansen CA, Tanaka H, Goyal BK and Greenstein P [6,11,14,43]. In agreement with the present study, with dentures inserted, an improvement in the speech intelligibility of patients with an edentulous maxillary arch was stated in studies that used a perceptual rating of speech intelligibility or spectral analysis to assess single distorted sounds [33].
The data so obtained showed that the speech intelligibility increased in phase four and three. This observation is understandable because the modified palatal surface by functional contouring (modification type I) of the denture offers a more physiologic contact of tongue during enunciation of speech as compared to the smooth, highly polished, arbitrarily contoured palatal surface of a conventional denture. But still speech produced phase three was but slightly unclear compared to phase four. This may be due to the fact that the even though the palate was functionally modified but tongue had to work against the artificial surface. It was quite possible that if the tongue was allowed to adapt with the change environment the speech produced may be clear.
In phase four where small opening was made in the anterior part of the palate (modification type II) had provided “natural” tactile sensation to the tongue thus resulting in even better speech intelligibility immediately after denture insertion compared to functional contouring [43]. This small opening allowed direct contact of the tongue with the palate resulting in production of sounds with high frequency and intensity, thus making it very clear. Similar results were depicted by the Likert chart with highest marking of 4 by the experts.
Conversely, in phase two and one the sound was not clear and can be understood with effort and only if the content was known previously. These results are in agreement with results reported by Pound, Palmer [22,40] and others Zakkula S et., Kong HJ and Hansen a, Tanaka H [6,11,14] where palatogram or functionally modified palate was considered best for speech sound production with adaptation time. By customising palatal contours of a maxillary denture to the tongue, the patient may easily adapt to the definitive denture contour, which in turn shortens the adjustment period for the achievement of proper enunciation [47].
Here in the present study the newer concept of making a small opening in the anterior part of the palate i.e. modification type II resulted in speech sound production which were very clear and without any adaptation period thus proved its advantage over other methods.
On comparing group A (phase-one, two, three, four) with group B (phase-one, two, three, four) on the basis of pitch and intensity, the statistically insignificant results were found, thus indicating that there were no changes of speech sounds (pitch and intensity) in terms of age. The variation in speech intelligibility was specifically related to the altered oral environment in the edentulous patients either with loss of teeth or dentures, with correct dental prosthesis clear sounds could be produced with adaptation period but with modification 2 as described in the present study the adaptation period would be eliminated and patients speech intelligibility will be high with very clear sounds.
Phase four had maximum scores (group A- 3.18±0.97, group B- 3.20±0.73) in perceptual (qualitative) analysis by 3 judges, for overall speech sounds intelligibility, in both the groups’. The sound samples in this phase were normal and experts categorised most samples very clear. They were able to identify an improved sharpness/clarity in each of the sounds and scored maximum samples 4 and very limited samples three. However, judges invariably categorized the maximum sounds of phase one and two as “Not Clear Sounds (NC)” and “can Understand Only If Content Is Known (C if)” in both groups with score 0 and 1 respectively. The phase three sound samples were better equally, the scores given by experts were three and two illustrating that the sound was normal but only Slightly Unclear Sounds (CL) in majority of the case and few samples Requires Effort to Understand (Re AV). Though there was an improvement in the clarity of speech sounds, the judges could not arrive at a common consensus and hence, varied in their opinion. These scores were in agreement with the other studies where functional countering of the palate was proved to be beneficial compared to other methods to enhance the speech intelligibility [6,11,14,22,40]. These samples would have scored four with very clear marking if adaptation time was provided.
This is the advantages of the Likert’s scale wherein value is given even to the relative opinion/relative preference of an individual. Since it is not just the theoretical success, in terms of frequency and decibels, but the listeners’ satisfaction in the clarity of speech that is also critical in determining the success of a prosthesis with respect to speech intelligibility [38,51]. The combined rating given by all the judges for the samples of each group showed that, they felt there was an improvement in the clarity of the sounds after functional contouring of the palatal vault, but this got enhanced with modification type II in phase four. This enhanced improvement may be due to the orosensory feedback by the tongue-palate direct contact relation hence, improvement in the quality of speech. Thus, the quantitative results were reaffirmed by the qualitative results that small opening in the anterior part of the palatal vault of maxillary complete dentures significantly improves the speech intelligibility.
Limitation
A varying number of factors may have had an effect on speech production such as position of teeth, denture flange thickness, Posterior palatal seal etc. Along with this retention is also an important factor to be visualised in the current study, although a small anterior palate opening does reduced retention force, but retention was still sufficient for general oral requirements [24] and also patient selection was very important, only patients where resorption of alveolar bone in the anterior maxilla was not severe were selected. Further studies are necessary to evaluate the effects of proposed modification in dentures for longer duration of time and its adaptation on all parameters and satisfaction of the patients.
Conclusion
Within the scope and limitations of this in vivo study, it can be concluded that speech intelligibility after denture insertion was found more, it was better in modified dentures (Modification type I and II). Relative improvement in the clarity of speech sounds was noticed in dentures with Modification I and significant improvement was observed in complete dentures with Modification II (Small-Opening (SO) in the anterior region of the palatal base), speech sound produced were very clear and without any adaptation period, immediately after denture insertion. This design should be used while fabricating complete dentures, owing to the situation where resorption of alveolar bone in the anterior maxilla is not severe and methods of managing lateral forces are incorporated.
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening
*OPT: Oral perception time; FCMP: Functionally contoured modified palate; SO: Small opening