Indwelling J Ureteral Stents Associated Asymptomatic Bacteraemia Caused by Multidrug Resistant Strain of Kocuria kristinae
Muhammed A.P. Manzoor1, K.S Shabeena2, M Mujeeburahiman3, Altaf Khan4
1 Senior Research Fellow, Department of Urology, Yenepoya Research Centre, Yenepoya University, Mangalore, Karnataka, India.
2 Research Scholar, Yenepoya Research Centre, Yenepoya University, Mangalore, Karnataka, India.
3 Professor, Department of Urology, Yenepoya University, Mangalore, Karnataka, India.
4 Associate Professor, Department of Urology, Yenepoya University, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mr. Muhammed A.P. Manzoor, Senior Research Fellow, Department of Urology, Yenepoya Research Centre, Yenepoya University, Seed Grant (YU/Seed grant/2011-019), Deralakatte, Mangalore-575018, Karnataka, India.
E-mail: manzoorapkdy@gmail.com
Kocuria kristinae is a Gram positive non pathogenic bacterium belonging to the family of micrococcacae. It may cause opportunistic infections in patients with indwelling devices and severe underlying diseases. Indwelling double J ureteral stent is commonly used in urological practice and bacterial colonisation in the ureteral stent plays an important role in the pathogenesis of stent associated infection. Here, we report a rare case of bacteraemia by Kocuria kristinae. Antimicrobial susceptibility testing was performed by Kirby Bauer disc diffusion method. The isolate were found to be multidrug resistant. Regular surveillance of drug resistance is of utmost importance to minimise the spread of infections.
Antimicrobial susceptibility, Renal stones, Ureteroscopic lithotripsy
Case Report
A 46-year-old male patient presented to the Urology Department with right flank pain radiating to the right lower quadrant since four weeks. The patient did not report fever or bowel and bladder dysfunction. The patient had a similar pain in the right flank five years ago and it was diagnosed as renal stones, and the patient had not underwent any treatment or conservative management. No history of urolithiasis was recorded in the family. The patient underwent a baseline assessment including a detailed medical history, physical examination, urinalysis, complete blood examination, renal function test, ultrasound and X-ray of Kidney, Ureter and Bladder (KUB). The blood examination showed neutrophils 78%, lymphocytes 13%, monocytes 8% and eosinophils 1%. The biochemical parameters were in normal range. Other investigations such as total protein 7.8 mg/dL, serum albumin 3.7 mg/dL, serum globulin 3.9 mg/dL and albumin globulin ratio 0.9 mg/dL. All the other blood parameters were normal. The preoperative urine analysis showed negative urine culture. The urine appeared pale yellow. Pus cells, red blood cells and albumin were absent in urine and urine pH was 6.24. No evidence of casts and crystals were found. Ultrasound KUB showed right 9x6 mm Pelvi Ureteric Junction (PUJ) calculi.
The patient received prophylactic antibiotic levofloxacin (500 mg) for five days orally before the procedure. Ureteroscopic lithotripsy was performed and stent was inserted. Stent made of polyurethane was inserted retrograde endoscopically under fluoroscopic guidance. The post operative urinalysis showed no evidence of bacteria. The duration of stenting was 15 days and the stent was removed in the operating room under aseptic conditions. After the stent removal, 1 to 3 cm of the tip located in the bladder was cut aseptically and immediately inoculated into MacConkey agar and incubated aerobically at 37oC for 18 to 24 hours. After incubation, each separate morphological colony type was counted using a digital colony counter. Gram staining of the culture revealed the cells to be Gram positive cocci.
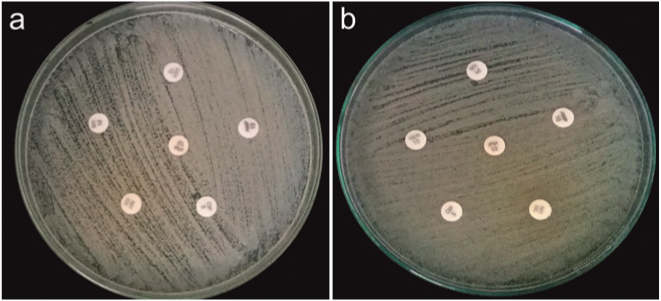
The bacteria were identified using Phoenix 100 automated system (BACTEC 9120) [1]. All the specimens were handled according to the clinical microbiology laboratory standard operating procedures. Antimicrobial susceptibility testing was performed using Kirby Bauer disc diffusion method on Muller Hinton agar using commercial antimicrobial disks [Table/Fig-1]. The results were expressed as Susceptible (S), Intermediate (I), or Resistant (R) according to the criteria of the clinical laboratory standards. Eighteen antibiotics with a broad range of mechanisms of action, including drugs that target cell wall, nucleic acid and protein were selected [Table/Fig-2]. The isolate was found to be resistant to all the tested antibiotics. The patient was discharged in satisfactory condition and follow-up was done for six months.
Drug sensitivity pattern of Kocuria kristinae showing resistance to antibiotics.
List of all antibiotics used in the study.
| Abbreviation | Antibiotic | Concentration (mcg) | Class | Main mechanism of action |
|---|
| AMK | Amikacin | 30 | Amioglycoside | Protein synthesis |
| AMP | Ampicillin | 10 | Aminopenicillin | Cell wall synthesis |
| GEN | Gentamycin | 10 | Amioglycoside | Protein synthesis |
| VA | Vancomycin | 30 | Glycopeptide | Cell wall synthesis |
| IPM | Imipenem | 10 | Carbapenem | Cell wall synthesis |
| AZM | Azithromycin | 15 | Macrolide | Protein synthesis inhibitors |
| NA | Nalidixic acid | 30 | Quinolone | Cellular deoxyribonucleic acid |
| E | Erythromycin | 15 | Macrolide | Protein synthesis |
| OX | Oxacillin | 1 | Penicillin | Cell wall synthesis |
| PIP | Piperacillin | 100 | Ureidopenicillin | Cell wall synthesis |
| TET | Tetracycline | 30 | Polyketide | Protein synthesis |
| CPR | Ciprofloxacin | 5 | Fluoroquinolone | Gyrase |
| CTX | Cefotaxime | 30 | Cephalosporin | Cell wall synthesis |
| CD | Clindamycin | 2 | Lincomycin | Protein synthesis |
| TOB | Tobramycin | 10 | Aminoglycoside | 30S and 50S ribosome |
| P | Penicillin G | 10 | Penicillin | Cell wall synthesis |
| NIT | Nitrofurantoin | 300 | Nitrofuran | Deoxyribonucleic acid |
| CEP | Cefepime | 30 | Cephalosporin | Cell wall synthesis |
Discussion
Kocuria is a Gram positive coccoid bacteria belonging to phylum Actinobacteria that are catalase positive and coagulase negative [2]. These bacteria are normally found in the skin and mucosa of humans and are rarely seen in clinical specimens. However, it may cause opportunistic infections in patients with indwelling devices and severe underlying diseases [3]. In addition, knowledge concerning the properties associated with Kocuria kristinae is limited [4]. However, reports showed that Kocuria kristinae can also be associated with the cases of catheter associated bacteraemia which was caused by this species in chronically ill patients [5-7]. As the use of indwelling ureteral stents has increased, the stent associated infection has also become more frequent. However, no case of an indwelling J ureteral stent infection with Kocuria kristinae has been reported. Present patient was treated for ureteric calculi and implanted with a J ureteral stents, which can be correlated somewhere with the association between indwelling devices and Kocuria kristinae. Here, we describe a case of indwelling J ureteral stent bacteraemia due to Kocuria kristinae in an adult man with right PUJ calculi. Antibiotic susceptibility testing was performed by Kirby Bauer disc diffusion method.
Understanding the microorganisms involved in the stent colonisation and their sensitivity profile will help in better treatment regime. Present patient’s isolate was found to be highly resistant to all the drugs as determined by disk diffusion method. The isolate was found to be resistant to various classes of antibiotics including penicillins, ureidopenicillin, amioglycosides, cephalosporins, and fluoroquinolones etc. However, the previous reports showed that Kocuria kristinae were susceptible to many commonly used antibiotics, including penicillins, clindamycin, vancomycin and fluoroquinolones [5,8].
Kocuria kristinae infections and its clinical spectrum will become clearer in near future with more reports [3]. Multidrug resistant bacteria are a major concern and therefore, precautions should be taken against it. Regular disease surveillance and rapid diagnostics to cut unnecessary use of antibiotics will be necessary in this regard.
With the high incidence of kidney stones and other urological diseases in our population there is an increased need for ureteral stent placement [9,10]. As the use of indwelling ureteral stents has increased, the stent associated infection has also become more frequent [11]. Bacterial colonisation in the stent plays an important role in the pathogenesis of stent associated bacteraemia.
Conclusion
Kocuria kristinae associated clinical infections are an emerging health concern and further care should be taken for proper administration of antibiotic treatment as they are intrinsically multidrug resistant.
[1]. Stefaniuk E, Baraniak A, Gniadkowski M, Hryniewicz W, Evaluation of the BD phoenix automated identification and susceptibility testing system in clinical microbiology laboratory practiceEur J Clin Microbiol Infect Dis 2003 22:479-85.10.1007/s10096-003-0962-y12884060 [Google Scholar] [CrossRef] [PubMed]
[2]. Takarada H, Sekine M, Kosugi H, Matsuo Y, Fujisawa T, Omata S, Complete genome sequence of the soil actinomycete Kocuria rhizophilaJ Bacteriol 2008 190(12):4139-46.10.1128/JB.01853-0718408034 [Google Scholar] [CrossRef] [PubMed]
[3]. Tewari R, Dudeja M, Das AK, Nandy S, Kocuria kristinae in catheter associated urinary tract infection: a case reportJ Clin Diagn Res 2013 7(8):169210.7860/JCDR/2013/6077.324724086877 [Google Scholar] [CrossRef] [PubMed]
[4]. Styková E, Nemcová R, Gancariková S, Valocký I, Lauková A, Bovine vaginal strain Kocuria kristinae and its characterizationFolia Microbiol 2016 61(3):243-48.10.1007/s12223-015-0431-x26494240 [Google Scholar] [CrossRef] [PubMed]
[5]. Basaglia G, Carretto E, Barbarini D, Moras L, Scalone S, Marone P, Catheter-related bacteraemia due to Kocuria kristinae in a patient with ovarian cancerJ. Clin. Microbiol 2002 40(1):311-13.10.1128/JCM.40.1.311-313.200211773142 [Google Scholar] [CrossRef] [PubMed]
[6]. Lai CC, Wang JY, Lin SH, Tan CK, Wang CY, Liao CH, Catheter-related bacteraemia and infective endocarditis caused by Kocuria speciesClin Microbiol Infect 2011 17:190-92.10.1111/j.1469-0691.2010.03211.x20218989 [Google Scholar] [CrossRef] [PubMed]
[7]. Kandi V, Palange P, Vaish R, Bhatti AB, Kale V, Kandi MR, Emerging bacterial infection: identification and clinical significance of Kocuria speciesCureus 2016 8(8):e73110.7759/cureus.731 [Google Scholar] [CrossRef]
[8]. Ma ES, Wong CL, Lai KT, Chan EC, Yam WC, Kocuria kristinae infection associated with acute cholecystitisBMC Infec Dis 2005 5:6010.1186/1471-2334-5-6016029488 [Google Scholar] [CrossRef] [PubMed]
[9]. Manzoor MA, Mujeeburahiman M, Rekha PD, Association of serum biochemical panel with mineralogical composition of kidney stone in IndiaActa Med Int 2017 4:26-30.10.4103/ami.ami_24_17 [Google Scholar] [CrossRef]
[10]. Manzoor MAP, Mujeeburahiman M, Rekha PD, Electron probe micro-analysis reveals the complexity of mineral deposition mechanisms in urinary stonesUrolithiasis 2018 doi: 10.1007/s00240-018-1052-z. https://doi.org/10.1007/s00240-018-1052-z10.1007/s00240-018-1052-z29504067 [Google Scholar] [CrossRef] [PubMed]
[11]. Shabeena KS, Bhargava R, Manzoor MAP, Mujeeburahiman M, Characteristics of bacterial colonization after indwelling double-J ureteral stents for different time durationUrol Ann 2018 10:71-75.10.4103/UA.UA_158_1729416279 [Google Scholar] [CrossRef] [PubMed]