Conservative Medical Treatment of Emphysematous Gastritis
Lamine Hamzaoui1, Mouna Medhioub2, Amal Khsiba3, Selim Sassi4, Mohamed Msadak Azouz5
1 Associate Professor, Department of Gastroenterology, Faculty of Medicine of Tunis, Mohamed Taher Maamouri Hospital, Tunis El Manar University, Nabeul, Tunisia.
2 Assistant, Department of Gastroenterology, Faculty of Medicine of Tunis, Mohamed Taher Maamouri Hospital, Tunis El Manar University, Nabeul, Tunisia.
3 Assistant, Department of Gastroenterology, Faculty of Medicine of Tunis, Mohamed Taher Maamouri Hospital, Tunis El Manar University, Nabeul, Tunisia.
4 Assistant, Department of Gastroenterology, Faculty of Medicine of Tunis, Mohamed Taher Maamouri Hospital, Tunis El Manar University, Nabeul, Tunisia.
5 Professor, Department of Gastroenterology, Mohamed Taher Maamouri Hospital, Tunis El Manar University, Nabeul, Tunisia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lamine Hamzaoui, Mohamed Taher Maamouri Hospital, Route d’Hammamet, Mrezga-8000, Nabeul, Tunisia.
E-mail: lamine015@yahoo.fr
Emphysematous gastritis is a very rare disease characterised by the presence of air within the stomach wall with an unfavourable prognosis. Diagnosis is generally made by radiologic findings with CT scan as the procedure of choice. We report a case of emphysematous gastritis in an 81-year-old diabetic man with stenosis of celiac trunk and mesenteric artery. We noted a clinico-biological, radiological and endoscopic improvement with conservative treatment despite the presence of stomach necrosis. Early diagnosis with conservative treatment is essential for the successful management of emphysematous gastritis.
Endoscopy, Gastroenterology, Infection
Case Report
An 81-year-old patient, with a history of type 2 diabetes, dyslipidaemia, hypertension, chronic obstructive bronchopneumopathy, and surgical history of umbilical hernia, presented with acute abdominal pain and vomiting which started 48 hours prior to admission. Physical examination showed a temperature of 99.5°F a distended abdomen with intense pain upon pressure in the epigastrum. Blood tests showed leukocytosis (26.103/L) and elevated C-reactive protein (322 mg/L). Abdominal ultrasound was normal.
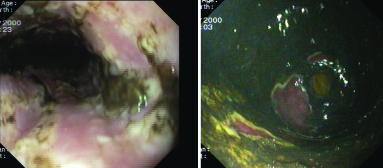
Upper gastrointestinal endoscopy showed ulcerated and necrotic lesions of oesophagus [Table/Fig-1a], the stomach [Table/Fig-1b] and the superior duodenum. A CT scan of the abdomen revealed signs of emphysema in the wall of the stomach with a significant stenosis of the celiac trunk and superior mesenteric artery [Table/Fig-2].
Oesophagogastroduodenoscopy: a) necrotic lesions of oesophagus; b) inflamed and necrotic lesions of the stomach.
A contrast computed axial tomography scan revealing gas in the wall of the stomach (arrows).

A conservative medical treatment was prescribed (antibiotics including cefotaxime, gentamycin and metronidazole in association to heparin relayed by Vitamin-K antagonists). Resolution of symptoms was observed after 3 days. Biological inflammation markers decreased.
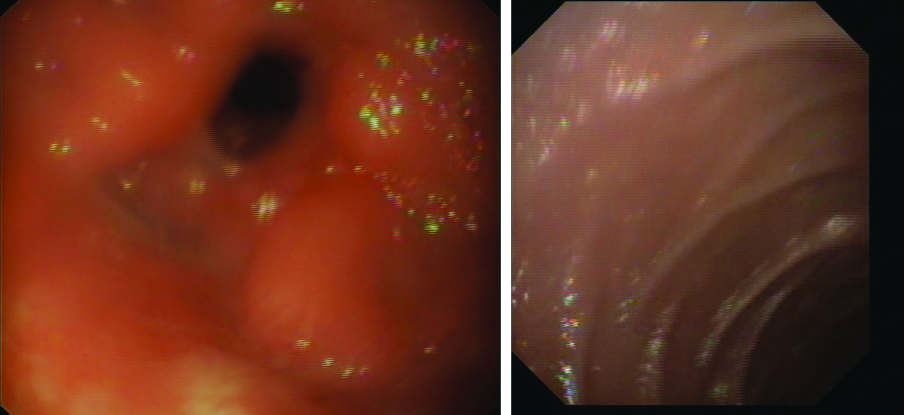
CT scan of the abdomen (day 10) showed a total regression of the gastric pneumatosis [Table/Fig-3]. Upper gastrointestinal endoscopy (day 15) revealed a normal oesophagus mucosa, a congested gastric mucosa without necrotic lesions [Table/Fig-4a] and a normal mucosa of duodenal bulb [Table/Fig-4b]. The patient was asymptomatic 45 days after hospitalisation. He died 3 months later from myocardial infarction.
A contrast computed axial tomography scan showing regression of gastric pneumatosis.

Oesophagogastroduodenoscopy realised at day 15 (after treatment): a) a mild gastric mucosal congestion (antrum) without ulcerations or necrosis; b) normal mucosa of the duodenal bulb.
Discussion
Emphysematous Gastritis (EG) is a very rare lethal infection of the gastric wall caused by gas-producing organisms [1]. Approximately, only 70 cases have been reported in the English literature to date [2]. Several predisposing factors have been reported such as ingestion of corrosives (ammonia, acids, bases), alcohol abuse, recent abdominal surgery, gastric infarction, nonsteroidal anti-inflammatory agents, diabetes, renal failure, gastroenteritis, pancreatitis, treatment with corticosteroids and cytotoxins [2,3]. Pharmaceuticals and ischaemia damage the gastric mucosal barrier [2]. Clinical presentation of EG is usually non-specific and variable, including acute abdominal pain, fever, nausea and vomiting with or without haematemesis and/or melena [4].
The diagnosis of EG is made by the radiological demonstration of intramural gas with CT scan being the imaging study of choice [5]. The diagnosis can be based on these criteria: severe clinical symptoms (abdominal pain, fever, vomiting), elevation in the inflammatory response on blood tests, imaging findings of air within the stomach wall, evidence of bacterial infection, based on gastric juice culture or pathology specimens [2].
Early diagnosis and treatment of EG is important for survival. Conservative treatment, including haemodynamic stabilisation with intravenous fluids, bowel rest, nutritional management and broad-spectrum antibiotics, had showed successful results [6,7]. Surgical treatment (total gastrectomy or partial gastrectomy) is considered in case of complications like perforation, necrosis, peritonitis or signs of strictures after healing [2,6]. In the present case, conservative treatment with close observation was indicated despite the presence of necrosis in oesophagus and stomach because of age, medical history and surgical mortality and morbidity. The prognosis is unfavourable with a mortality rate from 61-100% [8].
Conclusion
Emphysematous gastritis is a rare condition with an unfavourable prognosis. Early diagnosis with conservative treatment was essential for the successful management of the patient.
[1]. Kussin SZ, Henry C, Navarro C, Clain DJ, Gas within the wall of the stomach: report of a case and review of the literatureDig Dis Sci 1982 27:949-54.10.1007/BF013165827117080 [Google Scholar] [CrossRef] [PubMed]
[2]. Nemakayala DR, Rai MP, Rayamajhi S, Jafri SM, Role of conservative management in emphysematous gastritisBMJ Case Rep 2018 doi:10.1136/bcr-2017-222118. In Press10.1136/bcr-2017-22211829477992 [Google Scholar] [CrossRef] [PubMed]
[3]. Al-Jundi W, Shebl A, Emphysematous gastritis: case report and literature reviewInt J Surg 2008 6(6):e63-66.10.1016/j.ijsu.2007.02.00717446149 [Google Scholar] [CrossRef] [PubMed]
[4]. Paul M, John S, Menon MC, Golewale NH, Weiss SL, Murthy UK, Successful medical management of emphysematous gastritis with concomitant portal venous air: a case reportJ Med Case Rep 2010 19(4):14010.1186/1752-1947-4-14020482823 [Google Scholar] [CrossRef] [PubMed]
[5]. Yalamanchili M, Cady W, Emphysematous gastritis in a hemodialysis patientSouth Med J 2003 96:84-88.10.1097/01.SMJ.0000048085.35271.7512602725 [Google Scholar] [CrossRef] [PubMed]
[6]. Bashour CA, Popovich MJ, Irefin SA, Esfandiari S, Ratliff NB, Hoffman WD, Emphysematous gastritisSurgery 1998 123(6):716-18.10.1016/S0039-6060(98)70211-9 [Google Scholar] [CrossRef]
[7]. Szuchmacher M, Bedford T, Sukharamwala P, Nukala M, Parikh N, Devito P, Is surgical intervention avoidable in cases of emphysematous gastritis? A case presentation and literature reviewInt J Surg Case Rep 2013 4(5):456-59.10.1016/j.ijscr.2012.12.02123537915 [Google Scholar] [CrossRef] [PubMed]
[8]. Pear BL, Pneumatosis intestinalis: a reviewRadiology 1998 207:13-19.10.1148/radiology.207.1.95302949530294 [Google Scholar] [CrossRef] [PubMed]