Management of an Electrocuted Burn Injury in a District Hospital-A Case Report and Literature Review
Khoo Kah Seng1, Leong Qi Wen2, Bustaman Syamimi3, Ho Choon Aik4, Lim Chen Hong5
1 Medical Officer, Department of General Surgery, Hospital Segamat, Johor, Malaysia.
2 Medical Officer, Department of General Surgery, Hospital Segamat, Johor, Malaysia.
3 Medical Officer, Department of General Surgery, Hospital Segamat, Johor, Malaysia.
4 General Surgeon, Department of General Surgery, Sultanah Aminah Hospital, Johor Bahru, Johor, Malaysia.
5 General Surgeon, Department of General Surgery, Hospital Segamat, Johor, Malaysia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Khoo Kah Seng, KM-6, Jalan Genuang-85000, Segamat, Johor, Malaysia.
E-mail: kahseng901209@gmail.com
Electrical burns are one of the important health burdens throughout the world with incidences varying between 4-18% of all burns. They comprise of several types, including lighting injury, high voltage injury (>1000V) and low voltage injury (<1000V). The severity of injury depends on the type and strength of current, current pathway and duration of contact. Injuries sustained from high voltage electrical current can result in cardiac arrest and death, while the other survivors may have extensive damage to soft tissues and bones along with muscle necrosis and rhabdomyolysis. Hereby, we present a case of 45-year-old man whom sustained a high voltage electrical injury (railway voltage) with 25% Total Body Surface Area (TBSA) of mixed partial burns over the path of current. He was managed primarily by general surgical team in a district hospital. In this article, we discuss about management of electrocuted burns in district hospital setting without burn unit. A prompt resuscitation and monitoring of potential complications secondary to electrical burns are vital to reduce morbidity and mortality.
High voltage, Rhabdomyolysis, Total body surface area
Case Report
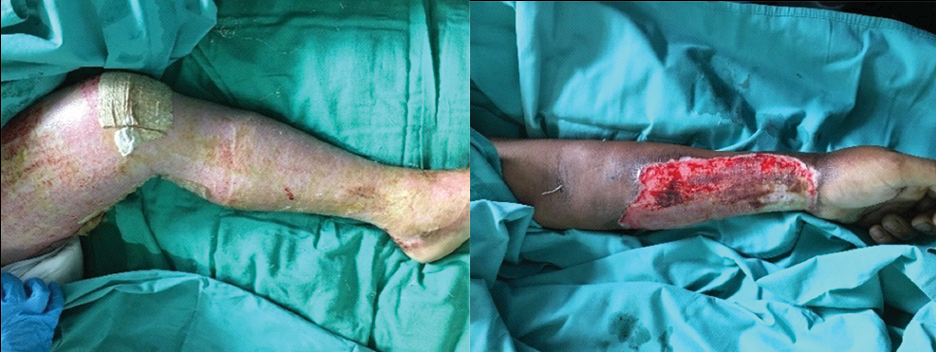
A 45-year-old man was accidentally electrocuted when he came in contact with the overhead line in subway station. He worked as a cleaner in a railway station during the incident. He was subsequently thrown to the ground by the impact. He was brought to the emergency department. On arrival to emergency department, he was tachycardic and tachypnoeic with respiratory rate of 32 breaths per minute with no evidence of airway compromise. There were no signs of inhalation injury. His Glasgow Coma Score was 15 out of 15. He was subsequently intubated for airway protection and then admitted to Intensive Care Unit (ICU) for close monitoring and fluids resuscitation according to Parkland’s formula. On inspection, there were mixed partial thickness burns over his anterior trunk, left anterior aspect of forearm, left anterior aspect of lower limb and right anterior aspect of thigh (which constitutes of 25% of TBSA) [Table/Fig-1,2]. His left forearm compartment was tense, however with good perfusion and all distal pulses were intact, therefore no fasciotomy was performed. Local debridement was performed as early as the second day and he was dressed with normal saline. The first Electrocardiogram (ECG) showed sinus rhythm with right bundle branch block without any pathological change and he was put on continuous cardiac monitoring. Biochemical investigations revealed elevated serum Creatinine Kinase (CK) (7094 U/L) which indicates muscle lysis. Otherwise, renal profile and blood gas were within normal limit. Urine output was kept above 1.5 cc/kg/hours since admission.

He was managed with daily normal saline dressing. Subsequently, he was extubated on day three of admission and was transferred out to general ward. Despite that, thick slough was still seen on his wound. Therefore, he underwent wound debridement and dressing under general anaesthesia on day five. On day nine of admission, wound appeared clean with minimal sloughs [Table/Fig-3,4 and 5].
Post wound debridement and dressing (trunk).

Post wound debridement and dressing (upper and lower limb).
Following the days, he was doing well throughout the hospitalisation. His cardiac function remained stable with good urine output and no signs of deterioration. His CK dropped from 7094 U/L to 386 U/L by day 10. His pain was managed with Patient Controlled Analgesia (PCA) opioid and Nonsteroidan Anti-inflamatory Durgs (NSAIDs). Besides that, limb physiotherapy was started to prevent contracture and joint stiffness. He was discharged well on day 23 of post trauma with continuation of daily dressing at home. He was followed up in surgical outpatient department, one month post trauma [Table/Fig-6].

Discussion
Overall, electrical injuries are associated with high morbidity and mortality, with a risk of death as high as 40%. A 20-year review of electrical injuries in adults and children in a large burn unit in Texas by Arnoldo et al., revealed that the mortality rate varied according to the type of electrical exposure: low voltage, 2.8%, high voltage, 5.3%, and lighting strikes, 17.6% [1].
Electrical burns are quite different from injuries sustained due to thermal or chemical burns [2]. Although, primary electrical injury is burns, secondary blunt trauma may result from falls or being thrown from the electrical source by an intense contraction of muscles [2-4]. Electrical injuries can be life-threatening as cardiorespiratory arrest and major cardiac arrhythmias can occur [1-8]. In adults, most electrical injuries happen at the workplace and constitute the fourth leading cause of work-related traumatic death [2,5,7]. As in the presented case, he sustained the electrocuted burns in the railway station during his working hour. Most of the high voltage electrical injuries are accidental. The use of protective devices is essential while working on any electrical cables.
Both entry and exit wounds are seen only in 20% of the cases [5]. In cases of severe burns with high-voltage current, because of thermal damage to tissue entry and exit, wounds may not be evident. In this case report, the entry and exit points were not evident. The treatment of high voltage electrical injuries requires multidisciplinary teams approach. Immediate resuscitation is important so that, cardiorespiratory complications are prevented [1,5]. The maintenance of vital parameters and early wound debridement can prevent systemic complications and physical disabilities.
In patients with electrical burns, since morbidity and mortality rates are high, defining risk factors is important for the prompt management and especially to reveal preventive measures in high-risk patients. In Tiryaki C et al., study, they have evaluated the risk factors for mortality in victims of electrical burns and TBSA >20%; ICU requirement, erythrocyte, Fresh Frozen Plasma (FFP) or albumin transfusion requirements, admission albumin level <3.5 mg/dL and admission haemoglobin level <12 mg/dL were determined as the risk factors for mortality [8]. In this case report, patient fulfilled 2 of the risk factors which are TBSA >20% and ICU admission. He did not receive transfusion during the stay. There are some mechanisms of the hypoalbuminaemia development in burn patients. All types of burns result in hypercatabolic responses that decrease serum albumin levels and also with an increase in TBSA percentage, an extracellular fluid loss induces vascular permeability and a plasma albumin loss from the wound exudations [8]. When developed, hypoalbuminaemia is associated with oedema, disturbances in wound healing and an increased susceptibility to sepsis that may play a role in mortality. On the other hand, anaemia directly reduces the oxygen delivery and worsens the multi-organ failure, especially acute kidney injury if present which may be associated with the increased mortality [8].
It has been a challenge to manage this patient in a district hospital without burn unit and adequate backup. In context of acute management, initial fluids resuscitation is vital to prevent acute renal failure from myoglobinuria. Besides that, close monitoring of cardiac rhythm, renal functions and musculoskeletal complications are needed in electrical burns. Appropriate wound debridement and aseptic technique during dressing is the key to prevent sepsis. On the other hand, nursing staffs in general setting might not familiar with burns management especially in dressing and wound management. With prompt and appropriate resuscitative efforts from multidiscipline team, patients can survived from high voltage current injuries.
Conclusion
In summary, the initial management of electrocuted burns could be done according to Advanced Trauma Life Support (ATLS) protocol in district setting as a guideline. However, special attention on fluids resuscitation, close monitoring of cardiac disturbance and musculoskeletal complications are emphasised. Prevention is definitely better than treatment. Thus, special precautions and protective devices should be introduced to the at risk workers.
[1]. Arnoldo BD, Purdue GF, Kowalske K, Helm PA, Burris A, Hunt JL, Electrical injuries: a 20 year reviewJ Burn Care Rehabil 2004 25(6):479-84.10.1097/01.BCR.0000144536.22284.5C15534455 [Google Scholar] [CrossRef] [PubMed]
[2]. Saeed AC, Pattern and profile of electric burn injury cases at a burn centreJournal Ayub Med Coll Abbottabad 2016 28(4):702-05. [Google Scholar]
[3]. Ungureanu M, Electrocutions-treatment strategy (case presentation)Journal of Medicine and Life 2014 7(4):623-26. [Google Scholar]
[4]. Zbuchea A, Humeral neck fracture after electrocution- case report and literature reviewChirurgia 2015 110(5):490-92. [Google Scholar]
[5]. Kumar SS, Narayan AR, Gopal S, Kumar JG, Agrawal A, High voltage electrical shock with multiple life-threatening injuriesInt J Crit Illness Inj Sci 2015 5(4):266-68.10.4103/2229-5151.17084726807397 [Google Scholar] [CrossRef] [PubMed]
[6]. Kokatnur L, Rudrappa M, Acute stroke due to electrocution: uncommon or unrecognized?Case Reports in Neurological Medicine 2016 9510863:01-05.10.1155/2016/951086328058122 [Google Scholar] [CrossRef] [PubMed]
[7]. Ngim NE, Otei OO, Osakwe O, Limb gangrene following high tension electrical injury: The need for caution!Internet Journal of Third World Medicine 2013 11(1):01-04. [Google Scholar]
[8]. Tiryaki C, Haksal MC, Yazicioglu MB, Ciftci A, Esen O, Turgut HT, Factors affecting mortality among victims of electrical burnsUlus Travma Acil Cerrahi Derg 2017 23(3):223-29.10.5505/tjtes.2016.2916628530776 [Google Scholar] [CrossRef] [PubMed]