Melanoacanthoma of Pinna-Treated with Skin Grafting: A Case Report
Santosh Uttarkar Pandurangarao1, Sridurga Janarthanan2, Aravind Darga Ramachandra3
1 Professor, Department of Ear, Nose and Throat, JJM Medical College, Davangere, Karnataka, India.
2 Postgraduate Student, Department of Ear, Nose and Throat, JJM Medical College, Davangere, Karnataka, India.
3 Postgraduate Student, Department of Ear, Nose and Throat, JJM Medical College, Davangere, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Santosh Uttarkar Pandurangarao, Professor, Department of Ear, Nose and Throat, JJM Medical College, Davangere-577004, Karnataka, India.
E-mail: drsantoshup@gmail.com
Melanoacanthoma is a very rare cutaneous lesion and it is considered to be a benign neoplasm, which is composed of large dendritic melanocytes and epidermal keratinocytes. Very few case reports of melanoacanthoma have been described in Indian literature in recent past. We hereby report a case of melanoacanthoma in a 50-year-old male, who presented to us with a growth in right ear, since 30 years. On examination of right pinna, a 4×3 cm blackish irregular mass occupying the conchal region, encroaching towards the external auditory canal. Surgical excision of the growth was done, since the patient had cosmetic problem and for biopsy (to differentiate it from melanoma and to confirm the diagnosis). As the lesion was big so, to close the primary defect, split skin grafting was used as one of the treatment.
Cartilage, Concha, Keratinocyte, Malignant melanoma, Melanocyte, Split skin graft
Case Report
A 50-year-old, male patient reported to the Department of Otorhinolaryngology, with the complaints of growth in right ear since 30 years. It started with a pigmented elevated lesion at the same site, which gradually increased to the present size. The patient did not have any other medical history/comorbidities.
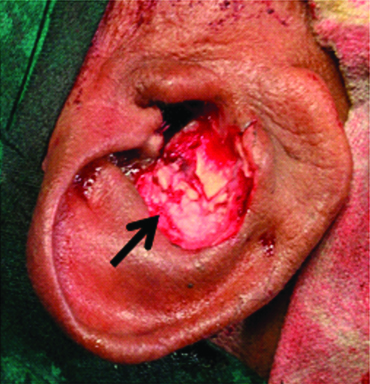
On examination of right pinna, a blackish irregular mass of 4×3 cm, occupying the conchal region, which was firm in consistency, encroaching towards the external auditory canal, not sensitive to touch and did not bleed on touch was present [Table/Fig-1]. External auditory canal and tympanic membrane of right side could not be visualised. Left ear was normal on examination. No abnormality was detected on systemic examination.
Pigmented, prolierative growth in right pinna.

After clinical examination, a differential diagnosis of melanoma and melanoacanthoma were thought of. An excision biopsy with or without split skin grafting was planned for the patient.
Preoperative work-up was done. All reports were within normal limit. After explaining the need for surgery to the patient, informed and written consent was taken for surgery.
Under general anaesthesia, the affected part was painted with betadine solution and drapped. A curvilinear incision was taken along the antihelix. Dissection was done and the growth was found to be infiltrating the conchal cartilage. Mass with approximately 1 mm of normal skin was excised [Table/Fig-2]. Complete haemostasis and asepsis was maintained in the surgical field. Excised mass sent for histopathological examination.
Right pinna, after excision of mass.
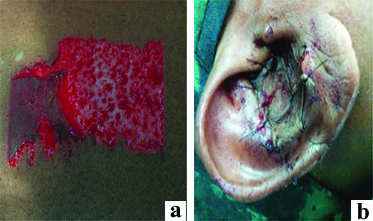
Since the skin defect was larger, primary closure was not done. A split skin graft was harvested from right thigh [Table/Fig-3a]. And the skin defect was closed by split skin graft [Table/Fig-3b]. Mastoid dressing and donor site dressing was done.
a) Split skin graft taken from right thigh; b) Split skin graft sutured to recipient site.
Regular postoperative care was given. Suture removal was done on 7th postoperative day. The recipient site was inspected on 7th day, after 3 weeks and 3 months. The recipient site has completely healed [Table/Fig-4].
Postoperative picture after 3 weeks.

Gross report of histopathology, showed a grey brown to grey black soft tissue mass measuring 4×3×1 cm. External surface was grey brown to grey black and cut surface was grey black in colour [Table/Fig-5a,b].
a) Gross specimen anterior view; b) Gross specimen posterior view.

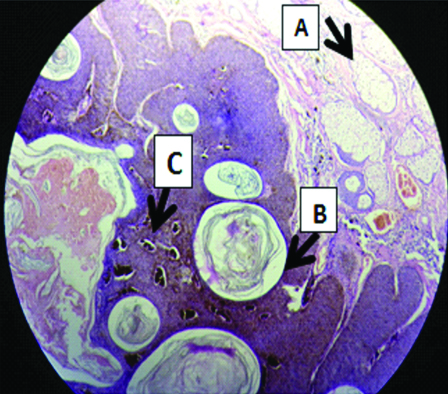
Microscopic section (under 10X magnification) showed greatly thickened epidermis composed of basaloid cells, marked melanin pigmentation, horn cyst (true and pseudo). The thick interwoven tract of epithelium is surrounded by connective tissue. The melanocytes are distributed throughout the tumour. The lesion was resting on a cartilage island [Table/Fig-6].
Histopathology (H&E staining) under 10X magnification showing: (a) Apocrine glands; (b) Horn cyst; (c) Dispersed melanin pigments.
Discussion
Melanoacanthoma is a benign, deeply pigmented, proliferation of keratinocytes and melanocytes. It is a very rare variant of seborrheic keratosis [1]. Mishima Y and Pinkus H in 1960 coined the term melanoacanthoma [2]. Bloch in 1927 described it as nevoid epithelioma type 1, which is different from the melanoepithelioma Type 2 or the ordinary pigmented variant of seborrheic keratosis [3]. It is more commonly seen in light skinned and presents as pigmented papules, plaques, cutaneous horns or nodules [4]. Patients are commonly asymptomatic and usually wait for several years before taking any treatment. Melanoacanthoma most commonly arises as a single lesion in the region of head, neck, trunk, lip and eyelid.
Melanoacanthoma shows proliferation of melanocytes and keratinocytes, confined only to the epidermis. Melanocytes are present deep into the tumour mass, by breaching the basal layer. This histological feature differentiates it from pigmented variant of seborrheic keratosis [5].
There are two histological types of melanoacanthoma, one is diffuse type, in which melanocytes are dispersed throughout the lesion and other is clonal type, where melanocytes and keratinocytes are grouped in small nests [4]. Electron microscopic studies have revealed that there is a defect in the transfer of the melanin from these highly dendritic melanocytes to the keratinocytes. Melanoacanthoma are not related to malignant melanoma, as per immunofluoroscent and immunoprecipitin studies. Cryotherapy or simple excision is a curative treatment [6].
There are very few case reports of melanoacanthoma arising from pinna Naik K et al., and Mudra RK et al., reported a case of seborrheic keratosis, of 3×2 cm in right pinna, which was excised and primary suturing was done [7,8]. However, in present case, as the lesion was big, to close the primary defect, split skin grafting was used as one of the treatment.
Patnayak R et al., in their case report presented two cases of melanoacanthoma. The first and second case in their study, presented with a pigmented lesion on the external auditory canal of dimensions 1.5×1 cm and 1×1 cm respectively. Clinically, they suspected melanoma. But, after excision the histopathology report showed characteristic features of melanoacanthoma [9].
Conclusion
Melanoacanthoma is a rare condition and it can occur in unusual sites like pinna. It should not be confused with melanoma. Histopathology of the excised lesion helps us to differentiate it from melanoma. After excision, where primary closure cannot be done, due to large skin defect, a split skin grafting can be done.
[1]. Thomas VD, Swanson NA, Lee KK, Benign epithelial tumours, hamartomas, and hyperplasias. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editorsFitzpatrick’s Dermatology in General Medicine 2008 7th edNew YorkMc-Graw Hill:1054-67. [Google Scholar]
[2]. Mishima Y, Pinkus H, Benign mixed tumour of melanocytes and malpighian cells. Melanoacanthoma: its relationship to Bloch’s benign on nevoid melanoepitheliomaArch Dermatol 1960 81:539-50.10.1001/archderm.1960.0373004004300914422903 [Google Scholar] [CrossRef] [PubMed]
[3]. MacKie RM, Quin AG, Non melanoma skin cancer and other epidermal skin tumours. In: Burns T, Breathnach S, Cox N, Griffiths C, editors 2004 7th edOxfordBlackwell:361-50. [Google Scholar]
[4]. Schwartz RA, Kihiczak GG, Cutaneous melanoacanthomaAvailable from: http:\\www.emedicine.com/derm/authorid2848, topicid865. [Last Accessed on 2006 Jun 27] [Google Scholar]
[5]. Vasani RJ, Khatu SS, Melanoacanthoma: uncommon presentation of an uncommon conditionIndian Dermatol Online J 2013 4:119-21.10.4103/2229-5178.11063823741670 [Google Scholar] [CrossRef] [PubMed]
[6]. Schlappner OL, Rowden G, Philips TM, Rahim Z, Melanoacanthoma. Ultrastructural and immunological studiesJ Cutan Pathol 1978 5:127-41.10.1111/j.1600-0560.1978.tb00949.x210197 [Google Scholar] [CrossRef] [PubMed]
[7]. Naik K, Adersh S, Mathew NL, A rare case of large seborrheic keratosis of the pinnaCIB Tech Journal of Surgery 2014 3:09-10. [Google Scholar]
[8]. Mundra RK, Agrawal R, Sinha R, A rare interesting case of seborrheic keratosis of pinnaCase Reports in Clinical Medicine 2013 2:463-65.10.4236/crcm.2013.28122 [Google Scholar] [CrossRef]
[9]. Patnayak R, Jena A, Chowhan AK, Rukmangadha N, Reddy MK, Melanoacanthoma of external ear: report of two casesJ Lab Physicians 2013 5:63-64.10.4103/0974-2727.11592824014974 [Google Scholar] [CrossRef] [PubMed]