Unearthing an Unusual Presentation of Chondrosarcoma Rib as Breast Mass: A Diagnostic Dilemma
Vijeta Tomar1, Parul Dargar2, Neha Vijay3, Paras Nuwal4
1 Senior Demonstrator, Department of Pathology, Sawai Man Singh Medical College, Jaipur, Rajasthan, India.
2 Assistant Professor, Department of Pathology, Index Medical College, Indore, Madhya Pradesh, India.
3 Senior Demonstrator, Department of Pathology, Jawaharlal Nehru Medical College, Ajmer, Rajasthan, India.
4 Ex Head and Senior Professor, Department of Pathology, Jawaharlal Nehru Medical College, Ajmer, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vijeta Tomar, D-166, Lane no. 7, Nirman Nagar, Jaipur-305001, Rajasthan, India.
E-mail: dr.vijetatomar@gmail.com
Chondrosarcomas usually arise in the pelvis or bones of the trunk, but rarely primary chest wall (rib) chondrosarcomas are also noted. We report the case of an 18-year-old female, who presented with left breast mass. On mammography and Ultrasonography (USG), possibility of giant fibroadenoma with cystic changes was given. On Fine Needle Aspiration Cytology (FNAC) and trucut biopsy of the mass, a diagnosis of pleomorphic adenoma was given. However, during resection it was found to be arising from left 4th rib, breast parenchyma was uninvolved and pushed to a side by the mass. Grossly, the mass was capsulated, lobulated and grey white measuring 17×13×10 cm. On cutting, it had a glistening bluish grey colour. On histology, a diagnosis of chondrosarcoma was given.
Case Report
An 18-year-old female complained of progressive left breast enlargement since six months. On examination, the left breast was markedly enlarged in comparison to right breast. The swelling was nodular, firm, fixed and non tender measuring 17x13x10 cm. Overlying skin, nipple and areola were unremarkable. Patient had no axillary lymphadenopathy. USG and mammography showed a well defined mass in left breast with cystic change, and a possibility of giant fibroadenoma was given. X-ray and Computed Tomography (CT) were not advised in view of age, clinical presentation and a possible diagnosis of giant fibroadenoma on mammography and USG was given.
FNAC was performed from left breast mass. Mucoid gelatinous substance was obtained on multiple passes. Cytological smears from the swelling were stained with haematoxylin and eosin stain. Smears were fairly cellular showing chondrocytes against chondromyxoid stroma. The cells were with well defined cytoplasm, round to oval nuclei, one to two small nucleoli and mild to moderate pleomorphism. Occasional binucleate cells were also noted. Mitosis was not seen [Table/Fig-1a,b]. In view of the age, site, clinical presentation, USG and mammographic findings and chondromyxoid substance on aspiration, a possibility of pleomorphic adenoma was given on cytology. On trucut biopsy, a tiny tissue measuring 0.2×0.2 cm was received which showed increased chodrocytes and chondroid matrix. Hence, in view of previous findings and FNAC report, again a possibility of pleomorphic adenoma was given.
Cytological smears: a) Chondrocytes lying in chondromyxoid substance (H&E, 10X); b) Chondrocytes with moderate pleomorphism, binucleate cells also seen (H&E, 40X); Gross. c) Encapsulated tumour with simple mastectomy; d) Rib can be seen (pointed by forceps).
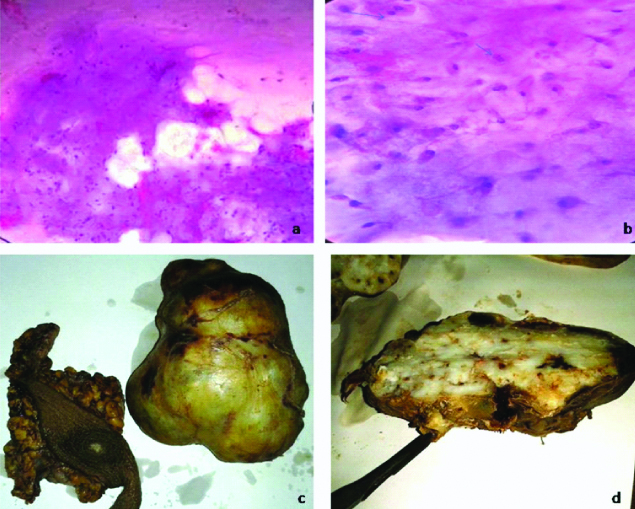
Patient was taken up for surgery, during excision the mass was seen to be arising from 4th rib. It was capsulated, nodular pushing the breast parenchyma to a side. However, nipple and areola were in place giving a pseudo appearance of mass arising from breast. The mass was excised along with part of 4th rib. Left side mastectomy was also performed. We had received tumour mass with part of rib and left mastectomy in the same jar. Grossly, the tumour was globular, grey white, encapsulated, well circumscribed, lobulated with nodular surface measuring 17×13×10 cm. Part of rib was attached to a side of mass measuring 1 cm in length. On cutting, the tumour was grey white with bluish glistening solid and cystic areas. Cystic spaces were filled with mucoid substance. At places gritty sensation were felt during cutting [Table/Fig-1c,d]. The breast, nipple and areola were unremarkable.
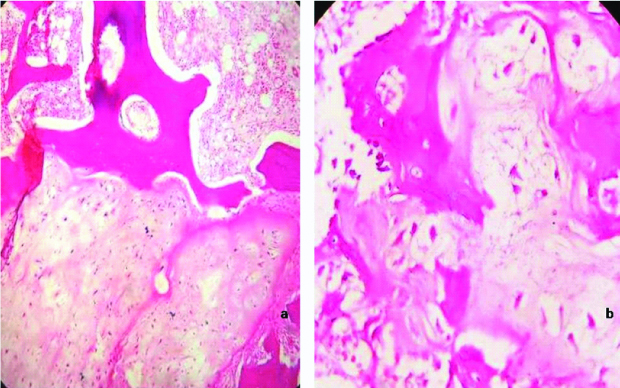
Sections were stained with haematoxylin and eosin and showed tumour cells lying in cartilaginous matrix having plump, hyperchromatic nuclei and moderate pleomorphism. At places binucleation and multinucleation were noted [Table/Fig-2a,b]. The tumour cells were permeating the marrow at places. The bone cut margin, breast parenchyma, nipple and areola were free of tumour. Based on the histomorphological features, a final diagnosis of well differentiated chondrosarcoma was given. However, a possibility of chondrogenic osteosarcoma was asked to rule out.
Histological sections: a) Marrow spaces are infiltrated by malignant chondrocytes (H&E, 10X); b) Malignant cells invading bone (H&E, 40X).
Discussion
Chondrosarcomas are the third most common malignant bone neoplasm and tends to involve the larger bones or pelvis of adult patients. There is a definite male predilection, and generally occurs in adult patients (30-60 years). Chondrosarcoma is unusual in patients younger than 16 years of age [1]. It is rare for chondrosarcoma to arise in the ribs [2,3]. However, in this case, patient was 18-year-old and was a female.
Mayo group reported 10 years survival rate of 96.4% for those who had wide resection, compared with 65.4% for those who had local excision only. McAfee MK et al., reported one of the largest studies of chest wall chondrosarcomas in 1985. The study consisted of 96 patients with primary chondrosarcoma of the chest wall with a median age of 53.5 years [4].
Microscopically, chondromyxoid ground substance is usually abundant in low grade tumours. Cellularity is variable in low grade chondrosarcoma. This is important in the distinction from chordoma. The tumour cells have a well defined cytoplasm and round nuclei with one or two nucleoli. Binucleate cells are present and nuclear pleomorphism is of moderate degree. Single cells dominate in high grade malignant tumours, cellular and nuclear pleomorphism is prominent and mitoses are present. Often abundant myxoid background matrix is present, while fragments of hyaline cartilage are few. It is difficult or impossible to distinguish between chondroma and some low grade (Grade 1) chondrosarcomas in fine needle biopsy smears [5].
The whole tumour was excised en masse along with 4th rib and simple mastectomy. Patient had an uneventful recovery and being followed up for one year.
Conclusion
To conclude, the unusual clinical presentation and subtle symptoms may masquerade a malignant lesion. Thus, a more extensive radiological work up should be considered in such patients.
[1]. Sternberg S, Stacey E, Mills Darryl Carter, Bone tumours. In: Stacy E, editorSternberg’s Diagnostic Surgical Pathology 2009 5th edChinaWolter Kluver:248-253. [Google Scholar]
[2]. King RM, Pairolero PC, Trastek VF, Piehler JM, Payne WS, Bernatz PE, Primary chest wall tumours: factors affecting survivalAnn Thorac Surg 1986 41:597-601.10.1016/S0003-4975(10)63067-6 [Google Scholar] [CrossRef]
[3]. Sabanathan S, Shah R, Mearns AJ, Surgical treatment of primary malignant chest wall tumoursEur J Cardiothorac Surg 1997 11:1011-16.10.1016/S1010-7940(97)00090-0 [Google Scholar] [CrossRef]
[4]. McAfee MK, Pairolero PC, Bergstralh EJ, Piehler JM, Unni KK, McLeod RA, Chondrosarcoma of the chest wall: factors affecting survivalAnn Thorac Surg 1985 40:535-41.10.1016/S0003-4975(10)60344-X [Google Scholar] [CrossRef]
[5]. Orell SR, Sterrett GF, Whitaker D, Bone. In: Orell, editorFine Needle Aspiration Cytology 2005 5th editionNew DelhiElsevier:422-23. [Google Scholar]