Spontaneous Inguinal Faecal Fistula due to Incarcerated Richter’s Hernia-Managed Conservatively
Ranendra Hajong1, Malaya Ranjan Dhal2, Narang Naku3, Manash Pratim Boruah4, Ojing Komut5
1 Associate Professor, Department of General Surgery, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
2 Resident, Department of General Surgery, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
3 Resident, Department of General Surgery, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
4 Resident, Department of General Surgery, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
5 Assistant Professor, Department of General Surgery, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ranendra Hajong, Associate Professor, Department of General Surgery, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong-793012, Meghalaya, India.
E-mail: ranenhajong@gmail.com
Spontaneous enterocutaneous fistula due to strangulated inguinal Richter’s hernia is a rare presentation and occurs mostly either due to ignorance of the patients or delay in seeking timely medical intervention. It is seen mostly in patients from developing countries like India, Nigeria, etc., Reported here is the case of a 50-year-old female patient who presented with left sided fecal fistula which on investigation was found to be due to incarcerated inguinal Richter’s hernia. The patient refused for any surgical intervention and hence was managed successfully and conservatively. No similar case reports have been found in the literature thus highlighting its significance.
Enterocutaneous fistula, Inguinal hernia, Spontaneous origin
Case Report
A 50-year-old female patient was admitted with the complaint of passage of faecal material from the left inguinal region since one week. The discharge was copious in amount. On detailed enquiry, the patient gave history of a painful swelling in the same region which started discharging yellow coloured fluid after about four days of appearance of the swelling. The patient did not give any history of vomiting or constipation or abdominal distension since the beginning of the complaints.
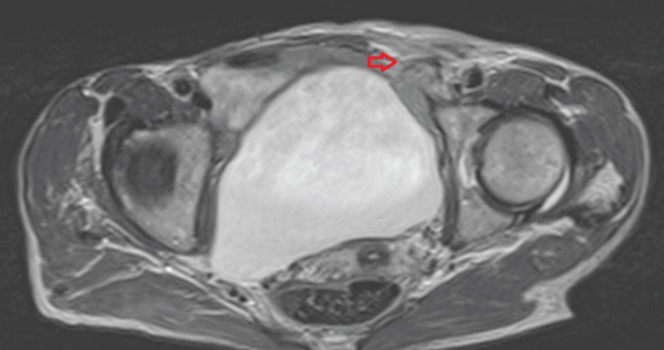
Clinically, a diagnosis of enterocutaneous fistula due to incarcerated inguinal hernia was made in view of the history of a painful swelling in the inguinal region prior to the starting of the discharge [Table/Fig-1]. The patient did not have any features of sepsis and all the blood investigations were within normal limits. MRI (Magnetic Resonance Imaging) was done to confirm the diagnosis which showed features of left sided direct inguinal hernia [Table/Fig-2] with intact femoral canal. The patient did not opt for any surgical intervention. So, she was planned for conservative management after explaining the needs for emergency laparotomy should her condition deteriorate.
The discharging inguinal fistula.

MRI showing inguinal hernia.
She was started on broad spectrum antibiotic to prevent sepsis from developing. She was kept nil per orally for few days and started on total parenteral nutrition. She responded well to conservative management and the discharge reduced drastically from second week onwards. She was discharged after about three weeks of hospitalisation. By that time the fistulous opening had closed [Table/Fig-3]. She was followed up till one year and was doing well without any recurrence of herniation clinically or sonologically.
The healed fecal fistula scar.

Discussion
Spontaneous faecal fistula is a very rare complication of strangulated Richter’s hernia. The entrapped circumference of the bowel wall on the anti-mesenteric side may result in ischemia, gangrene and perforation leading to the formation of enterocutaneous fistula [1]. Richter’s hernia occurs most commonly in the femoral ring (72-88%), followed by inguinal canal (12-24%) and the abdominal wall incisional hernias (4-25%) [1].
Luminal continuity is not obstructed in Richter’s hernia as only a part of the circumference of the bowel wall is entrapped in Richter’s hernia resulting in undue delay in diagnosis and increased mortality [2]. The patient in the present case also did not have any features of acute intestinal obstruction in the form of vomiting, constipation or abdominal distention.
Spontaneous enterocutaneous fistula was reported by Kumar A et al., which they tried initially to manage conservatively in a 60-year-old male patient, but on the third post-admission day the patient developed acute intestinal obstruction and had to be operated on where the patient was found to have bilateral femoral hernias with enterocutaneous fistula developing in the left side. Reduction and repair of hernia was done in that patient [3]. Umbilical enterocutaneous fistula due to incarcerated Richter’s hernia was reported by Chen W et al., but had to be operated due to repeated umbilical infections [4]. Elenwo SN reported entero-labial fistula due to incarcerated inguinal Richter’s hernia which had to be managed surgically [5]. The present case may be the first case of spontaneous enterocutaneous fistula developing as a complication of incarcerated inguinal Richter’s hernia which was managed conservatively and successfully. The fistula may however recur if no other further surgical management is undertaken [6].
Reber HA et al., in their series of 186 patients reported that 91% of small bowel enterocutaneous fistulas close spontaneously within one month of sepsis control [7]. Uba FA et al., also found that majority of enterocutaneous fistulas in children close spontaneously with high carbohydrate and protein nutrition [8]. The present case also responded positively to conservative management and there was no hernial recurrence till one year of follow-up.
Conclusion
Richter’s hernia may rarely present with spontaneous enterocutaneous fistula without any features of acute intestinal obstruction and may be managed successfully conservatively with proper sepsis control and maintenance of nutrition.
[1]. Ahi KS, Moudgil A, Aggarwal K, Sharma C, Singh K, A rare case of spontaneous inguinal faecal fistula as a complication of incarcerated Richter’s hernia with brief review of literatureBMC Surg 2015 15:6710.1186/s12893-015-0055-826018618 [Google Scholar] [CrossRef] [PubMed]
[2]. Faridi SH, Siddiqui B, Khan MA, Anees A, Ali SA, Suprapubic faecal fistula due to richter’s inguinal hernia: a case report and review of literatureIran J Med Sci 2013 38(2):129-31. [Google Scholar]
[3]. Kumar A, Pahwa HS, Pandey A, Kumar S, Spontaneous enterocutaneous fistula due to femoral herniaBMJ Case Reports 2012 2012:bcr201200693910.1136/bcr-2012-00693923060376 [Google Scholar] [CrossRef] [PubMed]
[4]. Chen W, Liu L, Huang H, Jiang M, Zhang T, A case report of spontaneous umbilical enterocutaneous fistula resulting from an incarcerated Richter’s hernia, with a brief literature reviewBMC Surgery 2017 17:1510.1186/s12893-017-0216-z28193213 [Google Scholar] [CrossRef] [PubMed]
[5]. Elenwo SN, Igwe PO, Jamabo RS, Sonye US, Spontaneous entero-labial fistula complicating Richters hernia: Report of a caseInt J Surg Case Rep 2016 20:27-29.10.1016/j.ijscr.2016.01.00326785080 [Google Scholar] [CrossRef] [PubMed]
[6]. Weledji EP, Puepi MA, Chichom AM, A rare spontaneous enterocutaneous fistulaJ Surg Case Rep 2014 2014(11):rju12110.1093/jscr/rju12125391523 [Google Scholar] [CrossRef] [PubMed]
[7]. Reber HA, Roberts C, Way LW, Dunphy JE, Management of external gastrointestinal fistulasAnn Surg 1978 188(4):460-67.10.1097/00000658-197810000-00003697430 [Google Scholar] [CrossRef] [PubMed]
[8]. Uba FA, Uba SC, Ojo EO, Management of postoperative enterocutaneous fistulae in children: a decade experience in a single centreAfr J Paediatr Surg 2012 9(1):40-46.10.4103/0189-6725.9330222382103 [Google Scholar] [CrossRef] [PubMed]