Fracture dislocations of Carpometacarpal (CMC) joints are high-energy injuries, often occurring from vehicle accidents. We here by present a rare case of open dislocation of the second, third, and fourth CMC joints associated with comminuted fracture of the first and fourth phalanges. The fracture in radius and ulna was managed by open reduction and fixed with multiple Kirschner wires (K-wires) and plates. The Disabilities of the Arm, Shoulder and Hand (DASH) score was used to assess functional status at the end of physiotherapy, which improved from 74.2 to 0 over two years. Union was achieved at the end of three months, with an eventual good functional outcome and joint alignment. A high index of suspicion along with good clinical examination and careful assessment of radiographs can ensure early diagnosis and proper management of this rare injury.
Case Report
A 48-year-old housewife presented to the emergency department with left wrist pain and dysfunction after sustaining a motor vehicle collision. The patient accidentally fell from the seat of her motorcycle, which she had parked on the street side but it was still running. It dragged her approximately 2 meters before she was able to untangle herself. Clinical examination revealed significant swelling, numbness, and deformity of the left hand and wrist, with an open avulsion wound on the left palm [Table/Fig-1]. Anteroposterior (AP), lateral and oblique radiographs (X-rays) of the left hand and the left forearm, including the wrist, showed multiple open volar dislocation of the second, third, and fourth CMC joints, comminuted fracture of the first, and fourth proximal phalanges [Table/Fig-2,3], and an associated fracture of the radius shaft and the ulnar shaft [Table/Fig-4,5]. The second, third, and fourth metacarpals were reduced onto the carpals under general anesthesia by applying force to the palm and using longitudinal traction as recommended by Schaefer N et al., [1]. Multiple K-wires 1.6 mm in diameter were inserted through the metacarpals, to maintain reduction. Comminuted fractures of the first and fourth proximal phalange were closed; reduction was maintained via K-wire fixation [Table/Fig-6,7]. The associated fracture of the radius and the ulna was managed with plates and screws.
Open dislocation of the 2nd, 3rd, 4th CMC joint of the left hand.

Preoperative anteroposterior radiograph of the left wrist and hand showing displacement and angulation of the metacarpal joint.

Preoperative oblique radiograph of the left wrist and hand showing displacement and angulation of the metacarpal joint.

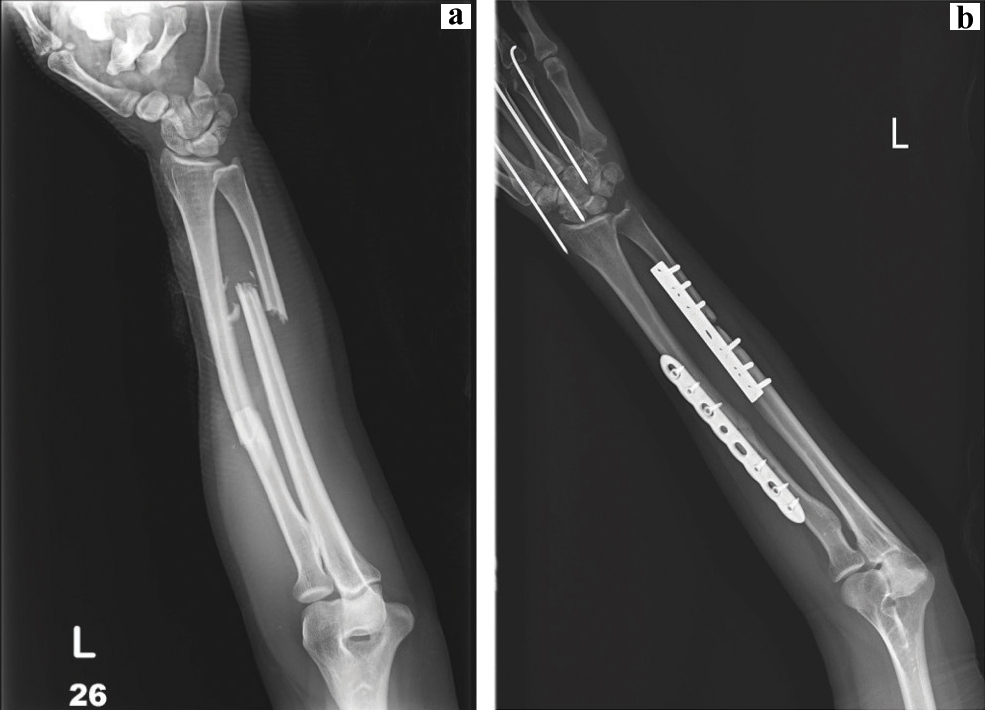
a) Preoperative anteroposterior radiograph of the left forearm showing displacement and angulation of the radius shaft and ulnar shaft; b) Postoperative anteroposterior radiograph of the left forearm showing internal plates with screws fixation.
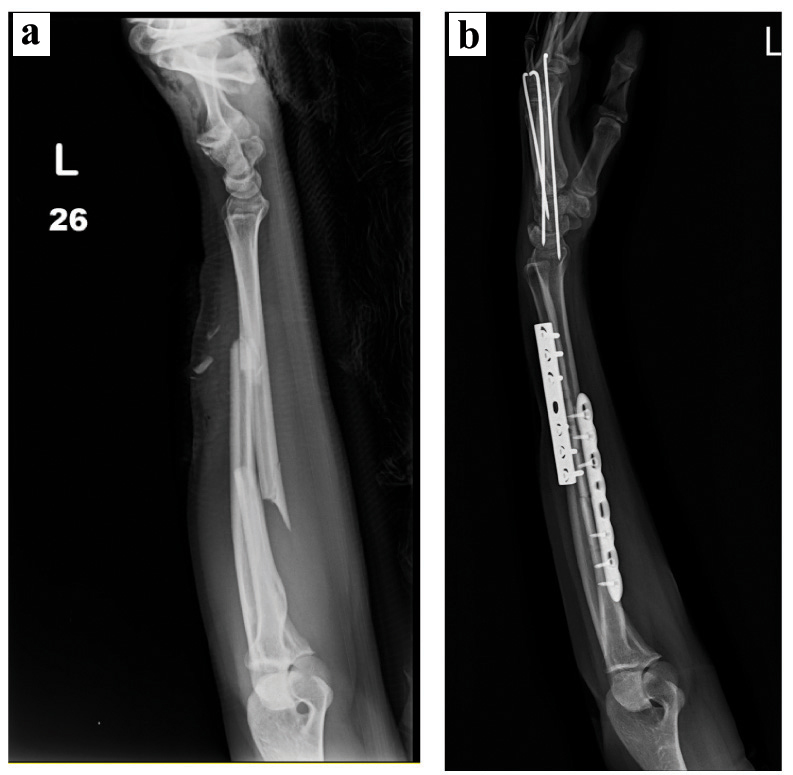
a) Preoperative lateral radiograph of the left forearm showing displacement and angulation of the radius shaft and ulnar shaft; b) Postoperative lateral radiograph of the left forearm showing internal plates with screw fixation.
Anteroposterior radiograph of the left wrist and hand showing reduced CMC joint and associated fracture, fixed with K-wires.

Posterior oblique radiograph of the left wrist and hand showing reduced CMC joint and associated fracture, fixed with K-wires.

The patient was discharged following an uneventful postoperative period. The reduction was protected for three months in a short arm plaster splint which allowed full mobilisation at the metacarpophalangeal joints distally. The K-wires were removed at three months, and active range of movement exercises were continued under the guidance of a hand therapist. Three months later, a painless full range of motion was regained and she was able to return to work.
Roentgenograms taken after the operation showed maintained reduction of the CMC joints with parallel joint surfaces at the third, sixth, twelfth, eighteenth, and 24 months, postoperatively, with anteroposterior and oblique X-rays of the wrist joint and hand. The last X-ray showed no evidence of subluxation or arthritis affecting CMC articulation [Table/Fig-8]. Functional assessment was conducted, with the DASH score for the injured left hand improving from 74.2 to 0 from month one to month 24, indicating a nearly full return to her pre-injury status. The patient had a full range of motion of the metacarpal joint (25° of extension-90° of flexion), the proximal interphalangeal joint (0°-110°) and the distal interphalangeal joint (0°-80°) of the first and fourth digits. Her hand function was unchanged at 6 and 24 months postoperatively. The patient returned to her previous occupation within three months and claimed complete functional recovery without substantial pain, weakness, or swelling.
Two years postoperative anteroposteror radiograph of the wrist and hand showing maintained reduction and alignment at CMC joints with complete healing of fractures.

Discussion
Both carpal and CMC dislocations stem from wrist trauma, including perilunate injury from hyperextension trauma, all of which require prompt care, as noted by Lefere M et al., in their recent discussion of rare dislocations [2]. This article complements their study by presenting a case of rare dislocation.
The CMC joints are modified compound saddle joints with an articular cavity within the capsule of each joint. The configuration of the bases of the metacarpals play an important role in the pattern of CMC dislocations. CMC articulations and joints are stabilised by volar and dorsal ligaments, transverse metacarpal ligaments, long flexor and extensor tendons, and intrinsic muscles of the hand. Dorsal ligaments are stronger than volar ligaments [3,4]. CMC joint dislocations are rare, which may be why they are often overlooked and misdiagnosed [5], while massive oedema, interposed fracture fragments from the bases of the metacarpals, overlapping of the bases of the metacarpals, and interposed ligament structure are several factors that may prevent successful closed reduction [6]. Joint stiffness, muscle atrophy, and decreased grip strength may result from failure to diagnose these injuries or inability to maintain an anatomic reduction [5].
We report a divergent dislocation between the second, third and fourth rays, an extremely infrequent pattern of injury which is difficult to diagnose because of gross swelling of the hand and no obvious abnormality detected by the routine posteroanterior view.
It is generally assumed that dorsal dislocation is caused either by direct force on the metacarpal bases from the anterior or by an indirect force that is transmitted through the metacarpal shafts after a dorsal blow to the distal aspect of the bones [7]. A dorsal dislocation of the CMC joints is seen more often than a volar dislocation, and affects the fourth and fifth digits [8]. El Kadi K et al., classifies the volar dislocations into radiopalmar and ulno-palmar, keyed to how the fifth metacarpal base is displaced [9]. Garg R et al., found that the metacarpal bone could deviate to either the ulnar or radial side [10].
Typically, volar and ulnar dislocations are rare, and we could find only few published reports [3,9-12]. The main clinical features associated with this injury are swelling, shortening of the little finger, pain at the base of the fifth metacarpal and an axial deformity of the little finger.
Ulno-palmar dislocations have been successfully treated by closed reduction without fixation, and by open reduction and K-wire fixation [9,13]. Radio-palmar dislocations are inherently unstable because of the tearing of all the ligaments and tendon attachments at the base of the fifth metacarpal [9]. A case series by Nazarian N et al., clearly demonstrated routine posterior-anterior view of the injured hand showing loss of parallelism or of symmetry at the CMC joints, the overlap of joint surfaces, or apparent shortening of the metacarpals [6].
Schaefer N et al., recommended that reduction should be achieved as soon as possible, and in the present case second, third, and fourth metacarpals were reduced onto the carpals and maintained with internal fixation [1].
Valente M et al., claimed that generally, in acute fracture-dislocations, reduction may be achieved by closed manipulation, but that maintenance of the reduced state may be difficult [13]. Open reduction may be necessary, followed by immobilisation [13]. Nazarian N et al., reported that it is difficult to perform the closed reduction under circumstances such as massive oedema, interposed fracture fragments of the metacarpal bases or distal carpal row, overlapping of the metacarpal bases, or interposed ligament structure [6]. The keys to this highly complex anatomic architecture are stabilisation and reduction of the third metacarpal base area.
CMC fracture-dislocations are often unstable. A delayed diagnosis and inappropriate reduction method can result in decreased grip strength and post-traumatic CMC arthritis [11].
Conclusion
Radiopalmar open dislocation of the second, third, and fourth CMC joint is a rare injury, and very few cases have been reported in the literature. This report highlights an extremely unusual case of open volar dislocations of the second, third, and fourth CMC joints associated with an extra-articular fracture of the first and fourth proximal phalanges, and fracture of radius shaft and ulna shaft. Open reduction and pinning combined with a period of immobilisation followed by hand physiotherapy resulted in excellent function.
Disclaimer
The Board of Ethics at Kaohsiung’s Armed Forces General Hospital approved this project. The patient formally consented and the work was conducted according to the World Medical Association Declaration of Helsinki.
[1]. Schaefer N, Elliott D, Loveridge J, Volar dislocation of the index, middle, and ring carpometacarpal joints: a reviewPlastic and Reconstructive Surgery Global Open 2015 3(3):e33010.1097/GOX.000000000000029725878941 [Google Scholar] [CrossRef] [PubMed]
[2]. Lefere M, Dallaudiére B, Omoumi P, Cyteval C, Larbi A, Rare carpometacarpal dislocationsOrthopaedics & Traumatology: Surgery & Research 2016 102(6):813-16.10.1016/j.otsr.2016.04.00327210506 [Google Scholar] [CrossRef] [PubMed]
[3]. Hudak PL, Amadio PC, Bombardier C, Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG)Am J Ind Med 1996 29(6):602-08.10.1002/(SICI)1097-0274(199606)29:6<602::AID-AJIM4>3.0.CO;2-L [Google Scholar] [CrossRef]
[4]. Kumar R, Malhotra R, Divergent fracture-dislocation of the second carpometacarpal joint and the three ulnar carpometacarpal jointsJ Hand Surg Am 2001 26(1):123-129.10.1053/jhsu.2001.2015311172378 [Google Scholar] [CrossRef] [PubMed]
[5]. Wright AC, Muir L, A review of published radiographic indicators of carpometacarpal dislocation including their application to volar dislocations through a case studyJ Emerg Med 2015 49(3):e69-71.10.1016/j.jemermed.2015.01.00525881888 [Google Scholar] [CrossRef] [PubMed]
[6]. Nazarian N, Page RS, Hoy GA, Hayton MJ, Loosemore M, Combined joint fusion for index and middle carpometacarpal instability in elite boxersJ Hand Surg Eur Vol.2014 2014 39(3):242-48.10.1177/175319341348746923649012 [Google Scholar] [CrossRef] [PubMed]
[7]. Pundkare GT, Patil AM, Carpometacarpal joint fracture dislocation of second to fifth fingerClin Orthop Surg 2015 7(4):430-35.10.4055/cios.2015.7.4.43026640624 [Google Scholar] [CrossRef] [PubMed]
[8]. Büren C, Gehrmann S, Kaufmann R, Windolf J, Lögters T, Management algorithm for index through small finger carpometacarpal fracture dislocationsEuropean Journal of Trauma and Emergency Surgery 2016 42(1):37-42.10.1007/s00068-015-0611-z26660674 [Google Scholar] [CrossRef] [PubMed]
[9]. El Kadi K, Sbiyaa M, Alami B, Rabhi I, Marzouki A, Lahrach K, Isolated radial volar dislocation of the fifth carpometacarpal joint: a rare injuryPan African Medical Journal 2014 16(1):1-5.10.11604/pamj.2013.16.90.321824711880 [Google Scholar] [CrossRef] [PubMed]
[10]. Garg R, Gupta R, Singh B, Siwach R, Volar dislocation of four carpometacarpal joint: A rarest injuryInternational Journal of Biomedical Research 2014 5(10):646-48.10.7439/ijbr.v5i10.749 [Google Scholar] [CrossRef]
[11]. Apergis E, Carpometacarpal (CMC) Dislocations or Fractures-Dislocations Excluding the ThumbIn: Fracture-Dislocations of the Wrist 2013 MilanoSpringer:239-71.10.1007/978-88-470-5328-1_9 [Google Scholar] [CrossRef]
[12]. Mito K, Nakamura T, Sato K, Toyama Y, Ikegami H, Dorsal dislocations of the second to fifth carpometacarpal joints: a case reportJournal of the Asia-Pacific Federation of Societies for Surgery of the Hand 2008 13(2):129-32.10.1142/S021881040800389X19054847 [Google Scholar] [CrossRef] [PubMed]
[13]. Valente M, Saggin G, Alecci V, Pure isolated dorsal dislocation of the fifth carpometacarpal jointMusculoskeletal Surgery 2009 93(2):97-100.10.1007/s12306-009-0029-z19711009 [Google Scholar] [CrossRef] [PubMed]