Multiple Recurrent Simultaneous Salivary Calculi
Bhushan P Mundada1, Sanidhya Surana2, Nitin Bhola3, Shrenik Oswal4, Prachet Dakshinkar5
1 Assistant Professor, Department of Oral and Maxillofacial Surgery, Sharad Pawar Dental College and Hospital, Sawangi, Wardha, Maharashtra, India.
2 Fellow Research, Department of Oral and Maxillofacial Surgery, Sharad Pawar Dental College and Hospital, Sawangi, Wardha, Maharashtra, India.
3 Professor, Department of Oral and Maxillofacial Surgery, Sharad Pawar Dental College and Hospital, Sawangi, Wardha, Maharashtra, India.
4 Assistant Professor, Department of Oral and Maxillofacial Surgery, Sharad Pawar Dental College and Hospital, Sawangi, Wardha, Maharashtra, India.
5 Assistant Professor, Department of Oral and Maxillofacial Surgery, Sharad Pawar Dental College and Hospital, Sawangi, Wardha, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bhushan P Mundada, Assistant Professor, Department of Oral and Maxillofacial Surgery, Sharad Pawar Dental College and Hospital, Sawangi, Wardha-442001, Maharashtra, India.
E-mail: pbmundada4@gmail.com
Calculus, Parotid, Submandibular
A 34-year-old female reported to our department with a complaint of extra oral pus discharge on left side since 10 days with associated pain in left preauricular region since last two months and fever since 15 days. Pain was intermittent, aggravated on mastication and not relieved after medication. She had similar complain 10 years back, for which surgical intervention was done, although the procedure was unclear as she lost her previous documents.
On examination a pale reddish swelling was present in the left preauricular region with pus draining fistula 1.5 cm anterior to angle of mandible [Table/Fig-1]. Intraorally all teeth were present with healthy periodontium and no obvious pathology seen. A single stony hard swelling palpated in the floor of mouth on right side in canine premolar region measuring 10×5 mm, with inflammation and relatively reduced salivary flow at ductal opening, provisionally diagnosing salivary calculi in left parotid and right submandibular gland with a secondary infection and extra oral fistula in parotid region. To confirm the diagnosis Orthopantomogram (OPG), mandibular occlusal radiograph and Ultrasonography (USG) were advised.
Clinical picture showing swelling over left preauricular region with a pus draining fistula on angle of mandible.

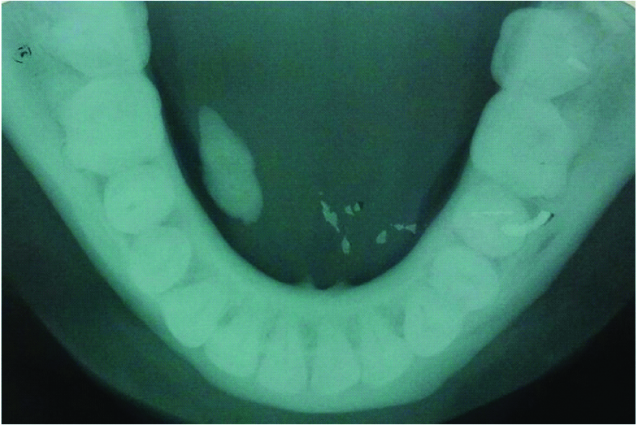
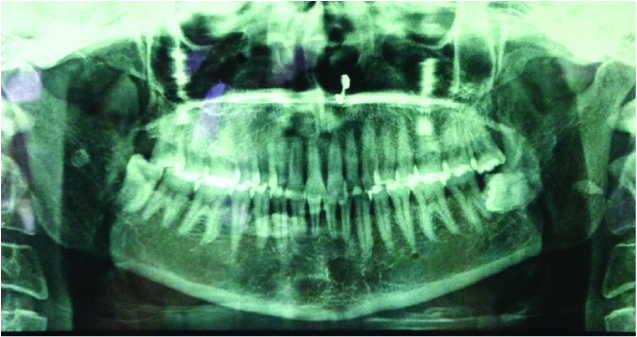
Occlusal view confirmed the same findings in right side of floor of mouth with normal counterpart [Table/Fig-2]. OPG showed radio-opacity in bilateral ramus region and right body region of mandible suggesting multiple sialoliths [Table/Fig-3]. USG revealed both parotid glands were slightly heterogeneous in echo texture. Left parotid glands duct was dilated with chronic inflammatory changes showing intraparenchymal Salivary Calculi (SC) measuring approximately 10.3×3.7 mm. Right parotid gland revealed two intraparenchymal calculi of size 10.8×3.0 mm and 7.6×3.1 mm, moreover, duct was minimally dilated. Single salivary calculi present in right sided Wharton’s duct measuring of 11×5 mm with obliteration of ductal lumen. However, left sided submandibular gland and duct appeared normal. These findings confirmed the provisional diagnosis.
Occlusal radiograph showing radiopacity of approx size 10×5 mm on right side mimicking salivary calculi.
OPG showing a radio opacity in bilateral ramus region and right body region of mandible suggesting multiple sialoliths.
To rule out formation of calculi at other places USG abdo-pelvis and Magnetic Resonance Imaging (MRI) brain were done which revealed no positive findings. So, the patient was advised medicinal therapy and surgical removal of all the calculi. Unfortunately surgical intervention could not perform as the patient did not turn for further treatment.
Discussion: Salivary sialoliths are one of the most common diseases of salivary glands. Uni-lateral presentation is more common while bilateral involvement is rare. Normal presentation is a single small/giant stone in a single gland, multiple calculi involving single gland or presence in multiple glands bilaterally. Incidence of bilateral involvement of parotid (32%) and submandibular glands (22%) had been reported. Only (3%) documented cases have been found to have such glandular stones in multiple salivary glands and only (5%) of them have more than three or more stones [1,2]. In present case, salivary calculi were present simultaneously in the left parotid (1 SC), right parotid (2 SCs) and right submandibular gland (1 SC) which makes it a rare case report.
Patient usually complains of pain and swelling around the gland duct during meal time. This patient initially had the same complaint on left side, but due to negligence it eventually progressed into a fistula with pus discharge. Contrary to literature, disease in right parotid and right submandibular gland was asymptomatic.
Odontogenic infection should be considered as a differential diagnosis, but it was rule out as no carious tooth was found and the pain only aggravated on mastication, which did not get relieved with medications.
Simple occlusal radiograph, OPG and posteroanterior view can help to identify the parotid and submandibular calculi. Modern diagnostic aids like Computed Tomography (CT), MRI, sialography and sialoendoscopy give precise information regarding the specificity, exact location and dimensions of the calculus [3].
Small salivary calculi can be managed by milking, very small stones need no intervention just medicinal therapy alone either dissolves them or they tend to come out on their own with increased salivary flow. Chewable Vitamin C tablets and sialagogues like pilocarpine help increasing the flow. Short wave infrared heating also causes ductal contraction and thus removal of the duct stone [3]. Sialodochoplasty, dormia basket and lithotripsy allows removal of calculi in less invasive way while more invasive surgical procedures like subtotal or total parotidectomy are indicated for recurrent or cases with multiple calculi in same gland [4].
Large sialoliths (Megaliths) are those measuring more than 1.5 cm in diameter, warrants surgical removal [5]. Present case did not have megaliths but the size was big enough to do a surgical intervention as fistula formation and pus discharge were seen.
[1]. Biddle RJ, Arora S, Giantsialolith of the submandibular salivary glandRadiol Case Resp 2008 3(1):10110.2484/rcr.v3i2.10127303513 [Google Scholar] [CrossRef] [PubMed]
[2]. Lustman J, Revag E, Melamed Y, Sialolithiasis: a survey on 245 patients and a review of the literatureInt J Oral Maxillofac Surg 1990 19(3):135-38.10.1016/S0901-5027(05)80127-4 [Google Scholar] [CrossRef]
[3]. Gadipelly S, Srilatha T, Sheraz BS, Vijaykumar N, Parotid sialolith-a case report and review of literatureInt J Contemp Med Res 2016 3(4):1211-13. [Google Scholar]
[4]. Konstantinidis S, Paschaloudi S, Triaridis S, Fyrmpas G, Sechlidis S, Constantinidis J, Bilateral multiple sialolithiasis of the parotidgland in a patient with Sjögren’s syndromeActa Otorhinolaryngol Ital 2007 27:41-44. [Google Scholar]
[5]. Banerjee N, Mitra S, Kundu S, Giant parotid sialolithiasis: report of a case with review of literatureInt J Scient Res Manag 2015 3(4):2595-604. [Google Scholar]