Introduction
Complementary and Alternative Medicine (CAM) as defined by National Center for CAM, a collection of healthcare systems, diverse medical, concerned practices and medicines that are not expected to be a subset of conventional medicine [1].
CAM is now practiced all over the world [2]. CAM also known in India as non allopathic Indian medicines is gathering credit in India and all over world. Ayurveda, siddha, unani and homeopathy are the non allopathic systems practiced in India that satisfies almost 80% of medical requirements of population [3,4].
The origin of ayurveda medicine in India dates more than 5000 years [5]. Ayurveda forms the commonly practiced non allopathic medicine especially in rural India, where almost 70% of people live [3]. India today officially recognises ayurveda and other systems of indigenous medicine. In 1995, Government of India (GOI) had accorded department known as Ayurveda, Yoga, Unani, Siddha, Homeopathy (AYUSH) [6]. In 2009, Government of India (GOI) had taken step to foster Indian Systems of Medicine on promotion of AYUSH [4].
Ayurveda is used in India, Nepal, Sri Lanka and is increasingly used in Western countries [7,8]. Western allopathic medicine had good results in handling acute medical crisis and ayurveda has ability to manage chronic disorders that are difficult to treat by Western medicine [9].
Ayurveda provides cost effective techniques that are supposed to have minimal side-effects in contrast to that are seen in Western allopathic medicine [5]. The research in ayurveda literature during past 100 years shows encouraging results, especially in management of chronic disorders associated with aging process [5]. Despite growing research and understanding, there is limited information on the use of ayurveda [8].
There is no study reported so far to assess the perceptions of patients as to why patients take ayurvedic medicines despite availability of allopathic treatment. What are the needs of the patients visiting ayurveda OPD and why allopathic physicians prescribe ayurveda. To understand if the needs of physicians to use ayurveda and patients to seek Ayurvedic treatment correlate, we did a questionnaire based study.
Materials and Methods
Complex articular fractures of the distal radius extending into a cross-sectional questionnaire based study was undertaken in 300 patients attending ayurveda OPD and 50 allopathic physicians of a tertiary care hospital. Institutional Ethics Committee permission (EC No: EC/OA-50/2014) was taken before starting the study. New and old patients more than18 years of age, of both gender, willing to give consent and attending the ayurveda OPD of medical college and tertiary care hospital were included. Objectives of the study were explained to participants, the participation was voluntary and written consent was taken prior to enrollment. The study was conducted from September 2014 to September 2016. The demographic details were noted, questionnaire was administered and collected after 20-30 minutes. The level of satisfaction to ayurveda therapy was measured by VAS from 0 (no satisfaction) to 10 (complete satisfaction).
A total of 369 patients were approached out of which 316 consented, 300 were included and 75 physicians were approached, 50 willing to participate were included. The allopathic practitioners were selected by randomisation based on the designation or at least 10% of the physicians from a department were enrolled after randomisation. Those not willing to participate or did not return the questionnaire or returned incompletely filled forms were excluded from study. Around 3000 new patients attend ayurveda OPD in a year; sample size taken was 10% i.e., 300 patients. The privacy and confidentiality of data were maintained throughout the study. Test-retest reliability was estimated with subsample of 10 patients and 5 physicians by taking two interviews seven days apart. Internal consistency reliability was assessed by Cronbach’s-alpha coefficient was calculated by Statistical Package for the Social Sciences (SPSS) software version 20.0 which was 0.74 for patient’s questionnaire and 0.82 for physicians questionnaire. Modified Kuppuswamy’s Socioeconomic Classification (MKSC) was used for socioeconomic status [10].
Questionnaire for patients included information on demographic profile, questions on the disease and symptoms patients are suffering from, the physicians from different medical branches they had visited, reasons for discontinuing previous treatment, reasons for believing and not believing in ayurveda and other questions.
Questionnaire for physicians included questions on demographic profile, their belief on ayurveda, reasons for believing and not believing in ayurveda, views of physician on diseases for which there is need to obtain treatment from complementary branch of medicine, reasons for patients not completing current treatment, diseases for which there is need to develop ayurveda treatment and other questions.
In the study, procedures were followed in accordance with ethical guidelines of Institutional Ethics Committee and Declaration of Helsinki, adopted by 18th World Medical Assembly, revised in 64th General Assembly, October 2013.
Statistical Analysis
Data were entered in MS Excel 2010, responses coded and analysed. Descriptive statistics was expressed in actual numbers, mean±standard deviation, frequency and percentage. A p-value <0.05 was considered statistically significant. Student’s unpaired t-test was used to compare the scores of VAS and parametric data. Categorical variables were compared using chi-square test. The statistical analysis in present study was done using GraphPad Prism software (version 5.0), and SPSS version 20.0.
Results
Patient’s
The mean age of patient attending ayurveda OPD was 44.2±14.2 years (range 18-84 year) (Female=42.45±13.44, Male=47.81±15.01). There were 203 females and 97 males. About 283 patients were from urban and 17 from rural area. Out of 300, 250 patients were married (Female=168, Male=82), and 50 were unmarried. In the employment status, there were 60 government employees, 36 self-employed, 36 students, 21 professional, 123 housewives, 21 retired males and 3 unemployed males. Age, education and socioeconomic distribution in patients are given in [Table/Fig-1]. Out of 300, 265 (88.33%) patients visited OPD on advice of friends and relatives, 18 (6%) due to previous physician reference, 17 (5.67%) patients visited OPD due to information on media which included 5 patients due to television, 5 by reading newspaper, 3 by internet, 2 by book and 2 by radio.
Age, education and socioeconomic distribution of patients.
| Variables | Numbers |
|---|
| Age (years) |
| <20 | 17 |
| 20-40 | 104 |
| 40-60 | 138 |
| 60-84 | 41 |
| Education |
| <10 standard | 93 |
| 11-12 | 110 |
| Diploma | 18 |
| Graduates | 62 |
| Postgraduates | 17 |
| KSC |
| Upper-Lower class | 199 |
| Lower-middle class | 49 |
| Upper-middle class | 40 |
| Upper class | 7 |
| Lower class | 5 |
KSC: Kuppuswamy’s socioeconomic classification
All 300 patients attending the ayurveda OPD believed in ayurveda. The average VAS score for satisfaction to ayurveda therapy was 7.67±1.58. The difference in average VAS for females (7.81±1.69) and males (7.17±1.43), was statistically significant (p=0.002). The average VAS for urban patients (7.68±1.54) and rural (7.58±1.42), not statistically significant difference (p=0.794). In females, VAS for housewife (7.84±1.23) and remaining female patients (7.78±1.93), the difference was not statistically significant (p=0.806).
Among 300, 192 (64%) patients had taken treatment from various systems of medicine and then visited ayurveda OPD, while 108 (36%) patients directly visited ayurveda OPD. Different branches of medicine that patients visited before coming to ayurveda OPD is given in [Table/Fig-2]. The patient’s reasons for preferring ayurveda medicine and other complementary medicines are given in [Table/Fig-3]. About 88.02% patients had stopped treatment by previous system of medicine, while 157/173 (90.75%) taking Allopathy discontinued treatment. Suggestions of operative treatment were some of the other reasons for stoppage of allopathy treatment. The symptom distribution in patients attending ayurveda OPD is given in [Table/Fig-4] and the accompanying disease distribution in patient is given in [Table/Fig-5].
Different branches of medicine patients visited and stopped treatment before coming to ayurveda OPD.
| Different branches of medicine | Number of patients | Stopped treatment |
|---|
| Allopathic (MBBS/MD/MS) | 173 | 157 |
| Ayurvedic (BAMS [Bachelor of Ayurveda, Medicine and Surgery]/MD) | 5 | 5 |
| Homeopathic (BHMS [Bachelors Degree in Homeopathy Medicine and Surgery]/MD) | 9 | 6 |
| Allopathic and Homeopathic | 4 | 0 |
| Allopathic and ayurvedic and Homeopathic | 1 | 1 |
| Total | 192 | 169 |
Patients reasoning for preferring ayurveda and other complementary medicines.
| Reasons | Ayurveda Alone | Other Complementary medicine | Total |
|---|
| Maintaining good health | 77 | 136 | 213 |
| No adverse side effects | 71 | 129 | 200 |
| Favourable personal/family experiences | 41 | 63 | 104 |
| Traditional science known and practiced for many centuries | 11 | 10 | 21 |
| Can be safely combined with modern medicines | 5 | 8 | 13 |
Symptom distribution inpatients attending the ayurveda OPD.
| Symptoms | Number of patients |
|---|
| Knee joint pain | 69 |
| All joint pain | 36 |
| Backache | 21 |
| Dyspepsia | 18 |
| Constipation | 14 |
| Hair loss/Bleeding per rectum | 13‡ |
| Abdominal pain/Tingling numbness | 10‡ |
| Sore throat | 9 |
| Allergy/Sleep disturbance/Weight gain | 8‡ |
| Anal pain/Irregular menses | 6‡ |
| Urinary Incontinence/Radiating pain lower limb | 5‡ |
| Acne/Neck pain/Headache | 4‡ |
| Urinary tract infection (UTI)/Infertility/White discharge | 3‡ |
| Anorexia/wrist joint pain/pedal edema/hyperpigmentation | 2‡ |
| Weight loss/ Psoriasis/Primary Infertility/Obesity/Premature ejaculation/Short stature/Treated case of Buccal Cancer | 1‡ |
‡Indicates the number of patients for each disease mentioned in the corresponding row
Physicians
The mean age of the physicians was 39.10±9.39 (25 to 58 years). Out of 50, 22 were females and 28 male physicians. The designation included 8 Senior residents, 16 Assistant Professors, 10 Associate professors and 16 Professor. The educational qualification and years of experience of physicians is given in [Table/Fig-6]. The reasons for discontinuing allopathy by patients and reasons according to physician are given in [Table/Fig-7].
Accompanying disease distribution in patients attending ayurveda OPD.
| Diseases | Number of patients |
|---|
| Osteoarthritis | 77 |
| Backache | 21 |
| Piles | 20 |
| Acidity | 16 |
| Irritable Bowel Syndrome | 14 |
| Alopecia/Diabetes Mellitus | 13 |
| Obesity | 12 |
| Rheumatoid arthritis/Sciatica/Cervical spondylitis | 10§ |
| Allergy/Lumbar spondylitis/Insomnia | 8§ |
| Acne/UTI | 6§ |
| Malignancy/Psoriasis/Viral Hepatits | 5§ |
| Primary Infertility/Sinusitis/Hypertension/Migraine | 4§ |
| Allergic rhinitis/Anemia/Polycystic Ovarian Disease/Varicose veins/Hypothyroid/Leucorrhea/Menorrhagia | 3§ |
| Dysfunctional Uterine Bleeding/Anal fissure/Gout/Urticaria | 2§ |
| Asthma, Ankylosing spondylitis, Frozen shoulder, Hernia, Hyperthyroidism, Hyperpigmentation, Irregular menses, Microphallus, Prolapse Intervertebral Disease, Premature ejaculation, Dysplasia buccal mucosa, Rhinitis, Vesicular calculus, Short stature | 1 |
§ Indicates the number of patients for each disease mentioned in the corresponding row
Educational qualification and years of experience of physicians.
| Qualification | Number of physicians | Experience (Years) | Number of physicians |
|---|
| MBBS (Bachelor of Medicine and Bachelor of Surgery) and MD (Doctor of Medicine) physicians | 25 | 1 to 5 | 20 |
| MD-DM (Doctorate of Medicine) | 02 | 5 to 10 | 11 |
| MBBS-MS (Master of Surgery) | 12 | 10 to 20 | 10 |
| MBBS-MS-MCH (Master of Chirurgiae) | 06 | 20 to 30 | 05 |
| MBBS-DNB (Diplomate of National Board) | 05 | >30 | 04 |
Patients reasoning for discontinuing from allopathy treatment and physicians views on patients reasons for discontinuing allopathy treatment†.
| Reasons | Number of patients | Percentage (Out of 157) | Physicians views (Number of physicians) | Percentage(Out of 50) | p-value |
|---|
| Not satisfied with the previous treatment | 138 | 87.89 | 19 | 38 | <0.0001 |
| Increased Cost of treatment | 22 | 14.01 | 28 | 56 | <0.0001 |
| Adverse drug effects | 26 | 16.56 | 25 | 50 | <0.0001 |
| Lengthy treatment | 45 | 28.66 | 21 | 42 | 0.082 |
| Resistance/Intolerance to treatment | 4 | 2.55 | 16 | 32 | <0.0001 |
| Other reasons | 2 | 1.27 | 0 | 0 | ------- |
†Patients and physicians opted for more than one option
Out of 50, 16 (32%) didn’t believe in ayurveda, while 11 (22%) physicians were not sure, 23 (46%) believed in ayurveda, which included 11 from Medicine and allied departments and 12 were from Surgery and its allied departments. Among 50, 17 (34%) physicians found patients to use other alternative systems of medicine. Among 50 physicians, 36 (72%) physicians would prefer use of alternative systems of medicine, among them 22 physicians gave first preference to ayurveda and yoga, 12 gave preference to homeopathy and one each for acupuncture and naturopathy. In second preference, 11 physicians preferred homeopathy followed by ayurveda, yoga (10) and one each for naturopathy, unani, yoga, reiki and acupuncture. About 10 (20%) physicians had come through patients that had satisfactory result after taking ayurveda therapy while 34 (68%) physicians had not come across any patients that had satisfactory treatment after taking ayurveda therapy and 6 (12%) physicians were not sure if they had across any patients that had satisfactory treatment after taking ayurveda therapy.
Among 50 physicians, 24 (48%) did not believe while 26 (52%) believed there is need to develop ayurveda treatment for different disease conditions; this included 13 from medicine and allied department and 13 from surgery and its allied department. The most common reason for physicians to believe in ayurveda were, 25 (50%) traditional science known and practiced for centuries followed by no adverse effect 5 (10%), 11 (22%) favourable personal/family experiences, 14 (28%) safely combined with modern medicines and 10 (20%) for maintaining good health. Physician’s reason for not believing in ayurveda is given in [Table/Fig-8]. According to physicians, diseases for which there is need to develop ayurveda treatment is given in [Table/Fig-9]. The matching in percentages of patients need and physicians need to develop ayurveda treatment for common diseases is shown in [Table/Fig-10].
Physicians reasons for not believing in ayurveda.
| Reasons for not believing in ayurveda | Number | Percentages |
|---|
| Lack of scientific evidence | 21 | 42 |
| Unavailability of standardised formulation | 13 | 26 |
| Not suitable for emergency care | 14 | 28 |
| Adulteration/malpractice | 13 | 26 |
| Unfavourable personal/family experiences | 4 | 8 |
| No knowledge | 7 | 14 |
| Costly | 1 | 2 |
||Physicians opted for more than one option
According to physicians, diseases for which there is need to develop ayurveda treatment.
| Diseases | Number |
|---|
| Arthritis | 6 |
| Diabetes Mellitus | 6 |
| Backache | 5 |
| Malignancy | 4 |
| Hypertension/Irritable bowel syndrome | 4** |
| Piles/Obesity/Hair loss | 3** |
| Allergy | 2 |
| Headache | 2 |
| Degenerative spinal disease/Meningioma/Gullian Barrie Syndrome | 1** |
| Viral hepatitis/Multi drug resistant Tuberculosis/Cataract | 1** |
| Chronic condition/Lifestyle related | 1** |
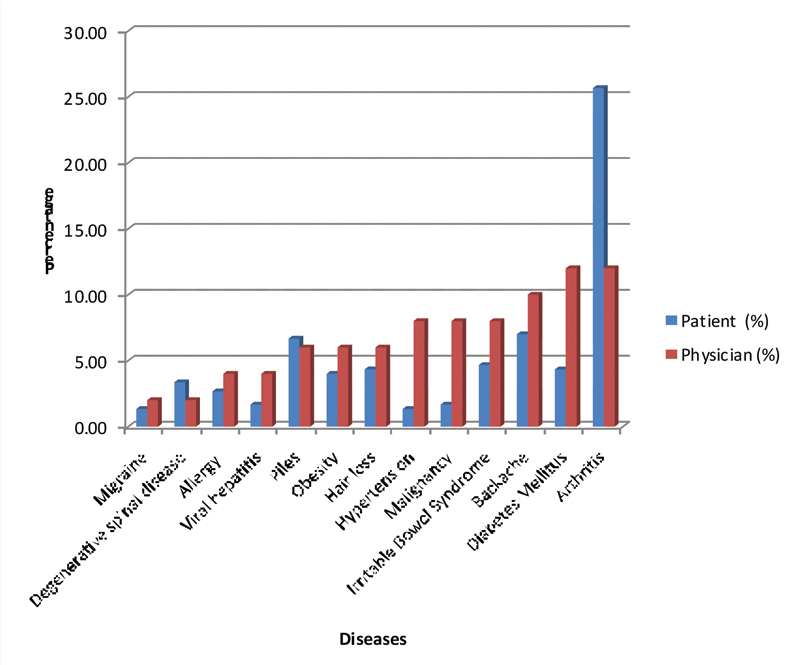
Matching of percentage, of patients need to attend ayurveda OPD and percentage of physicians that feel the need to develop ayurveda treatment for common diseases.
Discussion
In India, there is coexistence of modern medicine and multiple traditional health systems in clinical practice of medicine especially for treatment of chronic diseases [11,12].
In present study, majority of patients were aged 40-60 years, females and from urban area. The level of satisfaction by ayurveda was more for females than males. A study by Satow SW et al., had patients of 52.5 years (18 to 80 years) and majorly females (65.5%) [8] while study by Roy V et al., had 70% patients that used CAM on advice of family and friends [13]. As per Ahmed TE, there were 31% housewives, 23.9% Government and 30.1 % non government officer that used CAM [14]. Similar results by studies from Chatterjee B et al., and Abdul RJ et al., [9,15]. Thus, the demographic profile of the patients in this study was similar to other studies. Being a municipal hospital in metropolitan city, majority patients were from urban area and lower socioeconomic status. The role of family, friends and media has an importance as source of knowledge for patients.
The most common reason for discontinuing allopathy treatment by the patients was lack of satisfaction with previous treatment and the lengthy nature of treatment. According to physicians, prime reason for the patients to discontinue treatment was cost of treatment followed by adverse drug effects and resistance/intolerance to treatment. As per study by Roy V et al., there is inadequate doctor-patient communication about concomitant usage of CAM with allopathic medicine [13]. In present study, 90.75% patients had discontinued previous allopathy treatment, thus to change this, there is urgent need to change the attitude of patients through patient education to complete allopathy treatment.
There were various studies to evaluate the use of CAM but no studies evaluating only ayurveda system of medicine. In present study, physicians believed in ayurveda as it is traditional known science and can be safely combined with modern medicines. In study by Kong FH et al., 75% of physicians believed in CAM and 50% opined that CAM is better than allopathy in certain cases because of cost effectiveness and fewer side effects. According to the study by Sharma H et al., 62% of the physicians had recommended yoga and ayurveda as the commonly preferred CAM modality while 39% physicians had recommended yoga and ayurveda to patients [5]. In the study by Chaterjee B et al., patients most commonly preferred allopathy followed by ayurveda and homeopathy [9]. In study by Kenji F et al., the physician’s reason to not prefer CAM was because of no scientific evidence and lack of knowledge on CAM [16]. Also study by Kenji F et al., desire to receive CAM by patients and the limitations of modern western medicines were the reasons given by physicians to integrate CAM therapies [16].
In present study, patient’s attended ayurveda OPD for symptoms that were knee joint pain, all joint pain and backache. Physicians feel the need to develop ayurveda treatment were majorly for arthritis, diabetes mellitus and backache. Thus, the patient’s need to attend ayurveda OPD and the physicians consideration for the need to develop ayurveda treatment matched for 13 diseases. Study by Selvaraj K et al., found that 40% of the patients attending Siddha OPD were having arthritis as the most common symptom [17]. As reported by Kong FH et al., physicians considered CAM better than allopathic treatment in diseases like psychological/psychiatric disorders, chronic illnesses, joint problems, bronchial asthma, allergic disorders and skin conditions [4]. In study by Chatterjee B et al., for obesity, ayurveda was the most popular choice of treatment [9]. Doctors and medical students believed that CAM should be taught and is most useful in psychiatry, rheumatology, general medicine, oncology and dermatology [2]. Peter K and Erik WB, concluded that CAM training had 0-30% lower mortality rates and healthcare costs in patients whose general practitioners had practiced CAM [18].
The National Institute of Health states that 4 out of 10 Americans and in Switzerland 11% used some form of CAM [18]. The desire to practice CAM have increased in Japan from 1999 to 2006. The doctors in Japan were familiar and practicing CAM, also attending training courses related with CAM [16]. CAM model is followed in China, Russia with substantial success and is gaining momentum in Vietnam, Sweden, Germany and Italy [7].
With proper integrative strategies of AYUSH systems along with allopathy a dream of healthy India can be achieved. AYUSH systems may offer better management of chronic and metabolic diseases, psychosomatic conditions, disease prevention, and health promotion. While modern medicine has worthful contributions for surgical interventions, diagnostics emergency medicine and infectious diseases [19].
Integrative healthcare programmes will play a considerable role in 21st century. The shortfall of satisfactory treatment by a single system of healthcare has been addressed by upcoming government sponsored national research institutes for CAM in Sweden, United Kingdom, Europe and United States [20]. In India when it comes to healthcare, people look forward to choose allopathy, AYUSH or a combination for various health conditions. In study by Subramanian K and Midha I, majority of Indian students believed incorporating CAM into the healthcare system as viable alternative to conventional medicine [21]. The need for integrated medicine in medical curriculum is highlighted by various studies [2,4,7,16]. In India with inclusion of Pharmacology subject in BAMS curriculum, there will be increase in integrative prescription [22].
Limitation
There were certain limitations of present study, as the study was done in one hospital, it may not represent data from the general population. Since, this was a questionnaire based study, the possibility of recall bias cannot be excluded.
Conclusion
There is need to undertake orientation programs related to CAM for Physicians and medical students. There is need of patient education cell in hospitals to educate them about compliance of therapies. Evidence based clinical trials should be done to scientifically validate ayurveda treatment in therapeutic areas which are unmet clinical needs.
[1]. Dietlind LW, Vincent A, Elkin PL, Loehrer LL, Cha SS, Bauer BA, Physicians’ attitudes toward complementary and alternative medicine and their knowledge of specific therapies: a survey at an academic medical centerEvidence-Based Complementary and Alternative Medicine 2006 4(4):495-501.10.1093/ecam/nel03617173114 [Google Scholar] [CrossRef] [PubMed]
[2]. Münstedt K, Harre H, von Georgi R, Hackethal A, Complementary and alternative medicine: comparison of current knowledge, attitudes and interest among german medical students and doctorsEvidence-Based Complementary and Alternative Medicine 2011 190(1):01-07.[cited 2016 October 10]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3153080/pdf/ECAM2011-790951.pdf. DOI:10.1093/ecam/nen07910.1093/ecam/nen07919098296 [Google Scholar] [CrossRef] [PubMed]
[3]. Gogtay NJ, Bhatt HA, Dalvi SS, Kshirsagar NA, The use and safety of nonallopathic Indian medicinesDrug Saf 2002 25(14):1005-19.10.2165/00002018-200225140-0000312408732 [Google Scholar] [CrossRef] [PubMed]
[4]. Kong FH, Man LK, Shetty RS, Kamath VG, Knowledge, attitude and practice of complementary and alternative medicine (CAM) among medical practitionersIJRRMS 2013 3(2):05-09. [Google Scholar]
[5]. Sharma H, Chandola HM, Singh G, Basisht G, Utilization of ayurveda in health care: an approach for prevention, health promotion, and treatment of disease part 2-ayurveda in primary health care.Journal of Alternative and Complementary Medicine 2007 13(10):1135-50.10.1089/acm.2007.7017-B18166127 [Google Scholar] [CrossRef] [PubMed]
[6]. Gawde SR, Shetty YC, Pawar DB, Knowledge, attitude, and practices toward ayurvedic medicine use among allopathic resident doctors: a cross-sectional study at a tertiary care hospital in IndiaPerspect Clin Res 2013 4(3):175-80.10.4103/2229-3485.11538024010059 [Google Scholar] [CrossRef] [PubMed]
[7]. Patwardhan K, Gehlot S, Singh G, Rathore HC, The Ayurveda education in india: how well are the graduates exposed to basic clinical skills?Evidence-Based Complementary and Alternative Medicine 2011 41(1):01-07.[cited 2016 October 25]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3095267/pdf/ECAM2011-197391.pdf DOI:10.1093/ecam/nep11 [Google Scholar]
[8]. Satow YS, Kumar PD, Burke A, Inciardi JA, Exploring the prevalence of ayurveda Use Among Asian IndiansJournal of Alternative and Complementary Medicine 2008 14(10):1249-53.10.1089/acm.2008.010619123878 [Google Scholar] [CrossRef] [PubMed]
[9]. Chatterjee B, Biswas PC, Pancholi J, ealth awareness and popularity of alternative medicines among people of Jamnagar town: a cross-sectional studyAYU 2012 33(1):33-37.10.4103/0974-8520.10030623049181 [Google Scholar] [CrossRef] [PubMed]
[10]. Park K, The Community: Socioeconomic scale. In: Park’s Textbook of Preventive and Social Medicine 2015 23rd EditionIndiaBanarasidas Bhanot:689-90. [Google Scholar]
[11]. Balasubramanian AV, Seeing with two eyes: how professionals can help patients trying to integrate medical systemsJournal of Ayurveda & Integrative Medicine 2010 1(3):177-82.10.4103/0975-9476.7261321547045 [Google Scholar] [CrossRef] [PubMed]
[12]. Gadgil VD, Understanding ayurvedaJournal of Ayurveda & Integrative Medicine 2010 1(1):77-80.10.4103/0975-9476.5983621829307 [Google Scholar] [CrossRef] [PubMed]
[13]. Roy V, Gupta M, Ghosh RK, Perception, attitude and usage of complementary and alternative medicine among doctors and patients in a tertiary care hospital in IndiaIndian J Pharmacol 2015 :137-42.10.4103/0253-7613.15341825878370 [Google Scholar] [CrossRef] [PubMed]
[14]. Ahmed TE, Abdullah MN, Public Knowledge, Attitude and Practice of Complementary and Alternative Medicine in Riyadh Region, Saudi ArabiaOman Medical Journal 2012 27(1):20-26.10.5001/omj.2012.0422359720 [Google Scholar] [CrossRef] [PubMed]
[15]. Abdul RJ, Reem AS, Omalkhair A, Ahmed A, Faisal AS, Nagham S, Use of complementary and alternative medicine by patients with cancer in Saudi ArabiaJournal of Alternative and Complementary Medicine 2012 18(11):1045-49.10.1089/acm.2011.026622906212 [Google Scholar] [CrossRef] [PubMed]
[16]. Kenji F, Jiro I, Satoko W, Kotaro O, Kumi S, Changes in attitudes of Japanese doctors toward complementary and alternative medicine:-comparison of surveys in 1999 and 2005 in KyotoEvidence-Based Complementary and Alternative Medicine 2011 :01-07.[cited 2016 November 01]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3136716/pdf/ECAM2011-608921.pdf DOI:10.1093/ecam/nep04010.1093/ecam/nep04019465404 [Google Scholar] [CrossRef] [PubMed]
[17]. Selvaraj K, Srinivasan M, Duraisamy V, Ramaswamy G, Venugopal V, Chinnakali P, Morbidity profile of elderly outpatients attending selected sub-district Siddha health facilities in Tamil Nadu, IndiaAncient Sci Life 2016 35:212-16.10.4103/0257-7941.18817827621518 [Google Scholar] [CrossRef] [PubMed]
[18]. Peter K, Erik WB, Patients whose GP knows complementary medicine tend to have lower costs and live longerEur J Health Econ 2012 13:769-76.10.1007/s10198-011-0330-221695547 [Google Scholar] [CrossRef] [PubMed]
[19]. Patwardhan B, Health for India: Search for appropriate modelsJ Ayurveda Integr Med 2012 3:173-74.10.4103/0975-9476.10442323326085 [Google Scholar] [CrossRef] [PubMed]
[20]. Shankar D, Health sector reforms for 21st century healthcareJ Ayurveda Integr Med 2015 6:04-09.10.4103/0975-9476.15421425878456 [Google Scholar] [CrossRef] [PubMed]
[21]. Subramanian K, Midha I, Prevalence and perspectives of complementary and alternative medicine among university students in Atlanta, Newcastle upon Tyne, and New DelhiInternational Scholarly Research Notices 2016 :01-09.[cited 2016 November 03 ]. Available from: http://downloads.hindawi.com/journals/isrn/2016/9309534.pdf DOI:http://dx.doi.org/10.1155/2016/930953410.1155/2016/930953427382643 [Google Scholar] [CrossRef] [PubMed]
[22]. Haranath P, Role of pharmacology for integration of modern medicine and AyurvedaIndian J Pharmacol 2015 47:469-71.10.4103/0253-7613.16519126600632 [Google Scholar] [CrossRef] [PubMed]