Introduction
Cariology has traversed through various paths and is now witnessing a paradigm shift towards preventive approach. The evolution of treatment strategy for dental caries can be viewed under three phases namely extractive, restorative and preventive phases [1]. The trajectories of caries experience from childhood to adulthood encompassing the functional, social and financial encumbrance warrants a risk assessment based caries prevention and management [2]. Identifying the risk factors for an individual aids in carrying out a correctly targeted, clinically effective and economically beneficial preventive therapy [3,4]. Numerous approaches have been suggested and implemented towards prevention of dental caries [5-9]. Currently, calcium based phosphate system like CPP-ACP is preferred among non fluoride preventive agents that promote remineralisation [10].
Dairy products are one of the food groups that have been recognised as anticariogenic agents [11,12]. Studies have shown that rinsing the mouth with milk for 30 seconds despite refraining from brushing for three days produces a very negligible drop in pH. This property is specifically attributed to the casein, calcium and phosphate present in milk and milk products. The enamel rapidly absorbs casein fractions and enhances the resistance against acid attacks. These casein products are known to alter the adherence of the Streptococcus mutans which is the predominant microorganism convincingly associated with dental caries [13,14]. Furthermore, micelles of casein modulate the composition of the plaque microflora such that it results in the reduction of their cariogenic potential [15]. The CPP is obtained from the tryptic digestion of casein followed by its aggregation with calcium phosphate [16]. The CPP bonds with nanoclusters of ACP via the phosphoseryl residues present in the former to work as an effective remineralising agent [17].
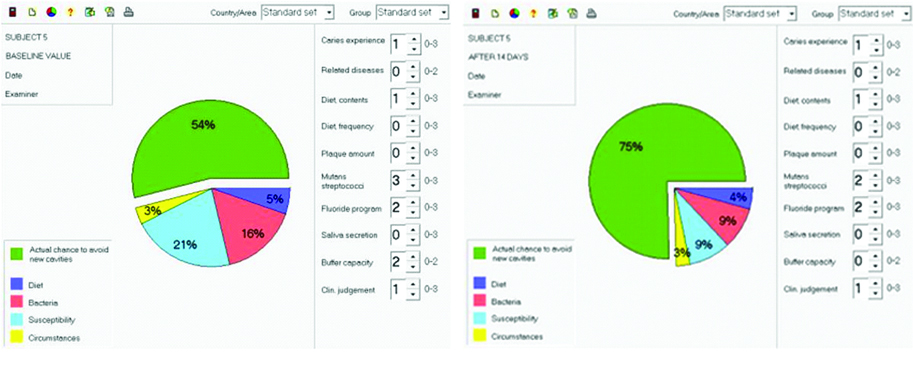
Cariogram is a relatively easy to use and plausibly reliable caries risk assessment tool. It consists of 10 criterions to assess the role of various risk factors for dental caries [18]. This computer based software gives an objective value for each factor and presents the patient’s caries risk profile as a pie chart with five domains [19]. The five sectors of the pie chart include diet, bacteria, susceptibility, chance of avoiding new caries and circumstances. Each sector represents the combined values of the risk factors falling under that domain. The green coloured sector representing the actual chance to avoid new cavities is determined by subtracting the share taken by all the other remaining risk factors on the pie chart. Risk stratification level of an individual is inversely proportional to the percentage of the green sector on the cariogram [20]. Thus, the cariogram provides the benefit of understanding to what extent each risk factor can affect the overall risk profile. This aids in designing a customised risk assessment based preventive therapy for each individual [21].
Exploration of the available literature related to cariogram and CPP-ACP reveals that no study has evaluated CPP-ACP as a caries preventive agent based on cariogram outcome. One study done by Patil B et al., has used the cariogram model to evaluate a prevention program for caries among mentally challenged children [22]. Numerous studies have been done to assess the caries risk using cariogram model; however, there is a scarcity in literature when it comes to using the tool for assessing a caries preventive strategy [23-27]. The present study employs cariogram as an evaluator for CPP-ACP’s anticariogenic action. Thus, the aim of the present study is to assess the changes in cariogram generated risk profiles following the use of CPP-ACP chewing gums.
Materials and Methods
This longitudinal study was conducted at Sri Venkateswara Dental College and Hospital, Tamil Nadu, India, for a period of 14 days in January, 2017. The study was designed as a longitudinal field trial with before and after comparisons to assess the changes in the caries risk profiles following the use of CPP-ACP chewing gums. The protocol was approved by the ethics committee of the Institutional Review Board. The study was registered with the Clinical Trial Registry of India (CTRI/2017/06/008827). This study was initiated as a pilot study and hence, the sample size was not calculated and the duration of the study was kept short. After elaborating the purpose of the study, written informed consent was obtained from all the subjects.
Inclusion and Exclusion Criteria
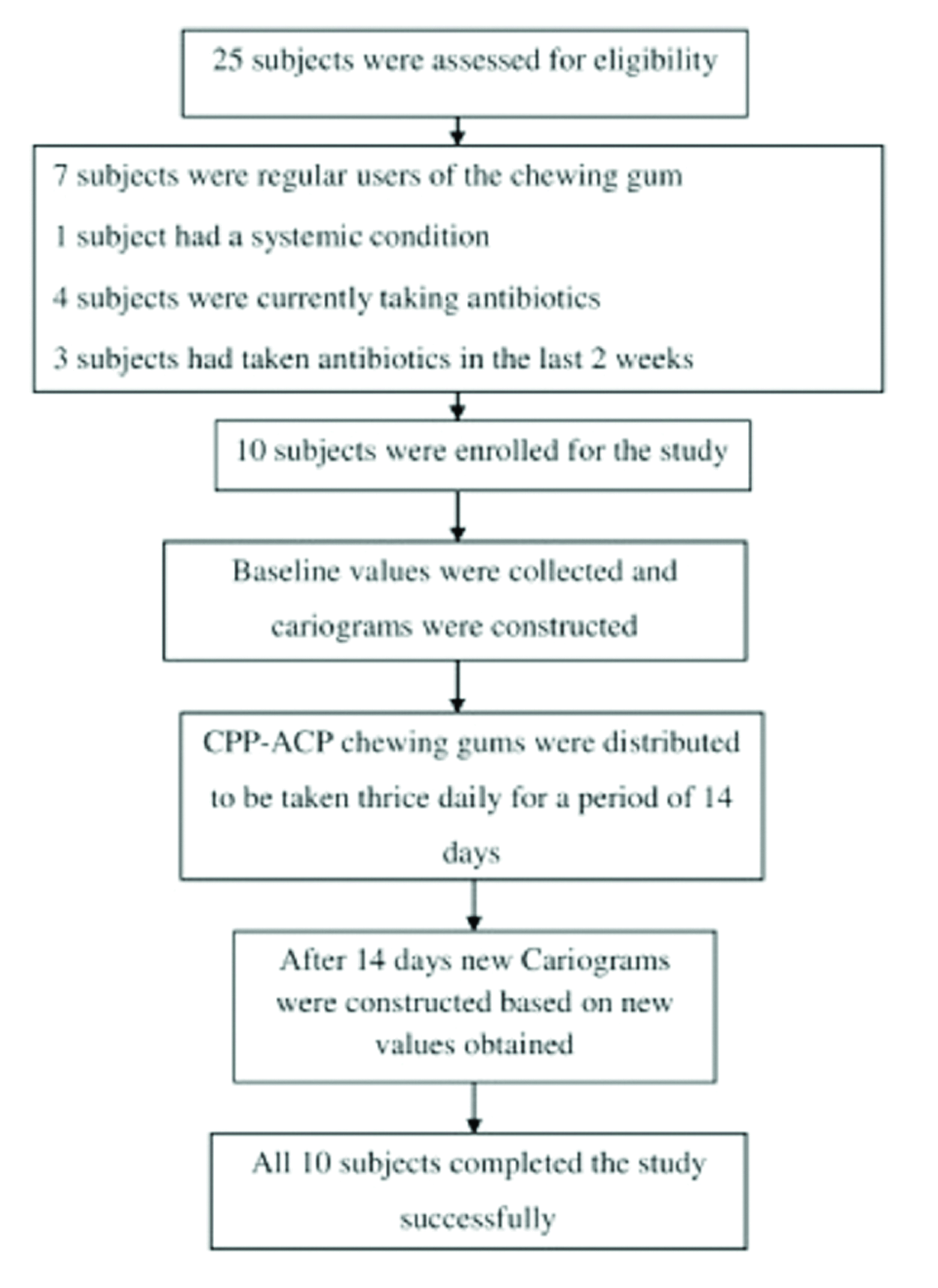
Ten healthy individuals falling in the age group of 18-25 years with no related general diseases were invited to participate in the study. The subjects were recruited from the hostel of Sri Venkateswara Dental College and Hospital and hence, subjects with similar diet pattern and fluoride program were included in the study.
Regular users of chewing gums and those who were allergic to these gums, individuals suffering from systemic illness, individuals under antibiotic cover and those who had taken antibiotics in the last two weeks were excluded from the study. In order to prevent confounding errors due to intake of antibiotics or other factors, every subject was continuously monitored throughout the study period. All subjects were asked to report immediately on the occurrence of any side effects. It was decided that under such circumstances the concerned subject will be excluded from the study.
Proforma for Recording Cariogram Scores
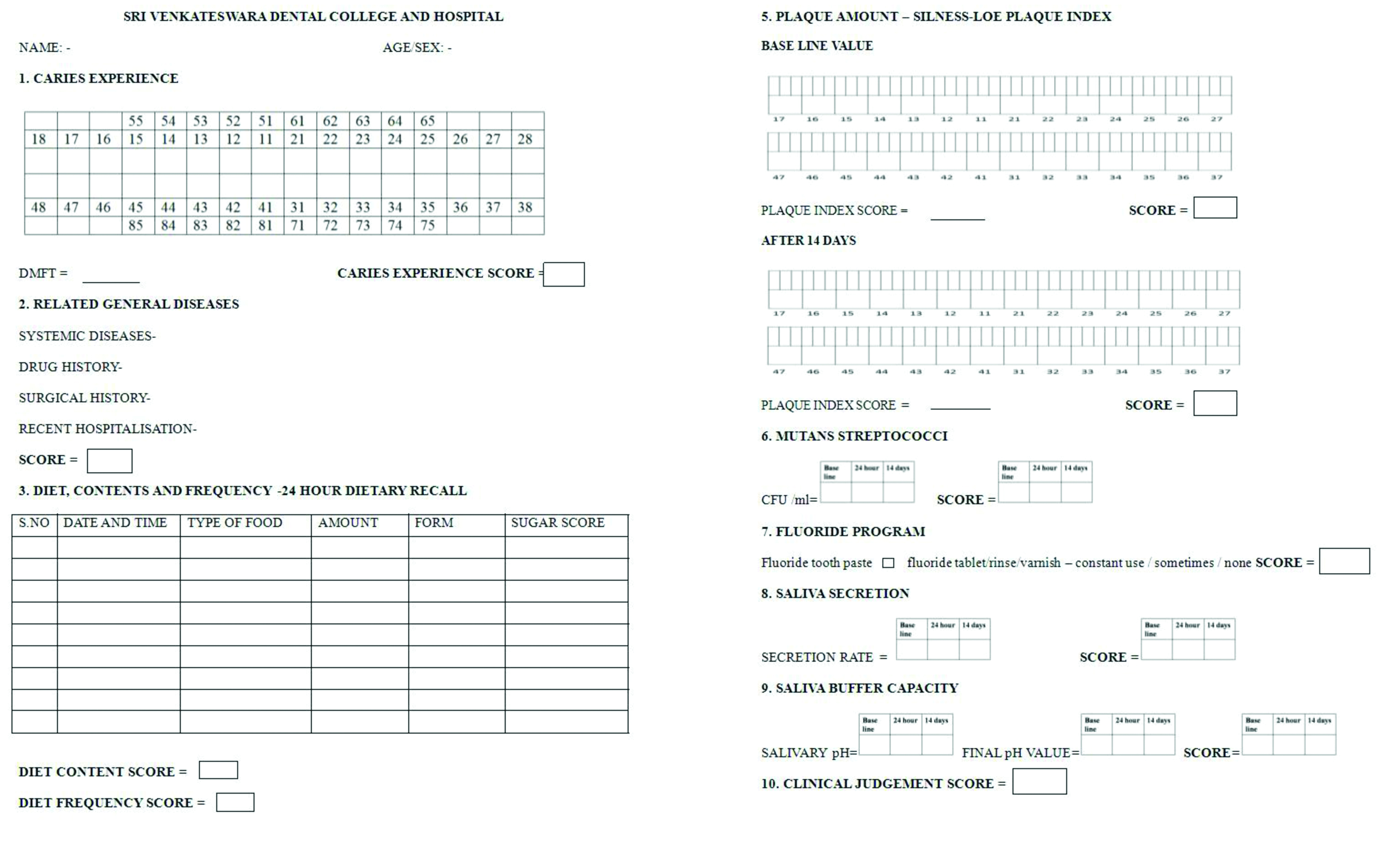
A proforma was designed to document all the information required for constructing the cariogram model [20]. The cariogram consists of 10 criterions spread under four categories each represented by a coloured sector. In addition, there is a fifth sector that is obtained by subtracting all the other four sectors from the pie diagram called the ‘chance to avoid caries’ which is given the green colour. Demographic details and details about fluoride usage, medical history, diet contents and frequency were recorded by taking a detailed case history. Each of these criteria was then allotted scores based on the key provided in the cariogram manual (Bratthall et al., cariogram Manual 2004, Internet version 2.01) [20]. All oral examinations were then carried out by a single investigator.
Recording Caries Status and Plaque Levels
Decayed, Missing, Filled Surface index (DMFS), WHO 1989 criteria was used to record caries experience. A plane mouth mirror and sickle ended probe was used to record the index. The Silness and Loe index was used for assessing the plaque amount. A plane mouth mirror no. #5 was alone used for this index. The DMFS and plaque scores were calculated and the corresponding cariogram scores were then entered in the proforma.
Sample Collection and Salivary Flow Rate
Unstimulated salivary samples were collected in a 5 mL sterile container to evaluate the salivary flow rate, buffer capacity and Streptococcus mutans levels. The subjects were asked to be seated upright in a relaxed position and collect their saliva in the given sterile container. The time taken for them to collect 5 mL of saliva was noted and the salivary flow rate per minute was calculated.
Salivary pH and Buffer Capacity
The pH and buffering capacity were identified using a hand held pH meter with digital display (Digital pH meter, MIFA systems pvt ltd, Ahmadabad, Gujarat, India). Standard pH pellets of pH 4.0 and 7.0 were used for the calibration of the pH sensitive electrode. The test samples were then titrated with 250 μL of lactic acid (pH 3, 1.5 mM). The pH values of the titrated samples were then noted using the same pH meter.
Microbial Analysis
For microbial analysis the salivary samples were diluted and vortex mixed. Aliquots of 0.1 mL from the diluted samples were inoculated on the surface of mitis salivarius agar base (Himedia, Mumbai, Maharashtra, India). The petri plates were then incubated for 48 hours at 37° C with 3% CO2. The colony forming units were counted manually after identifying the organisms based on their colony morphology.
Constructing the Cariogram
All data required for constructing a cariogram were first obtained from all the subjects for baseline. The scores obtained for the 10 criterions based on the key given in the cariogram manual were entered into the cariogram software and the pie chart was constructed. All subjects were given a clinical judgment score of one as there was no disparity between the investigator’s opinion and the cariogram. At the start of the study 10 cariograms were constructed based on baseline values.
Once the baseline cariograms were built, CPP-ACP chewing gums (Recaldent, Nihon Kraft foods limited, Tokyo, Japan) were distributed to the subjects. The subjects were instructed to follow similar oral hygiene measures during the entire study period. They were directed to use the gums thrice daily 15 minutes after each mealtime for a period of 14 days. Again at the end of 14 days, fresh set of data were collected pertaining to salivary analysis for flow rate, buffer capacity and Streptococcus mutans level and the plaque scoring alone. These scores were utilised to construct the new cariogram for all the 10 subjects. Thus, two cariograms were constructed for each subject with the values obtained before and after usage of CPP-ACP chewing gums. The percentage changes in each sector were noted and tabulated using Microsoft Excel 2007 and interpreted.
Results
All subjects completed the study with good compliance and no unpleasant incidents were reported. The [Table/Fig-1] shows proforma used to collect the data for constructing a cariogram. The [Table/Fig-2] shows the cariogram models constructed for one of the study subjects at baseline and after 14 days. The [Table/Fig-3] gives information on excluded subjects from the study and the flow diagram of the longitudinal study. The [Table/Fig-4] shows the gender distribution and mean age of the subjects. The [Table/Fig-5] shows the data collected for the cariogram at baseline and after 14 days. Changes in values are markedly seen only in Streptococcus mutans count and salivary buffer capacity.
Proforma used to collect the data for constructing a cariogram.
Cariogram models constructed for one of the study subjects at baseline and after 14 days.
Information on excluded subjects from the study and the flow diagram of the longitudinal study.
Gender distribution and mean age of the subjects.
| Gender (no. of persons in each gender) | Male | 5 | Total number of subjects=10 |
| Female | 5 |
| Mean age (in years) | Male | 21.2 |
| Female | 21.1 |
Score given for each parameter based on the data collected to construct the cariograms at baseline and after 14 days.
| Subjects | Caries experience | Related general diseases | Diet content | Diet frequency | Plaque amount | Streptococcus mutans | Fluoride program | Saliva secretion | Buffer capacity | Clinical judgment score |
|---|
| Baseline | After 14 days | Baseline | Afrer 14 days | Baseline | After 14 days |
|---|
| 2 | 0 | 0 | 1 | 2 | 0 | 0 | 3 | 3 | 2 | 0 | 3 | 2 | 1 |
| 4 | 1 | 0 | 1 | 1 | 1 | 0 | 3 | 3 | 2 | 0 | 3 | 2 | 1 |
| 6 | 0 | 0 | 1 | 0 | 0 | 0 | 3 | 2 | 2 | 0 | 2 | 1 | 1 |
| 8 | 0 | 0 | 1 | 1 | 0 | 0 | 3 | 2 | 2 | 0 | 3 | 2 | 1 |
| 10 | 1 | 0 | 1 | 0 | 0 | 0 | 3 | 2 | 2 | 0 | 3 | 1 | 1 |
| 12 | 0 | 0 | 1 | 0 | 0 | 0 | 3 | 2 | 2 | 0 | 2 | 1 | 1 |
| 14 | 3 | 0 | 2 | 2 | 0 | 0 | 3 | 2 | 2 | 0 | 3 | 2 | 1 |
| 16 | 0 | 0 | 1 | 1 | 0 | 0 | 3 | 2 | 2 | 0 | 3 | 1 | 1 |
| 18 | 1 | 0 | 2 | 2 | 0 | 0 | 3 | 2 | 2 | 0 | 3 | 2 | 1 |
| 20 | 13 | 0 | 2 | 1 | 1 | 0 | 3 | 3 | 2 | 0 | 3 | 2 | 1 |
The [Table/Fig-6] shows the change in percentage of green sector of all the subjects before and after the intervention. Results of the field trial show an increase in the percentage of green sector after 14 days in all the subjects. The central tendency value of the green sector has improved from 53.9% to 67.1% after the use of CPP- ACP chewing gums. This indicates that CPP-ACP is an effective caries protective agent. The magnitude of difference in green sector percentage among the subjects ranges from 4% to 24% with a mean value of 13.2%.
Change in percentage of green sector before and after the use of CPP-ACP chewing gum.
| Subject | Green sector (%) | Difference (%) |
|---|
| At baseline | After 14 days |
|---|
| 1 | 69 | 73 | 4 |
| 2 | 48 | 57 | 9 |
| 3 | 81 | 90 | 9 |
| 4 | 75 | 85 | 10 |
| 5 | 54 | 75 | 21 |
| 6 | 81 | 90 | 9 |
| 7 | 21 | 45 | 24 |
| 8 | 75 | 88 | 13 |
| 9 | 25 | 49 | 24 |
| 10 | 10 | 19 | 9 |
The [Table/Fig-7] shows the change in percentage of the four sectors on comparing the pre and post intervention cariogram models. A mean difference of 6.2% is seen under the light blue sector. A dip in the percentage of light blue sector from 18.5% to 13.3% is seen. This sector shows the maximum range of difference when compared to the other three sectors indicating that CPP-ACP improves the salivary flow rate and buffering capacity. Light blue sector is subsequently followed by the red sector with a mean difference value of 4.6% signifying the antimicrobial action and plaque reduction potential of CPP-ACP. The yellow sector and dark blue sector show insignificant alterations from baseline values.
Change in percentage of other four sectors before and after the use of CPP-ACP chewing gums.
| Subject | Light blue sector (%) | Difference (%) | Red sector (%) | Difference (%) | Dark blue sector (%) | Difference (%) | Yellow sector (%) | Diffe-rence (%) |
|---|
| At baseline | After 14 days | At baseline | After 14 days | At baseline | After 14 days | At baseline | After 14 days |
|---|
| 1 | 12 | 9 | 3 | 9 | 9 | 0 | 9 | 9 | 0 | 1 | 0 | 1 |
| 2 | 19 | 15 | 4 | 19 | 15 | 4 | 10 | 10 | 0 | 3 | 3 | 0 |
| 3 | 8 | 4 | 4 | 8 | 4 | 4 | 3 | 2 | 1 | 0 | 0 | 0 |
| 4 | 10 | 6 | 4 | 8 | 4 | 4 | 5 | 4 | 1 | 2 | 1 | 1 |
| 5 | 21 | 9 | 12 | 16 | 9 | 7 | 5 | 4 | 1 | 3 | 3 | 0 |
| 6 | 8 | 4 | 4 | 8 | 4 | 4 | 3 | 2 | 1 | 0 | 0 | 0 |
| 7 | 24 | 15 | 9 | 18 | 10 | 8 | 24 | 20 | 4 | 12 | 10 | 2 |
| 8 | 10 | 4 | 6 | 8 | 4 | 4 | 5 | 4 | 1 | 2 | 0 | 2 |
| 9 | 26 | 16 | 10 | 19 | 11 | 8 | 26 | 21 | 5 | 4 | 3 | 1 |
| 10 | 57 | 51 | 6 | 15 | 12 | 3 | 11 | 12 | -1 | 7 | 8 | -1 |
Discussion
Primary prevention is a vital concept in comprehensive dental care. Prevention of dental caries not only improves oral health but also the systemic health and the quality of life of an individual [28]. Before starting with a preventive program, the first imperative step is to assess the risk of the individual rather than proceeding with the routine prevention therapy. Assessing the risk factors will provide information for generating preventive strategies that result in successful work division and economic effectiveness [29]. Four models are available to assess the caries risk which includes Cariogram, Caries Management By Risk Assessment (CAMBRA), American Dental Association (ADA), and American Academy of Paediatric Dentistry (AAPD). Out of these systems, cariogram is found to be quick, inexpensive and acceptable tool [30]. Cariogram is an expedite tool that acts as both a prediction model and risk model for dental caries [21]. Apart from prophesying occurrence of dental caries, this tool can be used to educate and motivate the patient. The simple pie chart representation of the risk profile is easily appreciated by the patient. The cariogram can also be used to prescribe targeted preventive programs [18]. An expansion of the green area in the pie chart proclaims the success of the preventive intervention [20]. Also, an increase in green sector means a decrease in the percentage of another sector or combination of other sectors. This further aids in interpreting the action of the intervention on the risk factor. Hence, in this study the changes in the cariogram outcome following the use of CPP-ACP chewing gums have been assessed.
The CPP-ACP compounds have remarkable potential to act as caries preventive agents [31]. The compound can be delivered in the form of chewing gums, tooth pastes, topical applications, etc [10]. CPP-ACP chewing gums are sugar free and also stimulate salivary flow. Both these factors summated with the benefits of calcium phosphate system in CPP-ACP chewing gums give it the credence of being a caries preventive agent [32]. The amount of CPP-ACP by weight present in the chewing gum is 10.0 mg. Yengopal V and Mickenautsch S, in this systematic review and meta analysis has concluded that a significantly higher level of remineralisation effect is observed after exposure to 10.0 mg of CPP-ACP [33]. Hence, in the present study CPP-ACP was used in the form of chewing gums. The time interval of 5-20 minutes after each meal is when the pH plummets rapidly. In order to offset this pH drop effectively, the gums should be chewed within 20 minutes following each meal [34,35]. Hence, in this study the subjects were asked to follow the same.
Multiple studies have suggested CPP-ACP as a caries preventive agent [36-38]. This statement is in congruence with the result of the present study. The improvement in the caries risk profile after 14 days as indicated by the increase in green sector confirms the anticariogenic effectiveness of CPP-ACP. This seeming increase in the percentage of green sector is because of the actual decrease in percentage of the other sectors. Light blue sector seems to be the most altered sector followed by the red sector while the dark blue and yellow sectors showed very negligible changes.
The light blue sector (represents susceptibility) is based on a combination of fluoride program, salivary buffer and flow rate [20]. Since, the subjects were instructed to follow similar oral hygiene measures the alteration in the susceptibility sector can be attributed to the change in salivary characteristics. Studies done by Harris NO et al., and Iijima Y et al., have shown that the use of chewing gums for 20 minutes triples the salivary flow rate [39,40]. Furthermore studies have shown that CPP-ACP can enhance the buffering ability of saliva with the calcium and phosphate ion system [33]. Karlinsey RL and Mackey AC stated that a single CPP molecule can accommodate up to 25 calcium ions, 15 phosphate ions and five fluoride ions [41]. The CPP-ACP gets incorporated into the plaque and releases its cargo of ions to maintain a supersaturated state with respect to enamel. As the pH declines the bonding between CPP and ACP weakens thereby creating a pool of free calcium and phosphate ions which enhances remineralisation at the crucial time suppressing the demineralisation due to the low pH [42].
The red sector representing bacteria is calculated from weighted values of amount of plaque and Streptococcus mutans [20]. The change seen in the red sector is due to the antibacterial action of CPP-ACP on Streptococcus mutans. CPP-ACP destroys the calcium bridges among the bacteria and between bacteria and pellicle by competitive uptake of calcium in the plaque [43,44]. Rose RK, in an in vivo study concluded that CPP-ACP binds to calcium with an affinity which is twice as that of bacterial cells to calcium [44]. The Silness and Loe index used for plaque assessment in the cariogram simply objectifies the unmitigated presence of plaque. Thus, the quantity of plaque is taken into consideration and not the quality. Moreover, anticalculus action of CPP-ACP has been mentioned in the literatures but there is no evidence stating the reduction in plaque amounts due to CPP-ACP action [43]. The effect of CPP-ACP on plaque reduction remains questionable as CPP-ACP is known to reduce cariogenicity of the plaque by diminishing the adherence of Streptococcus mutans and Streptococus sobrinus to plaque biofilm [45].
Circumstances (yellow sector) comprises of past caries experience, related general diseases [20]. Results of the study show that changes in this sector is almost nil as dental caries take time periods longer than 14 days to occur. Similarly, the systemic health conditions do not sway morbidly in a short duration and hence no significant alteration is seen in yellow sector. Diet content and frequency constitute the diet domain (dark blue) which also shows negligible changes as no change in diet pattern was advised for the subjects to follow [20]. A visible increase is seen in the green sector within a span of 14 days due to the use of CPP-ACP, however, long term clinical trials with a bigger sample size should be done to declare the validity of the preventive intervention.
Limitation
The short time duration and fewer subjects stand as a limitation for the present study.
Conclusion
Within the limitations of the present study, it can be concluded that the caries risk profile of an individual improves after the use of CPP-ACP chewing gums. The idea of implementing multiple preventive strategies for the same individual based on their risk profile should be taken into consideration in the future. This might help in pushing the patients to low risk categories. Risk assessment is woven deeply into the fabric of preventive dentistry. If prevention is the new paradigm then risk assessment tool should be a mandatory instrument in the dentists’ armamentarium.
Risk based prevention should be preferred to routine prevention as it will be more rationale and specific for each individual. Building a cariogram for each subject will allow the clinician to assess the risk based needs for dental caries while simultaneously assessing the anticariogenic effectiveness of the preventive intervention.
[1]. Pitts NB, Are we ready to move from operative to non-operative/ preventive[1] treatment of dental caries in clinical practiceCaries Res 2004 38(3):294-304.10.1159/00007776915153703 [Google Scholar] [CrossRef] [PubMed]
[2]. Bowen WH, Tabak LA, Adaptations in dental plaque. In: cariology for the nineties. RochesterUniversity of Rochester Press 1993 :461-16. [Google Scholar]
[3]. Holst A, Martensson I, Laurin M, Identification of caries risk children and prevention of caries in preschool childrenSwed Dent J 1997 21(5):185-91. [Google Scholar]
[4]. Wendt LK, Carlsson E, Hallonsten AL, Birkhed D, Early dental caries risk assessment and prevention in preschool children: evaluation of a new strategy for dental care in a field studyActa Odontol Scand 2001 59(5):261-66.10.1080/00016350175054110111680643 [Google Scholar] [CrossRef] [PubMed]
[5]. Sicca C, Bobbio E, Quartuccio N, Nicolò G, Cistaro A, Prevention of dental caries: a review of effective treatmentsJ Clin Exp Dent 2016 8(5):604-10.10.4317/jced.5289027957278 [Google Scholar] [CrossRef] [PubMed]
[6]. Lee Y, Diagnosis and prevention strategies for dental cariesJ Lifestyle Med 2013 3(2):107-09. [Google Scholar]
[7]. Featherstone JD, The science and practice of caries preventionJ Am Dent Assoc 2000 131(7):887-99.10.14219/jada.archive.2000.030710916327 [Google Scholar] [CrossRef] [PubMed]
[8]. Chen F, Wang D, Novel technologies for the prevention and treatment of dental caries: a patent surveyExpert Opin Ther Pat 2010 20(6):681-94.10.1517/1354377100372049120230309 [Google Scholar] [CrossRef] [PubMed]
[9]. Rugg Gunn A, Dental caries: strategies to control this preventable diseaseActa Medi Acad 2013 42(2):117-30.10.5644/ama2006-124.8024308392 [Google Scholar] [CrossRef] [PubMed]
[10]. Divyapriya GK, Yavagal PC, Veeresh PJ, Casein phosphopeptide-amorphous calcium phosphate in dentistry: an updateInt J Oral Health Sci 2016 6(11):18-25.10.4103/2231-6027.186660 [Google Scholar] [CrossRef]
[11]. Reynolds EC, Johnson IH, Effect of milk on caries incidence and bacterial composition of dental plaque in ratArch Oral Biol 1981 26(4):445-51.10.1016/0003-9969(81)90042-X [Google Scholar] [CrossRef]
[12]. Rosen S, Min DB, Harper DS, Harper WJ, Beck EX, Beck FM, Effect of cheese with and without sucrose on dental caries and recovery of Streptococcus mutans in ratsJ Dent Res 1984 63:894-96.10.1177/002203458406300616016588074 [Google Scholar] [CrossRef] [PubMed]
[13]. Scholz-Arens KE, Schrezenmeir J, Effects of bioactive substances in milk on mineral and trace element metabolism with specia reference to casein phosphopeptidesBr J Nutr 2000 84:147-53.10.1017/S000711450000237311242459 [Google Scholar] [CrossRef] [PubMed]
[14]. Vacca-Smith AM, Van Wuy chheyse BC, Jabak LA, Bowen WH, The effect of milk and casein proteins on the adherence of Streptococcus mutans to saliva coated hydroxyapatiteArch Oral Biol 1994 39(12):1063-69.10.1016/0003-9969(94)90059-0 [Google Scholar] [CrossRef]
[15]. Guggenheim B, Schmidt R, Aeschlimann JM, Berrocal R, Neeser JR, Powdered milk miscellar casein prevents oral colonization by S.Sobrinus and dental caries in rats: a basis for caries protective effect of dairy products.Caries Res 1999 33(3):446-54.10.1159/00001655010529530 [Google Scholar] [CrossRef] [PubMed]
[16]. Reynolds EC, Calcium phosphate-based remineralization systems: scientific evidenceAust Dent J 2008 53(3):268-73.10.1111/j.1834-7819.2008.00061.x18782374 [Google Scholar] [CrossRef] [PubMed]
[17]. Reynolds EC, Remineralization of enamel subsurface lesions by casein phosphopeptide stabilized calcium phosphate solutionsJ Dent Res 1997 76(9):1587-95.10.1177/002203459707600911019294493 [Google Scholar] [CrossRef] [PubMed]
[18]. Bratthall D, Hånsel Petersson G. Cariogram-a multifactorial risk assessment model for a multifactorial diseaseCommunity Dent Oral Epidemiol 2005 33(4):256-64.10.1111/j.1600-0528.2005.00233.x16008632 [Google Scholar] [CrossRef] [PubMed]
[19]. Hansel G, Twetman S, Bratthall D, Evaluation of a computer programme for caries risk assessment in school childrenCaries Res 2002 36(5):327-40.10.1159/00006596312399693 [Google Scholar] [CrossRef] [PubMed]
[20]. Bratthall D, Petersson GH, Stjernswård JR, Stockholm, Sweden: Fğrlagshuset Gothia 2004 Cariogram manual, Internet Version, 2.01. https://www.mah.se/upload/FAKULTETER/OD/cariogram%20program%20caries/cariogmanual201net.pdf Accessed date on 01.02.2018 [Google Scholar]
[21]. Anup N, Vishnanil P, Cariogram-a multi-factorial risk assessment software for risk prediction of dental cariesInt J Sci Stud 2014 1(4):58-62. [Google Scholar]
[22]. Patil YB, Hegde shetiya S, Kakodkar PV, Shirahatti R, Evaluation of a preventive program based on caries risk among mentally challenged children using the cariogram modelCommunity Dent Health 2011 18(4):286-91. [Google Scholar]
[23]. Celik EU, Gokay N, Ates M, Efficiency of caries risk assessment in young adults using cariogramEur J Dent 2012 6(3):270-79.10.1055/s-0039-169896122904655 [Google Scholar] [CrossRef] [PubMed]
[24]. Kemparaj U, Chavan S, Shetty NL, Caries risk assessment among school children in Davangere city using cariogramInt J Prev Med. 2014 5(5):664-71. [Google Scholar]
[25]. Petersson GH, Isberg P, Twetman S, Caries risk assessment in school children using a reduced cariogram model without saliva testsBMC Oral Health 2010 10(5):02-06.10.1186/1472-6831-10-520403163 [Google Scholar] [CrossRef] [PubMed]
[26]. Petersson GH, Twetman S, Caries risk assessment in young adults: a 3 year validation of the Cariogram modelBMC Oral Health 2015 17:2-5.10.1186/1472-6831-15-1725627618 [Google Scholar] [CrossRef] [PubMed]
[27]. Hebbal ML, Ankola A, Metgud S, Caries risk profile of 12-year-old school children in an Indian city using cariogramMed Oral Patol Oral Cir Bucal 2012 17(6):1054-61.10.4317/medoral.1788022926464 [Google Scholar] [CrossRef] [PubMed]
[28]. American Dental Association. Electronic oral health risk assessment toolsADA SCDI. White Paper No.1074 2013 [Google Scholar]
[29]. Pienihåkkinen K, Jokela J, Alanen P, Risk based early prevention in comparison with routine prevention of dental caries: a 7year followup of a controlled clinical trial; clinical and economic aspects.BMC Oral Health 2005 2(1)10.1186/1472-6831-5-215784155 [Google Scholar] [CrossRef] [PubMed]
[30]. Tellez M, Gomez J, Pretty I, Ellwood R, Ismail AI, Evidence on existing caries risk assessment systems: are they predictive of future cariesCommunity Dent Oral Epidemiol 2013 41(1):67-78.10.1111/cdoe.1200322978796 [Google Scholar] [CrossRef] [PubMed]
[31]. Reema SD, Lahiri PK, Roy SS, The review of casein phosphopeptidesamorphous calcium phosphateChin J Dent Res 2014 17(1):07-14. [Google Scholar]
[32]. Chaitanya KG, Prabhakar AR, Saraswathi V, Shivani R, Blow off caries with bubble gumIndian J Med Res Pharmaceut Sci 2016 3(11):18-27. [Google Scholar]
[33]. Yengopal V, Mickenautsch S, Caries preventive effect of casein phosphopeptideamorphous calcium phosphate (CPP-ACP): a meta-analysisActa Odontol Scand. 2009 67(6):321-32.10.1080/0001635090316056319701818 [Google Scholar] [CrossRef] [PubMed]
[34]. Stephan RM, Intraoral hydrogen ion concentrations associated with dental caries activityJ Dent Res 1994 23(4):257-66.10.1177/00220345440230040401 [Google Scholar] [CrossRef]
[35]. Muthu MS, Sivakumar N, Pediatric dentistry: principles and practice 1999 2nd EditionIndiaElsevier. A division of Reed Elsevier India private limited:588 [Google Scholar]
[36]. Reynolds EC, Cain CJ, Webber FL, Black CJ, Riley PF, Johnson IH, Anticariogenicity of calcium phosphate complexes of tryptic calcium phosphopeptides in the ratJ Dent Res 1995 74(6):1272-79.10.1177/002203459507400606017629336 [Google Scholar] [CrossRef] [PubMed]
[37]. Reynolds EC, Black CL, Webber FL, Advances in enamel remineralization anticariogenic casein phosphopeptide- Amorphous calcium phosphateJ Clin Dent 1999 10:86-88. [Google Scholar] [CrossRef]
[38]. Walker G, Cai F, Shen P, Reynolds C, Ward B, Fone C, Increased remineralization of tooth enamel by milk containing added casein phosphopeptideamorphous calcium phosphateJ Dairy Res 2006 73(1):74-78.10.1017/S002202990500148216433964 [Google Scholar] [CrossRef] [PubMed]
[39]. Harris NO, Godoyf G, Nathe CN, Primary preventive dentistry 2004 6th EditionNew JerseyPrentice Hall:842-20. [Google Scholar]
[40]. Iijima Y, Cai F, Shen P, Reynolds G, Reynolds C, Acid resistance of enamel subsurface lesions remineralized by sugar free chewing gum containing casein phosphopeptide amorphous calcium phosphateCaries Res 2004 38(6):551-56.10.1159/00008058515528910 [Google Scholar] [CrossRef] [PubMed]
[41]. Karlinsey RL, Mackey AC, Solid state preparation and dental application of an organically modified calcium phosphateJ Master Sci 2009 44(1):346-49.10.1007/s10853-008-3068-1 [Google Scholar] [CrossRef]
[42]. Reynolds EC, Cai F, Shen P, Walker CD, Retention of plaque and remineralization of enamel lesions by various forms of calcium in a mouth rinse or sugar free chewing gumJ Dent Res 2002 82(3):206-11.10.1177/15440591030820031112598550 [Google Scholar] [CrossRef] [PubMed]
[43]. Rose RK, Effects of anti-cariogenic casein phosphopeptides on calcium diffusion in streptococcal model dental plaquesArch Oral Biol 2000 45(7):569-75.10.1016/S0003-9969(00)00017-0 [Google Scholar] [CrossRef]
[44]. Rose RK, Binding characteristics of Streptococcus mutans for calcium and casein phosphopeptidesCaries Res 2000 34(5):427-31.10.1159/00001661811014910 [Google Scholar] [CrossRef] [PubMed]
[45]. Pukallus ML, Plonka KA, Holcombe TF, Barnett AG, Walsh LJ, Seow WK, A randomized controlled trial of a 10 percent CPP-ACP cream to reduce mutans streptococci colonizationPediatr Dent 2013 35(8):550-55. [Google Scholar]