Ectopic Ureter Causing Hydrometra in a Case of Cervical Dysgenesis with Vaginal Agenesis
Vineet V Mishra1, Ruchika A Verneker2, Priyankur Roy3, Sumesh Choudhary4, Shaheen A Hokabaj5
1 Professor and Head, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Center, Ahmedabad, Gujarat, India.
2 Clinical Fellow, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Center, Ahmedabad, Gujarat, India.
3 Clinical Fellow, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Center, Ahmedabad, Gujarat, India.
4 Assistant Professor, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Center, Ahmedabad, Gujarat, India.
5 Clinical Fellow, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Center, Ahmedabad, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vineet V Mishra, Professor and Head, Department of Obstetrics and Gynaecology, IKDRC-ITS, Asarwa, Ahmedabad-380016, Gujarat, India.
E-mail: vineet.mishra.ikdrc@gmail.com
Cervical agenesis or dysgenesis is the defect of vertical fusion of the mullerian duct and the urogenital sinus. The reported incidence is 0.01% in general population. Up to 53% of patients with mullerian agenesis have concomitant congenital malformations and hence these patients should be thoroughly evaluated for the same. We report a case of cervical dysgenesis with ectopically located right ureter in the uterus. This patient had cervical obstruction with absent vagina. Conservative surgical approach was adopted. Cervical reconstruction with cervicovaginal anastomosis with the neovagina was done. The ectopically located ureter was cut and reimplanted into the bladder. Hence in patients with cervical agenesis or dysgenesis radicle approach like hysterectomy should be adopted only in case of failure of conservative surgery. Thus giving the patient a chance for healthy reproductive life and prevent premature ovarian failure.
Cervicovaginal anastomosis, Neocervix, Neovagina
Case Report
The present case report is about a 10-year-old prepubertal girl, deaf and dumb since birth with diminished vision. According to the mother of the child she had on and off noncyclical abdominal pain for last six months. She was investigated for the same at a private hospital. Computed tomography scan with contrast showed distended uterus cervix and vagina with possibility of ectopic ureteral opening into the vagina on right side. She was referred at our institute, with a diagnosis of hematocolpos with query right ectopic ureter.
On local examination secondary sexual characteristics showed thelarche Grade II and pubarche Grade II. Genital examination showed blind vagina. Per rectal examination revealed a cystic bulge pressing on the rectum. Case was discussed with urologist and a multidisciplinary approach was adopted. Investigation showed haemoglobin 10.4 gm/dL, serum creatinine 0.47 mg/dL, urine routine microscopy was normal and other blood investigations were within normal limits. A multidisciplinary approach was adopted along with an urologist and plastic surgeon, vaginoplasty along with neocervix creation with ureteric reimplantation was planned.
Patient and her parents were duly counselled regarding the surgical method and possible complication. Mcindoe vaginoplasty was done for vaginal agenesis [Table/Fig-1].
Vaginal space dissection with median raphe and after cutting median raphe.

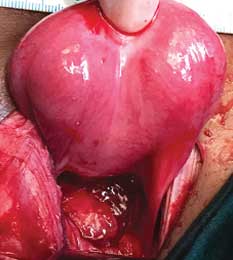
Laparotomy was performed. Intraoperative finding revealed right side ectopic ureter opening into the cervix posteriorly [Table/Fig-2]. Uterus was enlarged with a second bulge of the partially canalised cervix giving a dumble shaped appearance [Table/Fig-3]. Thus, the diagnosis of cervical dysgenesis with obstructed cervix along with vaginal agenesis and ectopic right ureter was confirmed.
Right side ectopic ureter opening into the cervix posteriorly after reflecting retroperitoneum.

Enlarged uterus with a second bulge of the partially canalised cervix giving dumble shaped appearance.
Stab incision was given on the anterior wall of the uterus and clear urine was drained out. Hysteroscopy was performed through the incision, which showed cervical dysgenesis with cervical outlet obstruction. A cruciate incision was given on the most dependent part of the cervix. The most distal end of the vaginal dissection was identified and an incision was given over it. A chest tube drain was cut and passed through the uterine incision into the vaginal space. Cruciate incision was sutured with the vagina to form the cervicovaginal anastomosis. The tube was fixed to the posterior wall of uterus. Mould with the graft was placed in the vagina and fixed. This was followed by uretetic reimplantation into the bladder. Intraoperative double J stenting was done.
She was kept nil per mouth postoperatively for eight days. On postoperative day 8, mould change was done under short general anaesthesia. Vaginoscopy with 2.9 mm hysteroscope showed the graft was well taken up. She was discharged on postoperative day 10, with advice to change the mould twice daily. The chest tube that is fixed intrauterine was kept in situ for minimum eight months. There was fibrosis of cervical tissue around the tube, forming neocervix communicating with the neovagina. She is now on regular follow-up with last follow up three months back and has adequate vaginal space with normal renal function.
Discussion
The congenital vaginal agenesis has a prevalence rate of 1 in 4000-5000 live births while the incidence of cervical agenesis is 0.01% in general population. It represents about 3% of all uterine anomalies [1].
In this case, the patient had cervical dysgenesis wherein the cervical body was intact with obstruction of the cervical os with ectopically opening ureter into the uterus. This gave the uterus dumble shaped appearance. There was associated complete vaginal agenesis. No case with similar presentation has been reported in the literature, where ectopic ureter draining into the uterus is associated with cervical and vaginal agenesis.
The urogenital system in females develops from the mullerian duct and wolffian duct. The mullerian ducts originate at six weeks and fuses with the sinovaginal bulb to form the uterus cervix and the vagina. Thus upper 2/3rd of vagina is formed from mullerian duct and lower 1/3rd by urogenital sinus. By fifth week the uretric bud branch from the posterior end of the wolffian duct at the level of the first sacral segment [2]. An appropriate ureteric bud out growth and patterning is necessary as urinary tract malformation is the most common associated congenital malformation.
These patients need to be evaluated thoroughly before the plan of management is decided. Magnetic Resonance Imaging (MRI) is the gold standard for diagnosis; however basic transabdominal or translabial ultrasound should be done. Up to 53% of patients with mullerian agenesis have concomitant congenital malformations and hence these patients should be thoroughly evaluated for the same [3]. Thorough psychosocial counselling should be done and the secondary sexual characteristics should be evaluated. Patient should be educated regarding the condition and the mode of management. Fertility options like surrogacy should be explained. However, there are cases of live births in patients of cervical agenesis [4].
For decades cervical agenesis would ultimately require hysterectomy. However, literature has shown that there is nearly a two-fold increased risk for ovarian failure post hysterectomy as compared to women with intact uteri [5]. Hence, we now have a novel technique wherein the cervical opening is created and the cervix is anastomosed with the neovagina. Thus hysterectomy can be avoided giving the patient a chance for a better life and reproduction. However, the risk of restenosis of the cervical canal on long-term follow-up cannot be ruled out thus warranting repeat surgery. Thus hysterectomy remains as a last resort in case of repeated episodes of endometriosis, haematometra, and recurrent obstruction [6]. To avoid this complication in present case we kept a tube in the uterine cavity passing through the cervical opening into the vagina. This tube was placed in situ till a fibrous tubular structure was formed which epithelised to form a neocervical canal. In a long term follow-up study of 23 patients of abbe Wharton McIndoe vaginoplasty most of the patients had satisfactory sexual activity with good mucosal sensitivity [7]. It is recommended that vaginoplasty should be deferred till the woman is physically and psychologicaly mature. Thus adolescence is the ideal time for vaginoplasty. However, the timing should be individualised based on the patient’s symptoms and presentation.
In present case, patient had hydrometra, with ectopic ureter opening into the cervix. Patient was symptomatic with abdominal pain and distended uterus. Hence, the decision for surgery was taken at an early age. Ureteric reimplantation was done into the bladder by ureteroneocystotomy. Mcindoe vaginoplasty was done using split skin graft. However, the success of the surgery depends on how efficiently patient keeps the mould in situ.
Conclusion
Preservation of the uterus gives the woman a chance for a better reproductive and a healthy life both psychologically and physically. Hence, conservative approach with neocervix creation must be adopted initially. However, in case of repeated failure of surgery hysterectomy should be the last resort in these patients.
[1]. Helmy YA, Cervical agenesis with a functioning uterus: Successful surgical treatment by Foley’s catheter stent: A case reportMiddle East Fertility Society Journal 2017 22(1):67-69.10.1016/j.mefs.2016.07.001 [Google Scholar] [CrossRef]
[2]. Jacob M, Development, Differentiation and Derivatives of the Wolffian and Müllerian DuctsThe Human Embryo. Germany: Intech open; March 2012 10.5772/34351 [Google Scholar] [CrossRef]
[3]. American college of obstetrics and gynaecologist. Committee on adolescent health care. Mullerian agenesis: Diagnosis, management, and treatment. Committee opinion, number 728. January 2018 (ACOG) [Google Scholar]
[4]. Acién P, Acién MI, Quereda F, Santoyo T, Cervicovaginal agenesis: spontaneous gestation at term after previous reimplantation of the uterine corpus in a neovagina: Case reportHum Reprod 2008 23(3):548-53.10.1093/humrep/dem42018192672 [Google Scholar] [CrossRef] [PubMed]
[5]. MoormanG P, Myers ER, Schildkraut JM, Iversen ES, Wang F, Warren N, Effect of hysterectomy with ovarian preservation on ovarian functionObstetrics and Gynecology 2011 118(6):1271-79.10.1097/AOG.0b013e318236fd1222067716 [Google Scholar] [CrossRef] [PubMed]
[6]. Mishra V, Saini SR, Nanda S, Choudhary S, Roy P, Singh T, Uterine conserving surgery in a case of cervicovaginal agenesis with unicornuate uterusJournal of Human Reproductive Sciences 2016 9(4):267-70.10.4103/0974-1208.19769628216917 [Google Scholar] [CrossRef] [PubMed]
[7]. Bastu E, Akhan SE, Mutlu MF, Nehir A, Yumru H, Hocaoglu E, Treatment of vaginal agenesis using a modified McIndoe technique: Long-term follow-up of 23 patients and a literature reviewCan J Plast Surg 2012 20(4):241-44.10.1177/22925503120200041624294018 [Google Scholar] [CrossRef] [PubMed]