Introduction
Dysphagia is a common symptom seen in patients in ENT OPD. Gastro-oesophageal reflux, foreign body, mass lesions being the known common causes. Cervical spondylosis with large osteophytes is one of the causes of dysphagia, which can be easily diagnosed even with limited facilities available but it is less discussed in younger age group.
Aim
To evaluate the clinical importance and significance of cervical osteophytes as a cause of dysphagia.
Materials and Methods
Seventy patients of either sex, between the age group of 25-59 years, with dysphagia were evaluated with complete history and clinical examination followed by upper gastrointestinal endoscopy. All common causes of dysphagia were ruled out. Patients were evaluated with a digital X-ray of cervical spine in lateral view. The results were analysed statistically using chi-square test and Fischer’s-exact test.
Results
Out of 70 patients evaluated, 40 (57.1%) were female patients and 30 (42.9%) male patients. About 21 (30%) patients were found to have cervical spine osteophytes.
Conclusion
After ruling out common causes, anterior cervical osteophytes should be remembered as one of the causes of dysphagia by the otorhinolaryngologists for effective management.
Introduction
Dysphagia is one of the common symptoms seen in patients in ENT OPD, manifesting as difficulty in swallowing [1]. Gastro-oesophageal reflux disease, infections, neoplastic growths, strictures, foreign body, neurological causes like stroke, myasthenia gravis are some of the causes of dysphagia. Cervical spondylosis with osteophyte/osteophytes is one of the causes of dysphagia which usually goes unnoticed by otorhinolaryngologists. Dysphagia caused by osteophytes was first described by Mosher HP, in 1926 [2].
Anterior cervical osteophytes may be asymptomatic in 20-30% of the population [1,3]. Even though osteophyte is asymptomatic most of the times, probably due to mechanical compressions, leading to inflammation and oedema, multiple symptoms may manifest [4]. This can be easily diagnosed even with limited facilities available, and hence should be considered to be included in the diagnostic workup.
Cervical spine changes are common with growing age and anterior cervical osteophytes is a frequent finding in elderly; however, osteophyte is usually not considered as a cause for dysphagia in relatively younger age group, so our study mainly concentrates on this group of patients. The aim of our study was to evaluate the clinical importance and significance of cervical osteophytes as a cause of dysphagia.
Materials and Methods
A prospective descriptive study was conducted on 70 patients with complaints of dysphagia attending ENT OPD at Bapuji hospital and Chigateri district hospital, teaching hospitals attached to JJM Medical college, Davangere, Karnataka, India. The study was conducted during the period of January 2017 to December 2017 after obtaining Ethical Committee clearance.
Informed and written consent was taken from all the 70 patients who fulfilled the inclusion and exclusion criteria and were willing to participate in the study.
Patients aged 25 to 59 years, of either sex, with dysphagia after ruling out intraluminal causes were included. While, patients with central and peripheral neurological causes were excluded from the study.
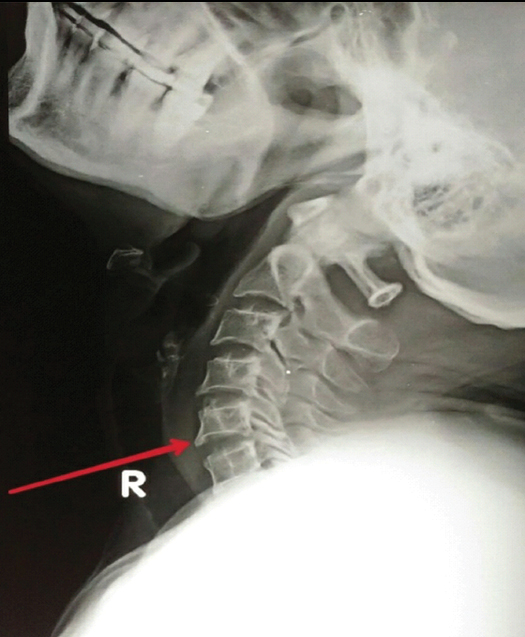
After thorough history and ENT examination, an upper gastrointestinal endoscopy was performed to rule out any obvious lesion in pharynx or oesophagus. Those patients with no evident cause for dysphagia, were later screened with a digital X-ray of cervical spine in lateral view and an orthopaedic opinion and in some neurosurgical opinion was taken [Table/Fig-1,2]. All the data were recorded in a proforma.
X-ray cervical spine lateral view showing osteophyte at C4.

X-ray cervical spine lateral view showing osteophyte at C5.
Statistical Analysis
Qualitative data were represented in the form of frequency and percentage. Association between qualitative variables was assessed by chi-square test or Fischer’s-exact test. A p-value of less than 0.05 was considered statistically significant. Statistical analysis was done with IBM SPSS version 22.0 for windows.
Results
A total of 70 (100%) patients were taken into the study, after ruling out intraluminal causes of dysphagia by doing thorough ENT examination and upper gastrointestinal endoscopy.
The patients of age group 25-59 years, of either sex were studied. Mean age being 41.3 years. Most of the patients were between 30-49 years (64.3%) of age [Table/Fig-3].
Age distribution of patients.
| Age (in years) | Frequency |
|---|
| <30 | 10 (14.3%) |
| 30-39 | 25 (35.7%) |
| 40-49 | 20 (28.6%) |
| 50-59 | 15 (21.4%) |
| Total | 70 (100%) |
Amongst 70 (100%) patients in our study, 40 (57.1%) were female patients and 30 (42.9%) male patients.
Out of 70 (100%) patients, 34 (48.6%) patients had cervical spine degenerative changes and 36 (51.4%) patients had normal X-ray cervical spine [Table/Fig-4].
X-ray cervical spine lateral view interpretation.
| Findings | Frequency |
|---|
| Osteophytes | 21 (30%) |
| Other Spondylotic changes | 13 (18.6%) |
| Normal | 36 (51.4%) |
| Total | 70 (100%) |
Out of 34 (48.6%) patients with cervical spine degenerative changes, 21 (30%) patients were found to have anterior cervical osteophytes.
Out of 21 patients with osteophytes in our study, 13 patients had a single osteophyte while 8 patients were found to have osteophytes at multiple levels of cervical vertebrae. Highest frequency of osteophytes was found to be at the level of C5 in 15 patients (71.4%) followed by C6 level in 8 patients (38%) [Table/Fig-5].
Level of cervical vertebrae with osteophytes.
| Level of osteophyte | Frequency |
|---|
| C3 | 3 |
| C4 | 2 |
| C5 | 15 |
| C6 | 8 |
| C7 | 2 |
The patients with dysphagia in age group 40-49 years were found to have highest incidence of osteophytes [Table/Fig-6].
Presence of osteophytes in various age groups.
| Age (in years) | Osteophyte present |
|---|
| Yes (n=21) | Number (n=49) |
|---|
| <30 | 0 | 10 |
| 30-39 | 4 | 21 |
| 40-49 | 9 | 11 |
| 50-59 | 8 | 7 |
Presence of osteophytes in males and females was compared and found to be statistically insignificant [Table/Fig-7].
Presence of osteophytes in either sex.
| Gender | Presence of osteophyte | Chi-square test |
|---|
| Yes (n=21) | No (n=49) |
|---|
| Male | 9 | 21 | NS p>0.05 |
| Female | 12 | 28 |
NS: Not Significant
Amongst 70 (100%) patients, 21 (30%) patients had osteophytes, p-value for which was calculated as less than 0.001 which was statistically significant [Table/Fig-8]. Dysphagia in these patients could be attributed to the osteophytes impinging on pharynx or oesophagus.
Number of patients with cervical spine changes with/without osteophytes.
| Cervical spine changes) | Presence of osteophyte | Fisher’s exact Test |
|---|
| Yes (n=21) | No (n=49) |
|---|
| Present | 21 | 13 | p<0.001 |
| Absent | 0 | 36 |
Discussion
Dysphagia can be caused either due to compression of hypopharynx or oesophagus by external cause or by some intrinsic oesophageal wall pathologies [5]. Dysphagia in patients with anterior osteophytes may be explained by the fact that the hypopharynx and oesophagus rests on the anterior border of the cervical vertebrae from C3-C7. Although osteophytes can form at any cervical level but probably due to greater load-bearing and mobility they are most common at C5-C6 and C6-C7 [6].
Mechanism causing dysphagia in patients with osteophytes can be described as, impinging of large osteophyte on pharynx or oesophageal segment thus causing mechanical obstruction [7-9]. Similarly small osteophytes impinging on pharyngoesophageal segment especially in postcricoid region, can cause obstruction [10,11]. Another mechanism suggested by Crowther A and Ardan GM is osteophyte causing impairment of tilting of epiglottis over laryngeal inlet [10]. Inflammation of prevertebral fascia causing fibrosis and adhesions due to cervical spine disease may also cause dysphagia [9,12]. Also, rare conditions like Forestier’s disease can cause dysphagia. Forestier’s disease also known as Diffuse Idiopathic Skeletal Hyperostosis (DISH) is an ossifying diasthesis characterised by spinal and peripheral enthesopathy, mainly constituted of ossification of anterior longitudinal ligaments [13].
Osteophytes are more commonly found in elderly age group [6] hence osteophytes causing dysphagia is looked for in elderly; however, in our study we have seen osteophytes causing dysphagia in relatively younger age group, which can be easily diagnosed with radiograph.
In a study by Strasser G et al., 1.7% of patients with dysphagia were found to have anterior cervical osteophytes [14]. In present study 30% of the patients were found to have anterior cervical osteophytes after ruling out other common causes. The difference was found in study by Strasser G et al., as they included all patients with dysphagia, irrespective of the cause, while in present study, we have ruled out patients with all commoner causes.
A case report by Silveri C et al., showed progressive dysphagia and hoarseness of voice being cured by resection of a cervical osteophyte [1]. Similarly Albayrak I et al., reported dysphagia caused due to large cervical osteophyte in a patient with ankylosing spondylitis [15].
A study by Seidler TO et al., showed highest frequency of osteophytes being present at the level of C5-C6 [16]. Present study, also had similar results with 15 patients (71.4%) having osteophytes at C5 level.
Early diagnosis of cervical osteophytes would help in early initiation of treatment modalities like neck exercises and physiotherapy with the orthopaedician opinion. Conservative medical therapy is used in early stages of disease; however, patients with intractable disease may require surgical intervention by osteophytectomy [17].
Limitation
The limitation of present study was its small sample size. Also, further evaluation of osteophytes with other imaging modalities like computed tomography, video fluoroscopy could be done.
Conclusion
Anterior cervical osteophyte as a cause of dysphagia can be overlooked by otorhinolaryngologists while looking for commoner causes. It should be looked for even in relatively younger patients, as it is easily diagnosed even with minimal facility of X-ray and thus help in early effective management.
NS: Not Significant
[1]. Silveri C, Velasco JM, Silveri A, Dysphagia produced by cervical spine osteophytes :a case reportColuna/Columna 2014 13(2):150-52.10.1590/S1808-18512014130200453 [Google Scholar] [CrossRef]
[2]. Mosher HP, Exostoses of the cervical vertebrae as a cause for difficulty in swallowingLaryngoscope 1926 36:181-82.10.1288/00005537-192603000-00004 [Google Scholar] [CrossRef]
[3]. Kissel MT, Youmans HP, Posttraumatic anterior cervical osteophyte and dysphagia: surgical report and literature reviewJ Spinal Disord 1992 5(1):104-07.10.1097/00002517-199203000-000141571607 [Google Scholar] [CrossRef] [PubMed]
[4]. Seo JW, Park JW, Jang JC, Kim JW, Lee YG, Kim YT, Anterior cervical osteophytes causing dysphagia and paradoxical vocal cord motion leading to dyspnea and dysphoniaAnn Rehabil Med 2013 37(5):717-20.10.5535/arm.2013.37.5.71724236261 [Google Scholar] [CrossRef] [PubMed]
[5]. Weinshel SS, Maiman DJ, Mueller WM, Dysphagia associated with cervical spine disorders: Pathologic relationship?J Spinal Disord 1988 1(4):312-16.10.1097/00002517-198800140-000072980259 [Google Scholar] [CrossRef] [PubMed]
[6]. Chen YR, Sung K, Tharin S, Symptomatic anterior cervical osteophyte causing dysphagia: case report, imaging, and review of the literatureCureus 2016 8(2):e47310.7759/cureus.473 [Google Scholar] [CrossRef]
[7]. Lambert JR, Tepperman PS, Jimenez J, Newman A, Cervical spine disease and dysphagia: four new cases and a review of the literatureAm J Gastroenterol 1981 76:35-40. [Google Scholar]
[8]. Resnick D, Shapiro RF, Wiesner KB, Niwayama G, Utsinger PD, Shaul SR, Diffuse Idiopathic Skeletal Hyperostosis (DISH)Semin Arthritis Rheum 1978 17:153-87.10.1016/0049-0172(78)90036-7 [Google Scholar] [CrossRef]
[9]. Sobol SM, Rigual NR, Anterolateral extrapharyngeal approach for cervical osteophyteinduced dysphagia; literature reviewAnn Otol Rhinol Laryngol 1984 93:498-504.10.1177/0003489484093005176388464 [Google Scholar] [CrossRef] [PubMed]
[10]. Crowther A, Ardran GM, Dysphagia due to cervical spondylosisJ Laryngol Otol 1985 99:1167-69.10.1017/S00222151000983524056603 [Google Scholar] [CrossRef] [PubMed]
[11]. Davies RP, Sage MR, Brophy BP, Cervical osteophyte induced dysphagiaAustralas Radiol 1989 33(3):225-27.10.1111/j.1440-1673.1989.tb03278.x2604632 [Google Scholar] [CrossRef] [PubMed]
[12]. Bone RC, Nahum AM, Harris AS, Evaluation and correction of dysphagiaproducing cervical osteophytosisLaryngoscope 1974 84(11):2045-50.10.1002/lary.55408411184437247 [Google Scholar] [CrossRef] [PubMed]
[13]. Najib J, Goutagny S, Peyre M, Faillot T, Kalamarides M, Forestier’s disease presenting with dysphagia and dysphoniaPan Afr Med J 2014 17:16810.11604/pamj.2014.17.168.245325120881 [Google Scholar] [CrossRef] [PubMed]
[14]. Strasser G, Schima W, Schober E, Pokieser P, Kaider P, Denk A, Cervical osteophytes impinging on the pharynx: importance of size and concurrent disorders for development of aspirationAmerican Journal of Roentgenology 2000 174(2):449-53.10.2214/ajr.174.2.174044910658723 [Google Scholar] [CrossRef] [PubMed]
[15]. Albayrak I, Bağcacı S, Sallı A, Kucuksen S, Uğurlu H, A rare cause of dysphagia: compression of the oesophagus by an anterior cervical osteophyte due to ankylosing spondylitisKorean J Intern Med 2013 28(5):614-18.10.3904/kjim.2013.28.5.61424009460 [Google Scholar] [CrossRef] [PubMed]
[16]. Seidler TO, Pèrez Alvarez JC, Wonneberger K, Hacki T, Dysphagia caused by ventral osteophytes of the cervical spine: clinical and radiographic findingsEur Arch Otorhinolaryngol 2009 266(2):285-91.10.1007/s00405-008-0735-418587593 [Google Scholar] [CrossRef] [PubMed]
[17]. Carlson ML, Archibald DJ, Graner DE, Kasperbauer JL, Surgical management of dysphagia and airway obstruction in patients with prominent ventral cervical osteophytesDysphagia 2011 26(1):3410.1007/s00455-009-9264-620099000 [Google Scholar] [CrossRef] [PubMed]