Common Trunk Arising from Ansa Cervicalis Innervating Strap Muscles along with Sternocleidomastoid: A Case Report
Binita Chaudhary1, Prabhas Ranjan Tripathy2, Manisha Rajanand Gaikwad3
1 Assistant Professor, Department of Anatomy, All India Institute of Medical Science, Bhubaneswar, Odisha, India.
2 Assistant Professor, Department of Anatomy, All India Institute of Medical Science, Bhubaneswar, Odisha, India.
3 Additional Professor, Department of Anatomy, All India Institute of Medical Science, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Binita Chaudhary, Assistant Professor, Department of Anatomy, All India Institute of Medical Science, Sijua, Patrapada, Dist-Khorda, Bhubaneswar-751019, Odisha, India.
E-mail: binitachaudhary18@yahoo.in
The infrahyoid muscles (omohyoid, sternohyoid, sternothyroid and thyrohyoid) are innervated by Ansa Cervicalis (AC) and are involved in movement of hyoid bone, thyroid cartilage during vocalisation and swallowing. Though variations in the formation and looping pattern of AC are reported in the literature, here we present a rare branching pattern of AC. During routine undergraduate dissection class, we have come across a rare variant of AC which has clinical significance. On the left side of the neck a common trunk was found to be arising from the loop of AC which trifurcated to supply inferior belly of omohyoid, sternohyoid and sternothyroid. This trunk was also providing a branch to sternocleidomastoid. Surgeons should keep such variation in mind while operating in the carotid region. If accidently during surgery or stab wound in the neck, this common trunk is cut, the function of inferior belly of omohyoid, sternohyoid and sternothyroid will be compromised leading to difficulty in deglutition and voice production. In unilateral vocal cord paralysis, artificially created anastomosis between AC and recurrent laryngeal nerve gives excellent to normal result in affected vocal cord. In thyroid surgery, recurrent laryngeal nerve is injured leading to vocal fold paralysis. To restore the nerve supply to the larynx in such cases neurorrhaphy (end to end anastomosis) between AC and recurrent laryngeal nerve is the choice of treatment.
Carotid triangle, Infrahyoid muscle, Laryngeal reinnervation, Neurorrhaphy
Case Report
During routine undergraduate dissection class, anterior triangle of a male cadaver of around 60 years was dissected and structures like strap muscle, Carotid Artery (CA), Internal Jugular Vein (IJV), Vagus nerve and AC were explored. The specimen was washed and contents of the carotid triangle were painted with poster colour. Red, blue and yellow colours were used for artery, vein and nerves respectively.
On the left side of the neck a common trunk of 2.3 cm length was found to be arising from the loop of AC. It was situated lateral to the lower part of larynx, behind the inferior belly of omohyoid, in front of Common Carotid Artery (CCA) and IJV. From the proximal part of this common trunk on the left side [Table/Fig-1A], a branch arose to supply sternocleidomastoid muscle. To show the branches from the common trunk, omohyoid and sternocleidomastoid muscle were reflected and the nerve to sternocleidomastoid was severed. This common trunk trifurcated to supply the sternohyoid, sternothyroid and inferior belly of omohyoid [Table/Fig-1B,2]. The formation of superior root, inferior root and loop of AC was normal. On the other side AC had normal branching pattern [Table/Fig-3A].
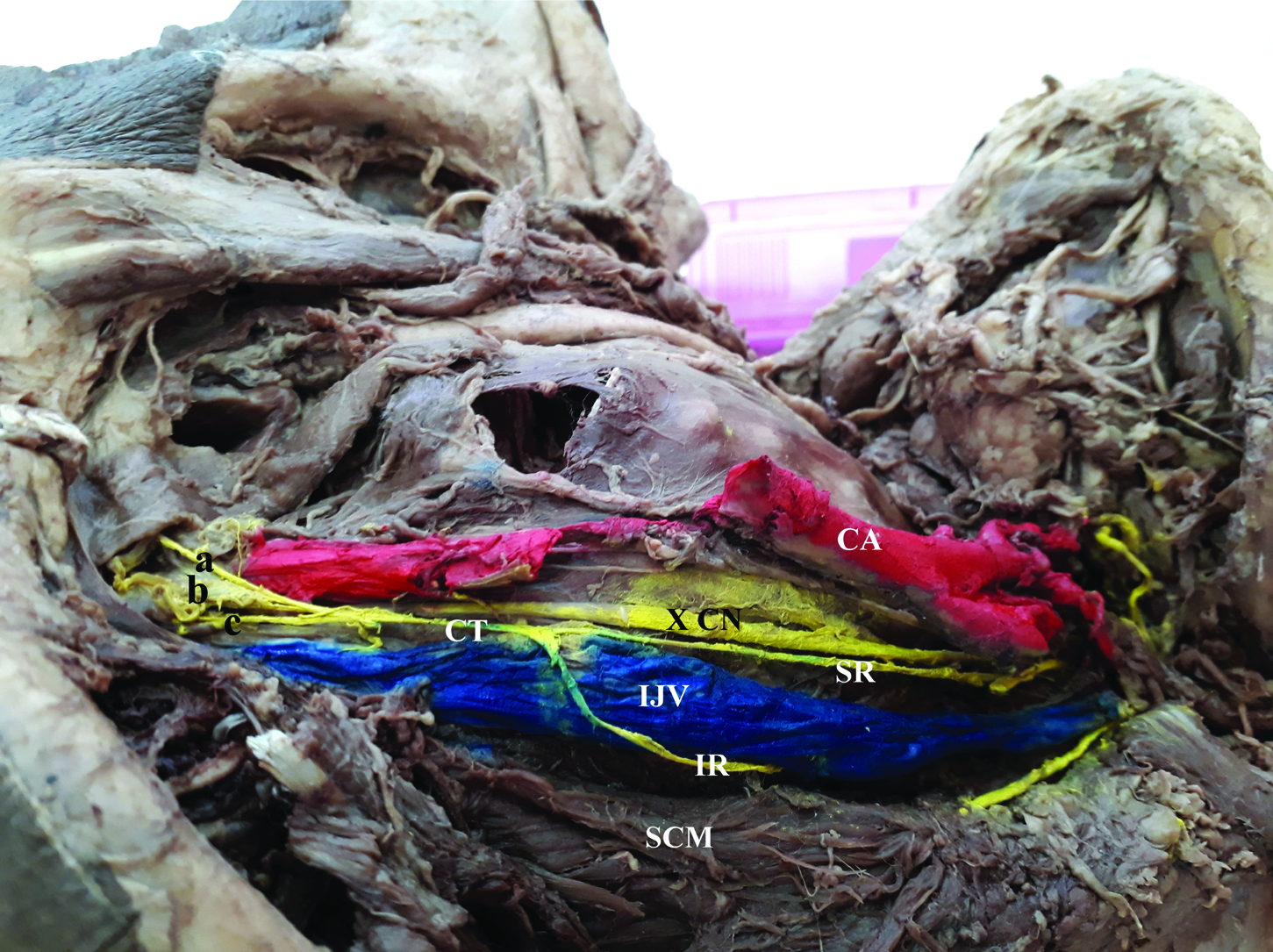
A) Common trunk arising from the loop of ansa cervicalis giving branch to sternocleidomastoid muscle. SH-Sternohyoid, ST-Sternothyroid, TH-Thyrohyoid, OH-Omohyoid, SR-Superior root, IR-Inferior root, CT-Common trunk, SCM-Sternocleidomastoid, br- branch to sternocleidomastoid. CA- Carotid artery, IJV-Internal jugular vein. B) Omohyoid is reflected to show the common trunk trifurcating to supply sternohyoid, sternothyroid, inferior belly of omohyoid. SR-superior root, IR- Inferior root, CT- Common trunk, X-Vagus Nerve, XI- Accessory Nerve. SCM- Sternocleidomastoid: a-branch to sternohyoid (SH); b-branch to Sternothyroid (ST); c-branch to inferior belly of omohyoid.

Common trunk (CT) arising from loop of ansa cervicalis is trifurcating to supply sternohyoid: (a) sternothyroid; (b) and inferior belly of omohyoid; (c) Formation of loop of ansa cervicalis by the union of superior root (SR) and inferior root (IR) is normal.
CA- Carotid artery, IJV- Internal jugular vein, X- Vagus nerve.
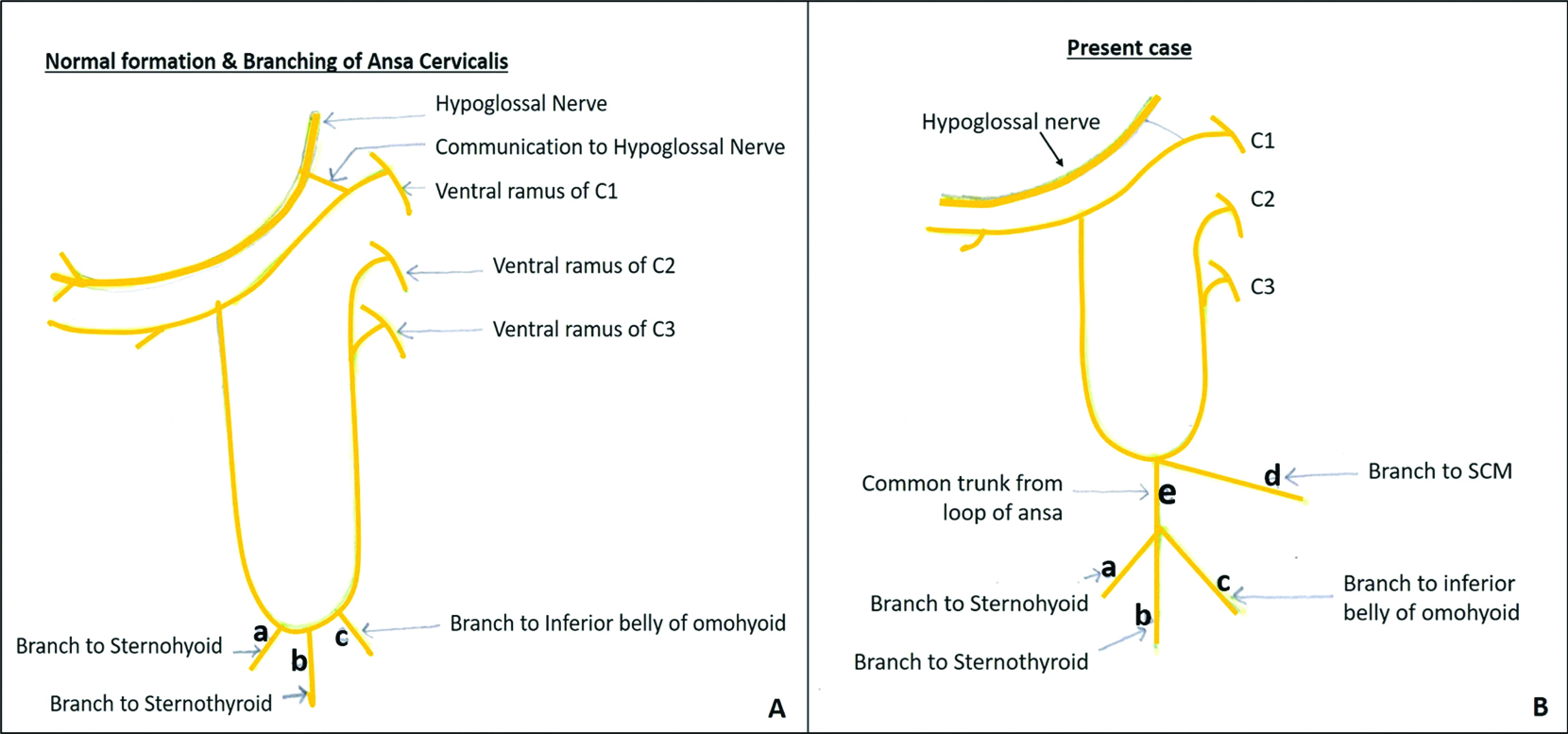
A) Normal formation and branching pattern of ansa cervicalis. Branches to sternohyoid, sternothyroid and inferior belly of omohyoid arises directly from the loop. B) Present case: Common trunk giving branch to sternocleidomastoid muscle (SCM). Common trunk (CT) trifurcating to supply the a-sternohyoid, b-sternothyroid, c-inferior belly of omohyoid.
Discussion
Beneath the investing layer of deep cervical fascia in the neck, longitudinal muscles are placed which are innervated by anterior rami of upper three cervical nerves. The muscles between the hyoid and manubrium sterni are known as infrahyoid muscles or strap muscles owing to their flat shape [1]. The infrahyoid muscles form the floor of the muscular triangle and below the floor lies the cervical viscera i.e., trachea, larynx, oesophagus, thyroid gland. These infrahyoid muscles are supplied by communicating branch of cervical plexus that pass from the loop between 1st and 2nd cervical rami to the hypoglossal nerve [2]. These infrahyoid muscles act as a depressor of larynx. Depression of larynx increases the volume of the resonating chambers during phonation and thus it affects the quality of voice. It opposes the elevators of larynx (i.e., mylohyoid, palatopharyngeus, stylopharyngeus, salpingopharyngeus). The strap muscles also depresses the hyoid bone [1].
During deglutition, the hyoid bone moves upwards. The infrahyoid muscles depress the hyoid bone following its elevation during deglutition. The sternothyroid muscle depresses the larynx after it is elevated in swallowing and in vocal cord movements. Variations in the formation and looping pattern of AC have been reported in the literature. D’Souza AS and Ray B has reported absence of contributing roots, loop of AC and the infrahyoid muscles received their nerve supply from vagus as the ventral rami of C1, C2, C3 were joining the vagus nerve at different levels [3]. Quadros LS et al., reported high level of ansa, low level of ansa, dual ansa with absence of inferior root, a common trunk which supplied all the strap muscles including superior belly of omohyoid [4]. Quadros LS et al., reported ‘Triple form of AC’ [5]. According to Ravindra SS et al., AC presented double loop pattern in which inferior root of AC has two separate components [6]. Normally the branches to inferior belly of omohyoid, sternohyoid, sternothyroid arises separately from the loop [Table/Fig-3A]. It is reported in the literature that the lower portion of the sternothyroid and sternohyoid muscles are innervated by a prominent common trunk in 80% of cases [7]. In the present case a common trunk arising from the loop is trifurcating to supply whole of the strap muscles [Table/Fig-2]. Our study resembles the study made by Quadros LS et al., to some extent, however in our case this common trunk was not supplying superior belly of omohyoid [4]. Also, in the present case, a branch arising from the common trunk was supplying the sternocleidomastoid muscle [Table/Fig-1A,3B] (probably C2 and C3 fibres) in addition to its motor nerve supply from spinal accessory nerve.
Because of proximity of carotid arteries, IJV, vagus nerve, thyroid gland etc., detailed anatomy of anterior triangle of neck needs meticulous attention to avoid injury to the nerves and vessels. This requires complete knowledge of three dimensional anatomy of neck. If during surgical interventions in the neck region, this common trunk gets damaged accidently then it will paralyse the strap muscles leading to dysphagia and difficulty in voice production. One of the complications of thyroid surgery is recurrent laryngeal nerve injury leading to vocal fold paralysis. In such cases to restore the nerve supply to the larynx, neurorrhaphy (end to end anastomosis) between AC and recurrent laryngeal nerve is the choice of treatment. The nerve chosen for laryngeal reinnervation should be anatomically close enough to allow neurorrhaphy. For this the donor nerve of choice is common trunk of sternohyoid and sternothyroid. If the main trunk is missing, the branch to sternothyroid is the nerve of choice [8]. Despite best effort, this common trunk may be cut and complication can still occur but it can be minimised by being vigilant during the perioperative period.
Conclusion
During thyroid surgeries, branches of AC are vulnerable to iatrogenic injury. In thyroid malignancies with lymph node metastasis modified radical neck dissection plays important role in its management. During such procedures strap muscles need to be preserved and integrity of AC should be maintained. If this common trunk is cut during surgery or stab wound in the neck, paralysis of strap muscle will cause difficulty in deglutition and voice production. Anastomosis between AC and recurrent laryngeal nerve is a preferred technique for management of iatrogenic vocal cord dysfunction.
[1]. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, Gray’s anatomy: the anatomical basis of clinical practice 2008 44240th EditionLondonChurchill Livingstone:455-56. [Google Scholar]
[2]. Datta AK, Essentials of human anatomy head & neck 2009 5th EditionKolkataCurrent Books International:98-107. [Google Scholar]
[3]. D’Souza AS, Ray B, Study of the formation and distribution of the ansa cervicalis and its clinical significanceEur J Anat 2010 14(3):143-48. [Google Scholar]
[4]. Quadros LS, Bhat N, Babu A, D’Souza AS, Anatomical variations in the ansa cervicalis and innervation of infrahyoid musclesInt J Anat Res 2013 1(2):69-74. [Google Scholar]
[5]. Quadros LS, Prasanna LC, D’souza AS, Singh A, Kalthur SG, Unilateral Anatomical variation of the ansa cervicalisAustralas Med J 2015 8(5):170-73.10.4066/AMJ.2015.237126097518 [Google Scholar] [CrossRef] [PubMed]
[6]. Ravindra SS, Kumar N, Nayak SB, Jyothsna R, Anitha P, Unusual looping pattern of ansa cervicalis: Case reportOA Case Rep 2013 2(9):8110.13172/2052-0077-2-9-792 [Google Scholar] [CrossRef]
[7]. Prades JM, Gavid M, Dubois MD, Dumollard JM, Timoshenko AT, Peoc’h M, Surgical anatomy of the ansa cervicalis nerve: Which branch to use for laryngeal reinnervation in humansSurg Radiol Anat 2015 37(2):139-45.10.1007/s00276-014-1355-x25165021 [Google Scholar] [CrossRef] [PubMed]
[8]. Wang W, Chen D, Chen S, Li D, Li M, Xia S, Laryngeal reinnervation using ansa cervicalis for thyroid surgery related unilateral vocal cord paralysis: A long term outcome analysis of 237 casesPLoS One 2011 6(4):e1912810.1371/journal.pone.001912821559458 [Google Scholar] [CrossRef] [PubMed]