Carcinosarcoma Gallbladder: A Rare Variety of Gallbladder Malignancy
Koustav Jana1, Amit Kumar Das2, Suman Saha3, Ranajoy Ghosh4, Sukanta Ray5
1 Senior Resident, Department of Division of Surgical Gastroenterology, School of Digestive and Liver Diseases, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
2 Senior Resident, Department of Division of Surgical Gastroenterology, School of Digestive and Liver Diseases, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
3 Senior Resident, Department of Division of Surgical Gastroenterology, School of Digestive and Liver Diseases, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
4 Associate Professor, Department of Division of Gastrointestinal Pathology, School of Digestive and Liver Diseases, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
5 Professor, Department of Division of Surgical Gastroenterology, School of Digestive and Liver Diseases, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sukanta Ray, Professor, Division of Surgical Gastroenterology, School of Digestive and Liver Diseases, Institute of Postgraduate Medical Education and Research, 244 A. J.C. Bose Road, Kolkata-700020, West Bengal, India.
E-mail: drsukantaray@yahoo.co.in
Gallbladder malignancy is frequently found in Indian population. Most of them are adenocarcinoma variety whereas carcinosarcoma variety is quite rare. It is typically characterised by presence of both epithelial and mesenchymal components. The prognosis of this variety is poorer because of its aggressive nature and delayed diagnosis. Here we report a case of Carcinosarcoma of Gallbladder (CSGB) in a 40-year-old lady presenting to us with features of acute cholecystitis and gallbladder mass. She was treated with radical cholecystectomy, bile duct excision and Roux-en-Y Hepaticojejunostomy (RYHJ). Histopathological examinations reveal pleomorphic spindle cells as well as epitheloid cell. In postoperative period she received adjuvant chemotherapy. Despite all these treatment she developed recurrence at seven months follow up.
Acute cholecystitis, Gallbladder mass, Radical cholecystectomy
Case Report
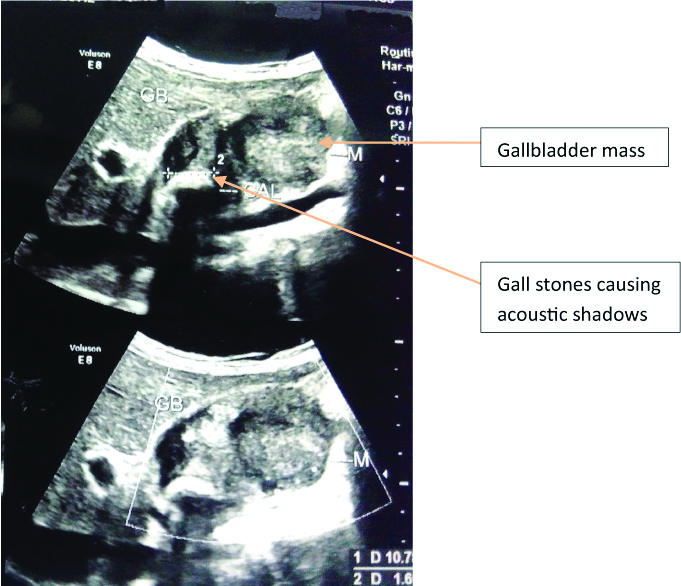
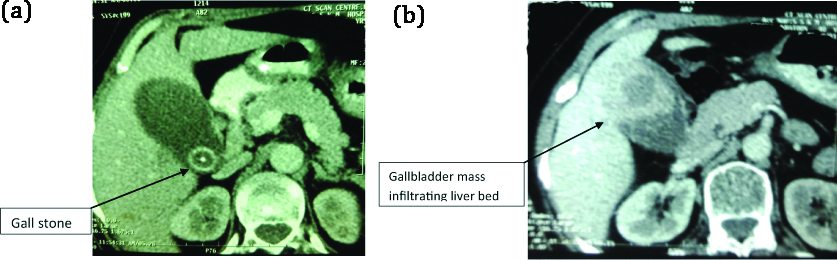
A 40-year-old woman presented with recurrent episodes of upper abdominal pain and vomiting for one month. Pain was acute in onset, colicky in nature, without any radiation and associated with non bilious vomiting. There was no history of jaundice, fever or upper gastrointestinal bleeding. Her medical history was otherwise unremarkable. She was initially managed conservatively at a local hospital. Ultrasonography at the time of acute episode revealed multiple calculi and a soft tissue mass measuring 33 mm×17 mm in the lumen of the gallbladder associated with multiple enlarged periportal lymph nodes [Table/Fig-1]. She came to the present institution for further evaluation and management. On physical examination a gallbladder mass was palpable. Rests of the physical findings were within normal limits. Contrast-enhanced Computed Tomography scan (CT scan) of the abdomen revealed cholelithiasis with heterogeneously enhancing mass (4.3 cm×5.1 cm) in fundus of gallbladder with loss of fat planes with adjacent hepatic parenchyma at places [Table/Fig-2a,b]. There were multiple enlarged lymph nodes (approximate size 1.5 cm) in periportal region. Common bile duct and intrahepatic biliary radicles were not dilated. Preoperative serum Cancer Antigen (CA) 19-9 was 87 U/mL (0-37 U/mL).
USG of abdomen showing gallbladder mass as well as gall stone.
a) CT scan of abdomen showing gallbladder stone and periportal lymphadenopathy; b) CT scan of abdomen showing gallbladder mass involving liver bed.
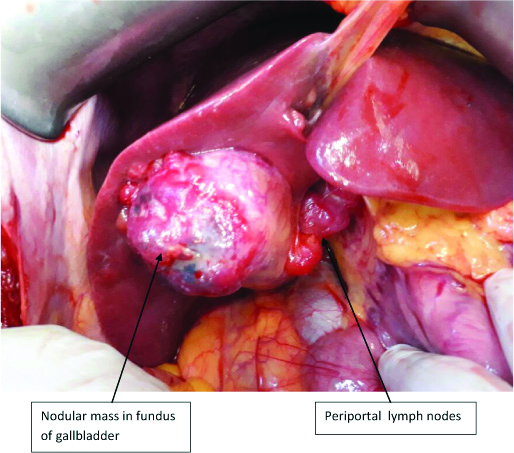
A preoperative diagnosis of gallbladder malignancy was made. After adequate preoperative preparation, she underwent staging laparoscopy followed by radical cholecystectomy (including hepatoduodenal ligament lymphadenectomy), excision of bile duct with RYHJ. Intraoperative findings included a large gallbladder mass involving cystic duct and the common bile duct [Table/Fig-3]. Portal vein and hepatic artery were not invaded by the mass. There were multiple enlarged lymph nodes in the hepatoduodenal ligament.
Intraoperative photograph showing nodular mass involving fundus of the gallbladder with enlarged cystic and pericholedochal lymph node.
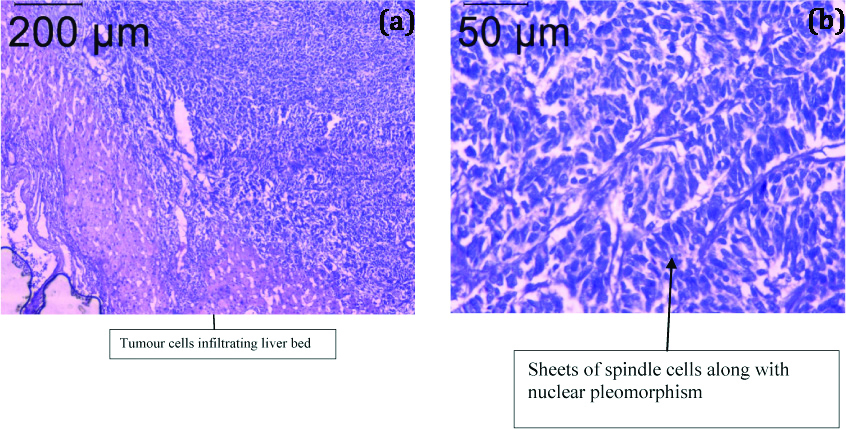
Her postoperative recovery was uneventful. Histopathological examination revealed sheets of pleomorphic spindle and epitheloid cells [Table/Fig-4a,b]. The cells have coarse chromatin. The tumour was infiltrating the liver. Resection margins were free of lesion. The final diagnosis was a CSGB. Immunohistochemical examination was not feasible. She was treated with gemcitabine based chemotherapy. The patient developed recurrence at seven months follow up.
a) Hematoxylin and eosin (10X) stained section showing tumour cells infiltrating liver bed; b) Hematoxylin and eosin (40X) stained section showing spindle cells along with nuclear pleomorphism.
Discussion
Gallbladder cancer is fairly common in East Indian women (22 cases per 1,00,000 populations annually) and most of them are adenocarcinoma [1]. Other varieties of gallbladder cancer are rare and among them CSGB is probably the rarest variety accounting less than 1% of gallbladder malignancy [2]. Till now, fewer than 100 cases have been reported in english literature [3]. The CSGB is characterised by malignant transformation of both the epithelial and mesenchymal components of the same tissue. The epithelial component usually consists of adenocarcinoma, although an element of squamous cell carcinoma is occasionally observed. The mesenchymal component typically consists of undifferentiated spindle or stellate cells admixed with various proportion of heterogeneous elements including osteosarcoma, chondrosarcoma, and rhabdomyosarcoma [4,5].
An accurate preoperative diagnosis is often not possible because of nonspecific symptoms. Moreover, imaging studies cannot differentiate it from carcinoma of the gallbladder. The clinical symptoms include right upper abdominal pain, weight loss, anorexia, fatigue, jaundice, and a palpable mass. In addition, patient may present with acute cholecystitis due to presence of associated cholecystolithiasis [6]. Similarly in the present case, the patient presented with acute abdominal pain resembling acute cholecystitis. The CT scan abdomen shows an enhanced solid mass lesion similar to that of gallbladder carcinoma. The CSGB should be suspected when calcification is observed within the tumour on CT scan [7].
Accurate diagnosis is made only after histopathological examination. An immunohistochemical examination should show that the epithelial component is positive for cytokeratin, while the mesenchymal component is positive for vimentin [5,8].
Due to paucity of cases, there is no staging system for CSGB, nor has any consensus been established on the management of CSGB. The usual treatment of choice is surgery and no successful treatment has so far been reported with radiotherapy or chemotherapy [9]. The CSGB is treated in the same way as other gallbladder cancers. In absence of metastasis, radical cholecystectomy is performed. More extensive procedures, such as right hepatectomy or extended right hepatectomy, probably increase the morbidity and mortality without any survival benefit [2,3,10].
The prognosis of CSGB is normally poor. Most patients present with either locally advanced disease or liver and peritoneal metastasis. Mean survival after diagnosis is only a few months in such patients. Even when a curative resection is performed, many patients die shortly after the operation because of recurrence or metastasis. The majority of recurrences occur within half a year of surgery [11]. In the present case, despite curative resection and adjuvant therapy, the patient developed recurrence within seven months after surgery.
Conclusion
Preoperative diagnosis of CSGB is often not possible. Surgery remains the mainstay of treatment in early stage of this disease. Because of its aggressive nature, majority of patients develop recurrence within a year of definitive surgery. More clinicopathological data and further studies are required to identify the prognostic factors of this dreadful gallbladder malignancy.
[1]. Hundal R, Shaffer EA, Gallbladder cancer: epidemiology and outcomeClin Epidemiol 2014 6:9910.2147/CLEP.S3735724634588 [Google Scholar] [CrossRef] [PubMed]
[2]. Huguet KL, Hughes CB, Hewitt WR, Gallbladder carcinosarcoma: a case report and literature reviewJ Gastrointest Surg 2005 9(6):818-21.10.1016/j.gassur.2004.12.00915985237 [Google Scholar] [CrossRef] [PubMed]
[3]. Gao S, Huang L, Dai S, Chen D, Dai R, Shan Y, Carcinosarcoma of the gallbladder: a case report and review of the literatureInt J Clin Exp Pathol 2015 8(6):7464 [Google Scholar]
[4]. Kuroki T, Tajima Y, Matsuo K, Kanematsu T, Genetic alterations in gallbladder carcinomaSurg Today 2005 35(2):101-05.10.1007/s00595-004-2906-215674488 [Google Scholar] [CrossRef] [PubMed]
[5]. Kim HH, Hur YH, Jeong EH, Park EK, Koh YS, Kim JC, Carcinosarcoma of the gallbladder: report of two casesSurg Today 2012 42(7):670-75.10.1007/s00595-012-0160-622391981 [Google Scholar] [CrossRef] [PubMed]
[6]. Zhang L, Chen Z, Fukuma M, Lee LY, Wu M, Prognostic significance of race and tumor size in carcinosarcoma of gallbladder: a meta-analysis of 68 casesInt J Clin Exp Pathol 2008 1(1):75-83. [Google Scholar]
[7]. Khanna M, Khanna A, Manjari M, Carcinosarcoma of the gallbladder: a case report and review of the literatureJ Clin Diagn Res 2013 7(3):560-62.10.7860/JCDR/2013/4924.282523634423 [Google Scholar] [CrossRef] [PubMed]
[8]. Takahashi Y, Fukushima JI, Fukusato T, Shiga J, Sarcomatoid carcinoma with components of small cell carcinoma and undifferentiated carcinoma of the gallbladderPathology International 2004 54(11):866-71.10.1111/j.1440-1827.2004.01771.x15533231 [Google Scholar] [CrossRef] [PubMed]
[9]. Sodergren MH, Silva MA, Read-Jones SL, Hubscher SG, Mirza DF, Carcinosarcoma of the biliary tract: two case reports and a review of the literatureEur J Gastroenterol Hepatol 2005 17(6):683-85.10.1097/00042737-200506000-0001615879734 [Google Scholar] [CrossRef] [PubMed]
[10]. Pu JJ, Wu W, Gallbladder carcinosarcomaBMJ Case Reports 2011 :bcr052010300910.1136/bcr.05.2010.300922700610 [Google Scholar] [CrossRef] [PubMed]
[11]. Park SB, Kim YH, Rho HL, Chae GB, Hong SK, Primary carcinosarcoma of the gallbladderJ Korean Surg Soc 2012 82(1):54-58.10.4174/jkss.2012.82.1.5422324048 [Google Scholar] [CrossRef] [PubMed]