A Modified Approach for Ultrasound- guided Lumbar Facet Joint Injection: Caudal-to-Cranial Technique
Ke-Vin Chang1, Wei-Tingwu2
1 Physical Medicine and Rehabilitation and Community and Geriatric Research Center, National Taiwan University Hospital, Bei-Hu Branch and National Taiwan University College of Medicine Taipei, Taiwan.
2 Physical Medicine and Rehabilitation and Community and Geriatric Research Center, National Taiwan University Hospital, Bei-Hu Branch and National Taiwan University College of Medicine Taipei, Taiwan.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ke-Vin Chang, No. 87, Neijiang Street, Wanhua District, Taipei City, Taiwan 108.
E-mail: kv.chang011@gmail.com
Pain, Rehabilitation, Sonography
Dear editor,
Low back pain is the most prevalent musculoskeletal complaint globally, while lumbar facet joint osteoarthritis appears to be one of its most common causes [1]. The lumbar facet joint is a real synovial joint, with Superior Articular Process (SAP) and Inferior Articular Process (IAP), hyaline cartilage surfaces, a synovial membrane, and a fibrous capsule. The facet joint receives dual innervation from the medial branches of the nerve roots above and below the target vertebrae. Pathological findings include hypertrophic articular processes, thickening joint capsules, narrow intra-articular gaps, and irregular bony contours. Non operative treatments consist of oral analgesics, physical therapy, corticosteroid injections, and administration of regenerative medicine.
In recent years, ultrasound has been widely used in viewing axial spines [2,3]. Regarding lumbar facet joint arthropathy, ultrasound-guided injection provides similar efficacy as fluoroscopic guidance but provides benefits of zero radiation and real-time imaging. Two approaches can be used to treat painful facet joints through ultrasound guidance. Medial branch block usually accompanies radiofrequency ablation, but the nerves above and below the target level require blockage for relief of the painful lumbar facet joint. Another approach is direct injection of corticosteroid or regenerative regimens such as dextrose or platelet-rich plasma to the infra-articular or periarticular regions. The very first approach to ultrasound-guided facet joint injection was proposed by Galiano K et al., and was also validated by computed tomography images [4]. This method places a curvilinear transducer at the short axis of the lumbar spine for visualizing the facet joint gap [5]. Then, the needle is introduced in-plane from a lateral to medial trajectory [Table/Fig-1a]. However, the joint opening might be obscured by the bony spurs and make it difficult for the physician to differentiate the joint from the inferior portion of the laminae.
a) The traditional ultrasound-guided lateral to medial approach for lumbar facet joint injection. The modified caudal to cranial ultrasound-guided technique for lumbar facet injection using curvilinear (b) and linear transducers (c) (Ecube 15; Alpinion, Seoul, Korea) is also shown.
SAP: superior articular process; IAP: inferior articular process; TP: transverse process; black arrow: needle.
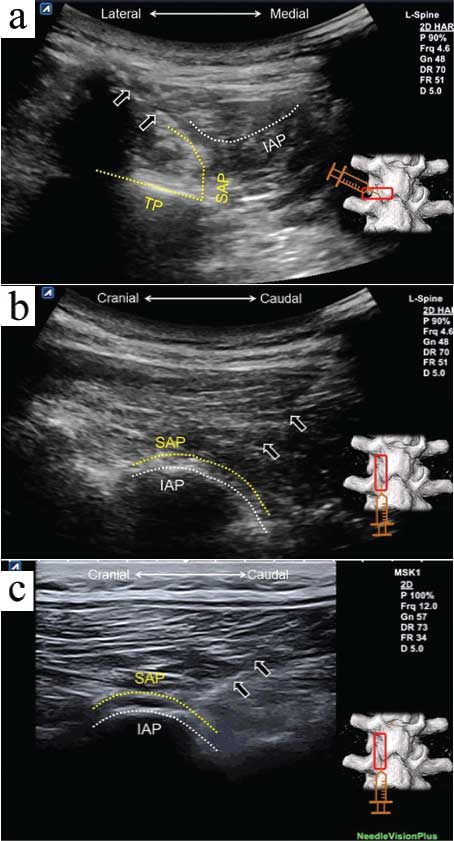
Therefore, we propose another ultrasound-guided approach for facet joint injection. First, the transducer is placed on the long axis of the facet column, which appears like a camel’s hump. The bony contour of the SAP is usually more superficial than the IAP. The needle is advanced from the caudal to cranial direction, targeting the space between the articular lines of the SAP and IAP [Table/Fig-1b]. Once the needle reaches the desired area, the transducer can be rotated 90° to further confirm that the needle tip is located inside the joint. This technique has more advantages than the traditional lateral to medial method. First, the angle of the trajectory can be less steep for better visualisation of the needle, and the procedure can be conducted even using a linear transducer [Table/Fig-1c]. Second, this approach allows injections of several facet joints by only creating a needle entry. The most important advantage regarding the injection in the L4/5 and L5/S1 facets is that the needle advancement will no longer be hindered by the iliac crest, which easily blocks the needle entrance during the traditional lateral to medial approach.
The present study is supported by National Taiwan University Hospital, Bei-Hu Branch, Ministry of Science and Technology (MOST 106-2314-B-002-180-MY3) and Taiwan Society of Ultrasound in Medicine.
[1]. Meucci RD, Fassa AG, Faria NM, Prevalence of chronic low back pain: systematic reviewRev Saude Publica 2015 49:110.1590/S0034-8910.201504900587426487293 [Google Scholar] [CrossRef] [PubMed]
[2]. Chang KV, Lin CP, Hung CY, Ozcakar L, Wang TG, Chen WS, Sonographic nerve tracking in the cervical region: a pictorial essay and video demonstrationAm J Phys Med Rehabil 2016 95(11):862-70.10.1097/PHM.000000000000055727362696 [Google Scholar] [CrossRef] [PubMed]
[3]. Chang KV, Lin CP, Lin CS, Wu WT, Karmakar MK, Ozcakar L, Sonographic tracking of trunk nerves: essential for ultrasound-guided pain management and researchJ Pain Res 2017 10:79-88.10.2147/JPR.S12382828115867 [Google Scholar] [CrossRef] [PubMed]
[4]. Galiano K, Obwegeser AA, Bodner G, Freund M, Maurer H, Kamelger FS, Ultrasound guidance for facet joint injections in the lumbar spine: a computed tomography-controlled feasibility studyAnesth Analg 2005 101(2):579-83.10.1213/01.ANE.0000158609.64417.9316037179 [Google Scholar] [CrossRef] [PubMed]
[5]. Karkucak M, Kurt M, Ozcakar L, Ultrasound video demonstration for lumbar facet joint injectionAm J Phys Med Rehabil 2016 95(10):e165-66.10.1097/PHM.000000000000051127149582 [Google Scholar] [CrossRef] [PubMed]