Introduction
Preoperative anxiety is associated with problems such as difficult venous access, jaw relaxation and coughing during induction of anaesthesia, autonomic fluctuations and increased anaesthesia requirements. It has also been correlated with increased pain, nausea and vomiting in the postoperative period, prolonged recovery and increased risk of infection. Most patients experience preoperative anxiety which is a major concern before surgery and it has been suggested that the reduction in preoperative anxiety levels might be associated with better surgical outcomes, shorten hospital stay and minimise lifestyle disruptions.
Aim
The aim of the present study was to assess the pre and post procedure anxiety level of the patient undergoing surgery under spinal anaesthesia, after being shown a video of how the procedure is performed and to assess the ease of the anaesthesiologist performing the Subarachnoid Block (SAB).
Materials and Methods
The present study included 100 patients divided in two groups. One group who had a face-to-face interview with the anaesthesiologist and the other group were shown a audio-visual video of the procedure, posted for elective surgery under SAB. The anxiety levels of the patients was evaluated using Visual Analogue Scale (VAS) scores, State-Trait Anxiety Inventory (STAI) questionnaire and the satisfaction level of the anaesthesiologist using Likert’s scale. The postoperative anxiety values were assessed when the patients were shifted to recovery room. The statistical tests used were Student’s t-test for continuous data, chi-square test for categorical variables. One-way repeated ANOVA to analyse the significance.
Results
The VAS scores in between Group 1 and Group 2 showed that the pre-intervention, pre-procedure and post-procedure were statistically not significant. The pre-intervention VAS score was 3.23±0.92 in Group 1 and 2.78±0.82 in Group 2 (p-value=0.4), the pre-procedure VAS score was 3.04±0.84 in Group 1 and 2.67±0.76 in Group 2 (p-value=0.6), the post-procedure VAS score was 3.84±0.96 in Group 1 and 2.88±0.9 in Group 2 (p-value=0.5). The state anxiety between the pre-intervention, pre-procedure and post-procedure in Group 1 and Group 2 the data was statistically significant (p=0.01 and p=0.02). The trait anxiety between pre-intervention, pre-procedure and post-procedure in Group 1 and Group 2 showed that the data was statistically significant (p=0.03 and p=0.01) respectively. The Likert’s score which was assessed by the anaesthesiologist performing the block, there was statistically highly significant difference present between the groups (p=0.00).
Conclusion
Educating the patient is important for helping in reducing the fear and anxiety of patient, face-to-face interview is a good way of providing information to the patient but multimedia information is better as patients are more receptive to audio-visual information.
Introduction
Fear and anxiety are compound phenomena that have psychological, motor, somatic-vegetative and metabolic components. The very thought of surgery and anaesthesia increases the feeling of anxiety and fear. The dimension of fear and anxiety has inconvenient influence on the recovery time, quantity of complications and the discomfort felt by patients.
The major changes in life are the factors that cause anxiety and the most important life changing factor is surgery [1]. The surgical act affects any subject by narcissistic damage, which is responsible for varied psychological reactions; some are the anaesthesia fantasies, the surgical aggression of the human body, fear of death, fear of not waking up after anaesthesia. Lack of information and other factors contribute to the occurrence of symptoms and psychiatric disorders such as anxiety, depression, confusion, delirium, agitation and acute psychosis.
Hospitalisation, regardless of the disease, is known to provoke anxiety, and the level of anxiety in patient’s posted for surgery is very high. If unrecognised, prolonged anxiety creates stress which may subsequently harm the patient and delay recovery. Preoperative anxiety is a challenging concept in the preoperative and peri-operative care of the patients [2].
Increased anxiety before surgery is associated with patho-physiological responses such as tachycardia, hypertension and dysrhythmias [2]. It may also worsen patient’s perception of pain and increased requirements for post operative analgesia and decreases the overall patient’s satisfaction with peri-operative care [3].
Fear patients have regarding subarachnoid block include permanent nerve damage leading to paralysis, seeing the surgery, hearing the surgical procedure, back pain, headaches and the prospect of a needle in the back only very few patients had the understanding of cardiovascular risks and risk of aspiration related to general anaesthesia [4].
The evaluation of the effectiveness of pamphlets and video tapes in affecting a patient’s recall of information and satisfaction is limited in anaesthesia. Patients state that a video offers a step by step explanation of events, a tedious endeavour for anaesthesiologist to conduct repeatedly [5]. Some studies have addressed the influence of videos on peri-operative anxiety in patients undergoing surgical procedures under General Anaesthesia (GA) [4,5]. The results have been mixed, and none of the previous studies focused explicitly on video-based risk education. A previous study included patients undergoing regional anaesthesia techniques or patients who underwent more invasive anaesthesia techniques, such as placement of invasive monitoring devices, however the conclusion of the study was unclear as to whether the placement of the video before or after the preanaesthetic interview is important [6].
None of the previous studies have assessed the anxiety of patient as well as satisfaction of the anaesthesiologist while performing the subarachnoid block. With this hypothesis we therefore planned the present study, to compare the anxiety level in patients and satisfaction of the anaesthesiologist after the multimedia information and face-to-face interview [7].
Materials and Methods
The present randomised control study was conducted in the Department of Anaesthesiology, Himalayan Institute of Medical Sciences (HIMS), Swami Ram Nagar, Dehradun, India, over a period of one year from July 2015- July 2016. Subjects were recruited from patients presenting in the Department of Orthopaedics, Urology, Gynaecology and General surgery for elective surgical procedure under spinal anaesthesia. Written Informed consent was obtained from all the subjects after explaining the procedure.
Sample size and sampling method: A previous study was taken in to account to evaluate the sample size with α=0.05, power=0.80, SD=8.9, for comparison of continuous and quantitative data, a minimum of 50 patients in each group is required. Therefore a total of 100 patients were included in two groups [8].
Inclusion Criteria
Age group (18-80 years), both male and female patients, American Society of Anaesthesiologist (ASA) physical status I-II undergoing elective procedures under subarachnoid block.
Exclusion Criteria
Patient’s refusal for participation in the study, contraindications to spinal anaesthesia, cognitive, speech or visual disorders and any other psychiatric disorder, patients who have prior exposure to surgery, anaesthesia or operating room.
Anxiety levels was assessed at three different time intervals firstly at the time of preanaesthetic visit before the study intervention (before being shown the video or having a face-to-face interview), second time after the study intervention in the preoperative holding area (before the patient underwent the procedure of the subarachnoid block) and thirdly after spinal anaesthesia (in the postoperative period). Anxiety levels were assessed with the help of VAS and STAI [8]. The satisfaction of the anaesthesiologist who performed the subarachnoid block was assessed after the procedure with the help of 6-point Likert scale and was interpreted as: 1) extremely satisfied; 2) very satisfied; 3) somewhat satisfied; 4) somewhat dissatisfied; 5) very dissatisfied; 6) extremely dissatisfied. It was assessed according to the ease with which the procedure was performed.
Study protocol: All the patients undergoing elective surgery under spinal anaesthesia were assessed during preanaesthetic visit and were allocated alternatively into any one of the two groups. Each group had a total of 50 patients.
Group 1: Patients had a preoperative face-to-face interview with the anaesthesiologist who conducted the study regarding all the steps of spinal anaesthesia procedure in detail with associated complications starting from asepsis to how the procedure was performed.
Group 2: Patients were shown a video (2:45 minutes) of the spinal procedure in detail during the preanaesthetic visit with the help of laptop and headphones a day before the surgery. The video was a pre-recorded video of the procedure being performed on the patient.
In the Operating Room (OR) standard monitoring were applied such as Electrocardiograph (ECG), non-invasive blood pressure (systolic, diastolic and mean arterial blood pressure), and pulse oximetry (SpO2) and temperature, after that an intravenous line was secured and intravenous fluid was started as per the requirement of the patient. The baseline value of blood pressure, heart rate, SpO2 and temperature was recorded and noted.
Lumbar puncture was performed by anaesthesiologist who was blinded about the intervention. The lumber puncture was done in sitting position at L3-4 or L4-5 inter-vertebral space with median approach using 25-gauge spinal needle. Maintaining the position, 3-3.5 mL of 0.5% hyperbaric bupivacaine with or without adjuvant was given in subarachnoid space, thereafter patient was placed in the supine position. After completion of the surgery the patient was shifted to post anaesthesia care unit.
Results
All the data were constituted using software SPSS Version 22.0 and Microsoft Excel to store and manage the collected data.
The test of significance was done using Student’s t-test for continuous data and chi square test for categorical variables. One-way repeated measure ANOVA was used to analyse the significance of changes in anxiety scores over time between groups. A p-value of <0.05 was taken as reference of significance and results were interpreted as:
p>0.05: Not Significant
p<0.05: Significant
p<0.001: Highly Significant.
Results
The demographic data were compared. Mean age in Group 1 was 39.54±14.01 and in Group 2 was 35.78+10.80 (p=0.2). For the data on gender in Group 1 and Group 2 had 34 males. The education status: 17 in Group 1 and 18 in Group 2 had education more than 10th standard (p=0.3). The ASA Grade 1 patients were 41 and ASA II was 9 in both groups. Applying t-test in between Group 1 and Group 2, shows that there was no statistically significant difference between the groups in respect to VAS scoring pre-intervention, pre-procedure and post-procedure as denoted in [Table/Fig-1].
VAS scores of the patient at different time.
| VAS | Group 1 (n=50) | Group 2 (n=50) | p-value |
|---|
| Pre-intervention | 3.23±0.92 | 2.78±0.82 | 0.4 |
| Pre-procedure | 3.04±0.84 | 2.67±0.76 | 0.6 |
| Post-procedure | 3.84±0.96 | 2.88±0.9 | 0.5 |
| p-value | 0.03 | 0.01 | - |
On comparing the state anxiety between the pre-intervention, pre-procedure and post-procedure in Group 1 and Group 2 the data was statistically significant (p=0.001 and p=0.001) respectively as denoted in [Table/Fig-2].
State anxiety comparison of groups at different times.
| State anxiety | Group 1 (n=50) | Group 2 (n=50) | p-value |
|---|
| Pre-intervention | 47.66±3.7 | 48.42±5.2 | 0.3 |
| Pre-procedure | 48±4.9 | 42.64±3.4 | 0.001 |
| Post-procedure | 47.35±4.6 | 44.23±4.6 | 0.001 |
| p-value | 0.01 | 0.02 | - |
On comparing the trait anxiety between pre-intervention, pre-procedure and post-procedure in Group 1 and Group 2 Friedman’s test shows that the data was statistically significant (p=0.001 and p=0.001) respectively as shown in [Table/Fig-3].
Trait anxiety data at different times.
| Trait anxiety | Group 1 (n=50) | Group 2 (n=50) | p-value |
|---|
| Pre-intervention | 47.28±3.13 | 42.86±6.34 | 0.2 |
| Pre-procedure | 46.21±3.02 | 41.68±6.12 | 0.001 |
| Post-procedure | 47.72±3.4 | 42.81±6.3 | 0.001 |
| p-value | 0.03 | 0.01 | - |
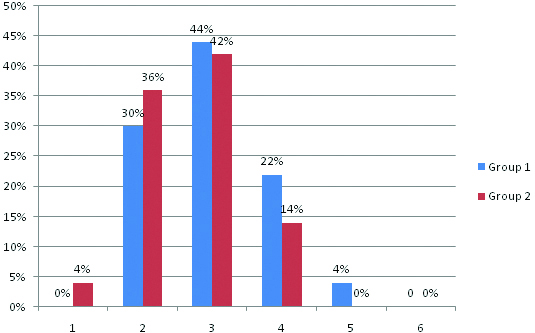
The Likert’s score which was assessed by the anaesthesiologist performing the block, there was statistically highly significant difference present between the groups, in Group 1 it was 3±0.83 and in Group 2 it was 2.78±0.81 with a p-value of 0.001 [Table/Fig-4].
Likert’s scale comparing the satisfaction level among anaesthesiologist of both the groups.
X-axis shows numbering of Likert’s scale
Y-axis shows percentage of anaesthesiologist who have assessed and numbered
Discussion
The main objective of the present study was to analyse the pre and post intervention anxiety of the patient after being shown the video or face-to-face interview of spinal anaesthesia. In the present study both the groups were similar on their demographic parameter. Education level of the patient does have an impact on understanding; however both the groups were similar in this regard.
In the present study we provided the information a day prior to the surgery via face-to-face interview and counselling of the patient and by showing a pre-recorded video of how the subarachnoid block was performed. A previous study suggested that the optimal duration and timing of media to educate patients about anaesthesia are unclear, because there were insufficient trials for a sensitivity analysis to be done. Arellano R et al., in their systematic review included interventions given on the day before or on the day of surgery. It showed a small reduction in state anxiety scores of the patients when they were seen by an anaesthesiologist immediately before surgery compared with those seen at an outpatient clinic one week before surgery or at the time of admission to the hospital [9].
If the patient understands the concept VAS, it is easy for the patient to denote. Thus, it can be inferred that the visual analog scale helps both the physician and patient to differentiate the level of post procedure and pre-procedure pain easily. We observed that state anxiety in the pre-intervention period was similar in both the groups however post intervention there was significant reduction in state anxiety in video group compared to interview alone group. A systemic review done by Lee A et al., concluded that the use of video and printed information for general process and risks of anaesthesia for patient education before surgery decrease anxiety and these interventions were also associated with increased patient knowledge [7]. During pre intervention there was no difference between the groups regarding trait anxiety; however, after intervention there was significant difference between the groups, present finding may suggest that showing the video film prior to the procedure significantly reduces the trait anxiety among the patient. Dalal KS et al., suggested that pre-anaesthetic interviews are not enough for adequate transfer of knowledge; and hence, alternative methods are required most probably because a patient does not accurately interpret knowledge from counselling alone [10].
Limitation
The limitation of present study was that, we did not explore other sources of information such as providing a printed brochure of the procedure that may have affected patient’s knowledge. Patients may interpret accurate or inaccurate information from doctors, nursing staff, friends, and the media that can influence patient’s knowledge, patients have more of an understanding and are more receptive to taking an information via multimedia and interpreting it more accurately than just counselling the patient.
Conclusion
The conclusion of the present study is that communication with the patients is important and explaining the entire procedure with the possible side-effects and giving them positive hope and courage, will help in reducing the stress and anxiety of the patients. Though, face to face interview provides with the information to the patient regarding the procedure but interpretation but people are more receptive to the visual and audio information and hence it is more useful a tool in reducing preoperative anxiety.
[1]. Kemal, Cemile, Dumani T, Sarkilari G, Selmin. The evaluation of factors affecting preoperative fear http://www.priory.com/anaesthesia/Preoperative_fear.htm [Google Scholar]
[2]. Nigussie S, Belachew T, Wolancho W, Predictors of Preoperative anxiety among surgical patients in Jimma University Specialized Teaching Hospital, South Western EthiopiaBMC Surgery 2014 14:6710.1186/1471-2482-14-6725189274 [Google Scholar] [CrossRef] [PubMed]
[3]. Akkamahadevi P, Subhramanium VV, The efficacy of different methods of Preoperative counselling on perioperative anxiety in patients undergoing regional anaesthesiaIndian J Anaesth 2016 60:58-60.10.4103/0019-5049.17481226962258 [Google Scholar] [CrossRef] [PubMed]
[4]. Sandhu K, Dash HH, Anaesthesia related neurological complicationsIndian J Anaesth 2004 48(6):439-45. [Google Scholar]
[5]. Done ML, Lee A, The use of video to convey preanaesthetic information to patients undergoing ambulatory surgeryAnaesth Analg 1998 87(5):531-36.10.1097/00000539-199809000-000059728822 [Google Scholar] [CrossRef] [PubMed]
[6]. Salzwedel C, Petersen C, Blanc I, Koch U, Goetz AE, Schuster M, The effect of detailed, video-assisted anaesthesia risk education on patient anxiety and the duration of the pre anaesthetic interview: A randomized controlled trialAesth Analg 2008 106(5):202-09.10.1213/01.ane.0000287665.96156.7218165579 [Google Scholar] [CrossRef] [PubMed]
[7]. Lee A, Chui PT, Gin T, Educating patients about anaesthesia: A systemic review of randomized controlled trials of media-based interventionsAnaesth Analg 2003 96:1424-31.10.1213/01.ANE.0000055806.93400.9312707146 [Google Scholar] [CrossRef] [PubMed]
[8]. Spielberg CD, Sydeman SJ, State Trait Anxiety Inventory and State- Trait Anger Expression Inventory. In M.E. Maruish (Ed.). The use of psychological testing for treatment planning and outcome assessment 1994 :292-321. [Google Scholar]
[9]. Arellano R, Cruise C, Chung F, Timing of the anaesthetist’s preoperative outpatient interviewAnaesth Analg 1989 68(5):645-48.10.1213/00000539-198905000-00018 [Google Scholar] [CrossRef]
[10]. Dalal KS, Chellam S, Toal P, Anaesthesia Reference booklet: Is it better than a preoperative visitIndian J Anaesth 2015 59(8):511-13.10.4103/0019-5049.16299826379298 [Google Scholar] [CrossRef] [PubMed]