Early Childhood Caries (ECC) can be defined as the presence of one or more carious lesions, cavitated or not, in children up to five years of age. Presence of bacterial plaque, poor oral hygiene, frequency and time of consumption of beverages containing sugar are among the risk factors. Unfortunately, ECC has a major impact on the child’s quality of life, causing pain, early tooth loss, malnutrition, delayed growth and development, difficulty in chewing, speech problems, general health disorders and psychological problems. This paper presents a case report of a 3-year-old male patient, diagnosed with ECC and describes the therapeutic approach that ranges from effective measures to control caries activity, rehabilitative and restorative treatment, to changing of the eating habits and oral hygiene of the child.
Case Report
A 3-year-old (and 11 month) male child, with the complaint of multiple decayed teeth for a period of four months, presented for treatment in the Paediatric Dentistry Clinic, School of Dentistry of the Federal University of Rio Grande do Sul (UFRGS) Brazil. The patient’s mother complained that the child had many carious lesions and had spontaneous and provoked pain from eating and brushing. In the anamnesis and dietary diary, she reported that the patient drank from a sugared baby bottle twice a day and had the habit of eating sugary foods throughout the day. No significant past medical or dental family history was reported. Fluoride dentifrice was being used since the patient was two years of age. The family had a monthly income below the current minimum wage, representing a very low socioeconomic level.
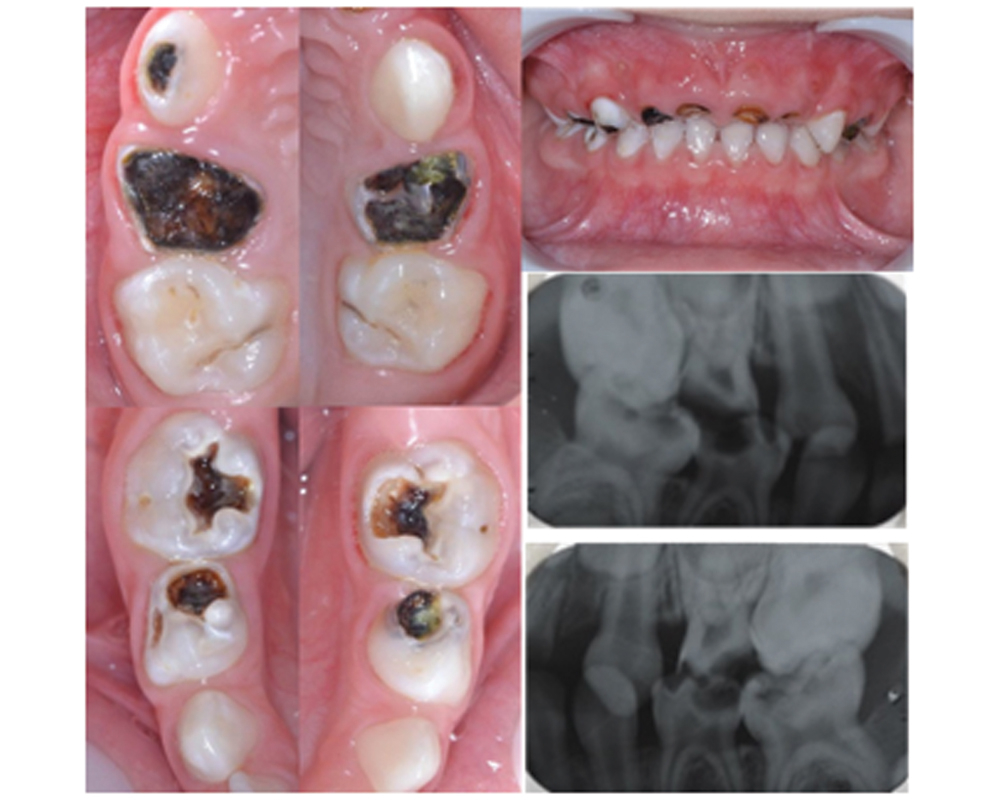
The clinical examination revealed an extensive carious coronal destruction in all the upper incisors, whitish-opaque rough spot lesions in enamel of the occlusal surface of teeth #55 and #65, soft cavity in dentin in tooth #53, and extensive coronal destruction of teeth #54 and #64 [Table/Fig-1]. In the mandibular arch, teeth #75, #74, #84 and #85 showed rough and opaque enamel breakdown and soft cavity in dentin, teeth #73 and #83 had whitish opaque rough spot lesions in enamel. The initial Visible Plaque Index (VPI) was 47% and the initial Gingival Blood Index (GBI) was 13% [1]. Radiographic examination also matched with the clinical diagnosis of ECC.
Preoperative intraoral photograph and radiograph showing early childhood caries destruction.
Initially, the proposed treatment was functional oral rehabilitation, starting with restorative treatment of cavitated lesions by selective caries removal technique for teeth #53, #54, #64, #74, #75, #84 and #85. For teeth #52, #51, #61 and #62, extraction and the installation of an upper fixed prosthesis with stock teeth were indicated. For the treatment of whitish opaque rough spot lesions in enamel, topical application of 1.23% fluoride gel was indicated over four weekly sessions. A treatment plan was developed and explained to the patient’s mother, who signed an approved informed consent form authorising the treatment as well as disclosure and publishing of this case report.
All procedures were performed under local anaesthesia, to avoid pain and discomfort, and rubber dam isolation was done in each quadrant in one session. Teeth #53, #75, #74, #84 and #85 were restored using the universal adhesive system (3M Espe®, Brazil) and composite resin Z350 (3M Espe®, Brazil) in WD, A1D and A1B colours. FluroShield resin sealant (Dentsply®, Brazil) was used on the occlusal surfaces of teeth #55 and #65 to block rough and opaque enamel breakdown. Teeth 54 and 64, were sealed with a cover of Resin Flow (3M Espe®, Brazil) in A1 colour, to re-establish the patient’s oral health condition. Due to the loss of vertical dimension of the patient, there was insufficient space to allow reconstruction with composite resin.
Extraction of root stumps of tooth no. #52, #51, #61 and #62 were performed under local anaesthesia in a single session. Two weeks after healing, an alginate impression was taken to obtain gypsum models to make an upper fixed prosthesis. Band pinching was done on teeth #55 and #65, commercially acrylic pontics were embedded in self-cured acrylic and a stainless-steel wire running from the anterior palatal surface was solded to the bands. The chosen colour was B1 of the Vita scale. The prosthesis was cemented with glass ionomer cement (Vitremer, 3M Espe®, Brazil) [Table/Fig-2,3 and 4].
Upper fixed prosthesis installed in anterior region.

Complete rehabilitation of maxillary arch.

Complete rehabilitation of mandibular arch.

After selective caries removal and restorations, regular application of 1.23% acidulated phosphate fluoride gel was performed once a week for one month, with one minute brushing, according to the manufacturer’s instructions. Concurrently, educational materials on diet and oral hygiene were given to the family. After the final examination, the patient was discharged and instructed to return after three months for monitoring. At follow up examination, the restorations as well as the prosthesis remained intact. No further carious lesions were detected. Patient was followed-up twice a year.
Discussion
Early childhood caries can be defined as the presence of one or more carious lesions, cavitated or not, in children up to five years of age [2,3]. It represents the result of an imbalance between multiple risk factors and protective factors that lead to pain, early dental loss, malnutrition, growth retardation, difficulty in chewing, speech problems, general health disorders and psychological problems. ECC also contributes to loss of self-esteem and future damage to the permanent dentition [4,5,6,7].
The aetiology of ECC is complex and involves interactions between social, behavioral and microbiological factors [8]. Moreover, the literature shows that the socioeconomic level of the family, such as low parental education and low monthly family income, are associated with the etiology and the higher prevalence of ECC [7,9,10]. The estimated monthly family income of the patient reported was less than minimum wage.
Through the anamnesis and dietary diary of the patient reported, a low-nutrient and high-frequency diet was observed regarding the intake of sugary foods and beverages, especially at night. The literature confirms that dietary practices are an important cause of ECC, specifically through the consumption of sugary drinks and a diet rich in sugars and starches [6,11].
The presence of bacterial plaque and poor oral hygiene, reflecting maternal knowledge of oral hygiene practices and oral hygiene behavior of the child, are factors associated with the risk for ECC [3]. The data presented in the literature was pertinent to the first clinical examination of the patient, where the visible plaque index was 47%.
The oral rehabilitation of this case was based on the patient’s age, cooperation during procedures and clinical findings. Some recent published case reports and studies have shown the use of strip crown, stainless-steel crown, resin or glass ionomer restoration, removable or fixed prosthesis as treatment options [12,13,14,15,16]. In this case, it was decided to start treatment with the selective caries removal due to the degree of coronal destruction. Systematic reviews support that there is no evidence to justify the total removal of carious tissue because of risk of increasing the chance of pulpal exposure [17]. For the opaque enamel breakdown, resinous sealant was used. The use is justified in the literature because there is no progression of blocked caries lesions when they are located in the outer half of the dentin [18]. For the upper first molars, a flowable resin was used. Due to the loss of vertical dimension of the patient, there was insufficient space to allow for reconstruction with composite resin. Alternatives such as stainless-steel crowns [12,13,14,16], resin filled celluloid crowns [13], and amalgam restorations [19] are available, but sealed with a cover of resin flow seemed to be the most advantageous choice for the present case. This was because there was no space to place other alternatives as described above. Probably, after re-establisment of the vertical dimension, other alternatives are possible.
Early decay in the anterior primary teeth may result in the development of parafunctional habits (tongue interposition and speech problems), aesthetic-functional problems such as malocclusion and space loss, and psychological problems that may interfere in the personality and behavioural development of the child [20,21]. It was for these reasons that the fixed prosthesis with commercially acrylic pontics were made.
Although, the removable space maintainer is most commonly employed [13,14], unfortunately, there are a number of drawbacks associated with its use, like dependency on the patient for success, the child may not wear it, accidental ingestion or aspiration, breakage and loss. Besides, a removable appliance may have a deleterious effect on the involved soft tissue and periodontium. As a result, the efficiency and effectiveness of the space maintainer could be compromised [21].
The use of fixed prostheses in children is limited by the arch modifications that result from the development of primary and mixed dentition occlusions. However, a period of stability exists in which a fixed appliance may be used. This period, when children are between the ages of 3 and 5.5 years, is the time in which the primary arch is completed and the sagittal and transverse dimensions are unaltered [22]. The use of fixed aesthetic space maintainers to replace a prematurely lost anterior tooth have also been tried previously [15]. The most commonly used technique involves the same technique described in this case report.
In the present case, the patient was almost 4-year-old, which represents an indicated and stable period to consider a fixed prosthesis. The patient would to be supervised continously twice a year, following the growth of the permanent incisors, until the time that the appliance could be removed. There is no need to construct a new prosthesis in the meantime, since growth changes will likely occur at six years of age and then the space maintainer will have to be removed.
Conclusion
Thus, prevention of early childhood caries should be an important public health goal. Providing guidance on healthy eating practices can reduce the occurrence of caries in early life. In addition, oral health programs should be established with a focus on mothers, caregivers, community health workers, preschool teachers and children.
[1]. Ainamo J, Bay I, Problems and proposals for recording gingivitis and plaqueInt Dent J 1975 25:229-35. [Google Scholar]
[2]. Kagihara LE, Niederhauser VP, Stark M, Assessment, management, and prevention of early childhood cariesJ Am Acad Nurse Pract 2009 21(1):01-10.10.1111/j.1745-7599.2008.00367.x19125889 [Google Scholar] [CrossRef] [PubMed]
[3]. Folayan MO, Kolawole KA, Oziegbe EO, Oyedele T, Oshomoji OV, Chukwumah NM, revalence and early childhood caries risk indicators in preschool children in suburban NigeriaBMC Oral Health. 2015 30:15-72.10.1186/s12903-015-0058-y26123713 [Google Scholar] [CrossRef] [PubMed]
[4]. Feldens CA, Vitolo MR, Drachler Mde L, A randomized trial of the effectiveness of home visits in preventing early childhood cariesCommunity Dent Oral Epidemiol 2007 35(3):215-23.10.1111/j.1600-0528.2006.00337.x17518968 [Google Scholar] [CrossRef] [PubMed]
[5]. Abbasoğlu Z, Tanboga I, Kuchler EC, Deeley K, Weber M, Kaspar C, Early Childhood Caries Is Associated with Genetic Variants in Enamel Formation and Immune Response GenesCaries Res 2015 49(1):70-77.10.1159/00036282525531160 [Google Scholar] [CrossRef] [PubMed]
[6]. Smith GA, Riedford K, Epidemiology of Early Childhood Caries: Clinical ApplicationJ Pediatr Nurs 2013 28(4):369-73.10.1016/j.pedn.2012.04.00522608944 [Google Scholar] [CrossRef] [PubMed]
[7]. Corrêa-Faria P, Martins-Júnior PA, Vieira-Andrade RG, Marques LS, Ramos-Jorge ML, Factors associated with the development of early childhood caries among Brazilian preschoolersBraz Oral Res 2013 27(4):356-62.10.1590/S1806-8324201300500002123780495 [Google Scholar] [CrossRef] [PubMed]
[8]. Feldens CA, Giugliani ERJ, Vigo A, Vítolo MR, Early Feeding Practices and Severe Early Childhood Caries in Four-Year-Old Children from Southern Brazil: A Birth Cohort StudyCaries Res 2010 44(5):445-52.10.1159/00031989820838043 [Google Scholar] [CrossRef] [PubMed]
[9]. Congiu G, Campus G, Luglie PF, Early Childhood Caries (ECC) Prevalence and Background Factors: A ReviewOral Health Prev Dent 2014 12(1):71-76. [Google Scholar]
[10]. Dos Santos Junior VE, De Sousa RM, De Caldas Junior MC, Rosenblatt AF, Early childhood caries and its relationship with perinatal, socioeconomic and nutritional risks: a cross-sectional studyBMC Oral Health 2014 6:14-47.10.1186/1472-6831-14-4724885697 [Google Scholar] [CrossRef] [PubMed]
[11]. Cidro J, Zahayko L, Lawrence HP, Folster S, McGregor M, McKay K, Breast feeding practices as cultural interventions for early childhood caries in Cree communitiesBMC Oral Health 2015 9:15-49.10.1186/s12903-015-0027-525888182 [Google Scholar] [CrossRef] [PubMed]
[12]. Doneria D, Thakur S, Singhal P, Chauhan D, Complete mouth rehabilitation of children with early childhood caries: A case report of three casesInt J Pedod Rehabil 2017 2(1):37-40.10.4103/ijpr.ijpr_2_17 [Google Scholar] [CrossRef]
[13]. Parisotto TM, De Souza-E-Silva CM, Steiner-Oliveira C, Nobre-dos-Santos M, Gaviãp MB, Prosthetic rehabilitation in a four-year-old child with severe early childhood caries: a case reportJ. Contemp Dent Pract 2009 10(2):90-97.10.5005/jcdp-10-2-9019279977 [Google Scholar] [CrossRef] [PubMed]
[14]. Cuadros Fernández C, Armengol Olivares A, Guinot Jimeno F, Lorente Rodríguez AI, Oral rehabilitation of a 4-year-old child with early childhood caries under general anaesthesia: a case report on long-term outcomeEur J Paediatr Dent 2014 15(2 Suppl):229-33. [Google Scholar]
[15]. Bhayade S, Rathi A, Wasnik M, Esthetic rehabilitation in young toddler-a case reportInt J Cur Adv Res 2016 5(5):936-37. [Google Scholar]
[16]. Mishra A, Pandey R, Pandey N, Jain E, A pedoprosthetic rehabilitation in patients with severe early childhood caries (S-ECC)BMJ Case Rep 2013 910.1136/bcr-2013-01026923843409 [Google Scholar] [CrossRef] [PubMed]
[17]. Casagrande L, Dalpian AK, Ardenghi TM, Zanatta FB, Balbinot CE, Garcia-Godoy F, Randomized clinical Trial of adhesive restorations in primary molars. 18-month resultsAm J Dent 2013 26(6):351-55. [Google Scholar]
[18]. Hesse D, Bonifacio CC, Mendes FM, Braga MM, Imparato JC, Raggio DP, Sealing versus partial caries removal in primary molars: a randomized clinical trialBMC Oral Health 2014 28:14-58.10.1186/1472-6831-14-5824884684 [Google Scholar] [CrossRef] [PubMed]
[19]. Parisotto TM, De Souza-E-Silva CM, Steiner-Oliveira C, Nobre-dos-Santos M, Gavião MB, Prosthetic rehabilitation in a four-year-old child with severe early childhood caries: a case reportJ Contemp Dent Pract 2009 10(2):90-97.10.5005/jcdp-10-2-9019279977 [Google Scholar] [CrossRef] [PubMed]
[20]. Sharma N, Passi S, Kumar VV, Multidisciplinary Approach to the Rehabilitation in Management of Child with Early Childhood Caries: A Case ReportJ Clin Diagn Res 2013 (10):2374-75.10.7860/JCDR/2013/5272.352824298533 [Google Scholar] [CrossRef] [PubMed]
[21]. Goenka P, Sarawgi A, Marwah N, Gumber P, Dutta S, Simple Fixed Functional Space MaintainerInt J Clin Pediatr Dent 2014 7(3):225-28. 10.5005/jp-journals-10005-127225709309 [Google Scholar] [CrossRef] [PubMed]
[22]. De Sant´anna GR, Guare Rde O, Rodrigues CR, Guedes-Pinto AC, Primary anterior tooth replacement with a fixed prosthesis using a precision connection system: a case reportQuintessence Int 2002 33(4):303-08. [Google Scholar]