Introduction
Problem solving skills are of utmost importance to medical students who in the future would depend on them for diagnosing a case. However, there are very few avenues to develop problem solving skills in the preclinical years. Generally, case scenarios are used by medical schools to develop these skills during Problem Based Learning (PBL) or Case Based Learning (CBL) sessions.
Aim
To build problem-solving skills by using analysis, reasoning and application. The experiment tests a novel digital mode to achieve these objectives.
Materials and Methods
This was a prospective cross-sectional study, conducted at Melaka Manipal Medical College (MMMC), Manipal Academy of Higher Education, Manipal, India, spanning over four months. MBBS students (n=81), in the first year of their curriculum, took part in the activity. Seven case scenarios were designed using PowerPoint 2013. Each case scenario was divided into case title, case history, clinical findings, investigations and treatment. The content and construct validity of the case scenarios was carried out by a clinician and changes were affected accordingly. The slides were placed in random order, forming a ‘potpourri’ and presented to the students through a Local Area Network (LAN) in the digital laboratory. They were asked to sort the slides and give a diagnosis for each case. Using google forms a questionnaire was prepared and this was used to collect feedback from students.
Results
Majority of students (85%) scored more than 72% marks in the activity. Marks obtained in arranging the slides did not correlate with marks obtained in diagnosis of the case. However, it is important to note that all students who got the diagnosis right had full marks in arranging the slides. The present study required students to recall and relate the facts which they had learnt during their entire year, apply it to the case and give a diagnosis which 74% of them found challenging. Though, most of the time they succeeded in bringing order to the ‘potpourri’, their success in achieving percipience was limited.
Conclusion
This novel experiment in using case scenarios on a digital platform offers many possibilities for testing and building skills essential for clinical practice. The fact that the activity was much appreciated by students, bolsters the faculty’s resolve to plan many more such innovations.
Introduction
The delivery of the medical curriculum in India, even today, follows largely the traditional method, with lectures occupying an eminent role. The Medical Council of India (MCI) restructured the curriculum vide a vision 2015 announcement to augment student’s exposure to innovative teaching learning methodologies like CBL and PBL [1,2]. However, the directive of the MCI has not been implemented to any significant extent in Indian medical schools [3]. The reasons being cited for the status quo in reforming curriculum delivery are many, being related to unpreparedness and resistance towards change from the stake holders, viz., students, teachers and the administration [3].
The MMMC, a constituent of the Manipal Academy of Higher Education, has dual advantages when it comes to experimentation in curriculum delivery. Most of the faculty are in the age group of 25 to 40 and are more amenable towards adopting new teaching and learning techniques. The management is very encouraging towards curricular innovations. The first year’s curriculum consists of three subjects, viz., anatomy, physiology and biochemistry which are divided into four blocks and taught with a system wise approach. The hybrid curriculum is delivered in the form of didactic lectures, practicals, PBL, self directed learning and CBL [4]. Of late, the institution has commissioned a digital laboratory which is widely used to conduct practical sessions and other teaching learning activities.
Though, active learning has many positive attributes, it does not happen unless the teacher takes the initiative to create an atmosphere for it [5]. The present study was planned with the intention of training individual students in problem solving using case scenarios, which addresses the skill set required by a physician to diagnose and treat a case, beginning with history taking and ending with the treatment strategy. Though, this study could be carried out using paper in the usual classroom setting, the digital laboratory was chosen to carry out this exercise. This we thought, would enable better visual impact in the form of text and graphics which would be incorporated into powerpoint slides and also would make the execution of the exercise less cumbersome [6]. Since, the present generation of medical students is computer-savvy, the digital interface we thought would provide amore comfortable experience.
Materials and Methods
This was a prospective cross-sectional study, conducted at MMMC, Manipal Academy of Higher Education, Manipal, India, spanning over four months from May to August, 2017. Ethics clearance was obtained from the Institutional Ethics Committee (IEC 333/2017). MBBS students in the 36th week of their 40 week curriculum in the first year, took part in the activity. Out of a class of 150 students, 81 students participated, subject to informed consent. The students were informed right in the beginning that the activity would not contribute any marks towards their internal assessment.
Ten case scenarios were designed using PowerPoint 2013. (https://drive.google.com/file/d/1W2V2lEmS3fEVvgKT7oTK3Qd3Ph5Awr2X/view?usp=sharing). While designing the case scenarios, care was taken not to make them too complex and incomprehensible for the first year MBBS students. Each case scenario was divided into the following headings: Case title, case history, clinical findings, investigations and treatment. The cases revolved around topics the students had learnt, but were not entirely the same in content as seen in their curriculum. They contained aspects mainly from anatomy, physiology, biochemistry along with traces of pathology, pharmacology and microbiology. They contained text, tables, as well as pictures relevant to the case. The case scenarios were presented to a professor of medicine, TMA Pai Hospital, MMMC, Manipal Academy of Higher Education, for validation. He was instructed to validate the case scenarios based on suitability of the title, accuracy of the clinical history, relevant clinical investigations and appropriate treatment strategy. He opined that the case scenarios were well designed according to the criteria for validation provided (as mentioned above) and were of a difficulty level suited for first year MBBS students. He recommended minor changes in the content using text boxes on the slides, which were then incorporated into the case scenarios. Each of the headings i.e., case title, case history, clinical findings, investigations and treatment was arranged in individual powerpoint slides. Thus, there were 50 slides in total corresponding to 10 case scenarios. The slides were placed in random order and presented initially to a faculty of the biochemistry department in an effort to decide the optimum time to be given to students for solving them. The first year curriculum allowed only an hour’s time to conduct the activity. Since, it was found that solving 10 cases would be a difficult task in a span of an hour, it was decided to administer only seven case scenarios to the students, with their content divided between 35 slides as mentioned above. Google forms (an online application from Google) was used to prepare a questionnaire (Cronbach’s alpha=0.83) with 12 items on a Likert scale with responses graded from strongly agree (five points) to strongly disagree (one point) [Table/Fig-1]. This was validated by medical educationists of the institution, for the attributes of the activity which addressed learning and the ease of taking part in the activity and was used to collect feedback from the students.
Results of the questionnaire given to students.
| S. No. | Questionnaire | Strongly agree (5) | Agree (4) | Neutral (3) | Disagree (2) | Strongly disagree (1) |
|---|
| 1 | The activity was interesting | 75 | 3 | 3 | - | - |
| 2 | The activity promoted active learning | 70 | 9 | 2 | - | - |
| 3 | The activity made us correlate different aspects of a case scenario and give a diagnosis | 74 | 3 | 4 | - | - |
| 4 | Helped build problem solving skills | 69 | 8 | 4 | - | - |
| 5 | Helped activate prior knowledge | 70 | 2 | 9 | - | - |
| 6 | Improved clinical orientation to the curriculum | 72 | 9 | - | - | - |
| 7 | Integrated subjects of the first year | 75 | 6 | - | - | - |
| 8 | The activity was well planned | 75 | 6 | - | - | - |
| 9 | Exposed to aspects of the disease not dealt with in the class room | 74 | 7 | - | - | - |
| 10 | The difficulty level was adequate for first year medical students | 60 | 11 | 10 | - | - |
| 11 | The activity was comfortable to be executed on the computer | 74 | 7 | - | - | - |
| 12 | Allotted time was adequate | 78 | 3 | - | - | - |
*The numbers indicate the number of students who responded to each one of the items in the questionnaire. For calculating the collective opinion of students, the strongly agree and agree were clubbed together and expressed as a percentage
The students were divided into two batches and took part in the activity in sequence. Each one of them was seated at a computer terminal which was connected by ethernet LAN to the master computer. The IT expert in the digital laboratory was involved in planning and execution of the study. He sent a powerpoint file consisting of seven cases scenarios from the master computer to all the computer terminals. The students were instructed as follows:
There are a total of 35 slides in a powerpoint file named ‘potpourri’ in a folder by name ‘Biochem’ on the desktop. Copy the powerpoint file onto the desktop. The slides in the file are in random order. After opening the file, go to the slide sorter view and first identify seven case titles, viz., 1) A dizzy diabetic; 2) Turning yellow; 3) Puffy young boy; 4) The drinking problem; 5) Thyroid blues; 6) A congenital heart anomaly; 7) Bruising and bleeding. Arrange the case title slides in the increasing order of their number in a new powerpoint presentation named with your roll number.
Go through the remaining slides in the slide sorter view and start arranging them below their respective titles in the order of case history, clinical findings, investigations and treatment by copying and pasting them. The case title should match the other components of the case.
Once all the components of the case scenarios have been aligned in the right order, write the diagnosis for each case in a separate slide after the slide entitled ‘treatment’ in every case. Thus, seven more slides will be added by you to the presentation.
Save the file thus created.
You have one hour to complete the task.
After this, a small questionnaire will appear on your desktop to collect your opinion on this activity [Table/Fig-1]. Please answer according to the options provided and submit the questionnaire.
The slides and the responses to the questionnaire submitted by the students were automatically saved in the master computer from where they were retrieved for further analysis. Each correctly assembled case scenario with the correct diagnosis was given 10 marks, i.e., seven marks for correctly arranging the slides in sequence (1.4 marks for each slide arranged correctly in sequence and three more for the correct diagnosis). Thus, the powerpoint file from each student carried a maximum of 70 marks.
Results
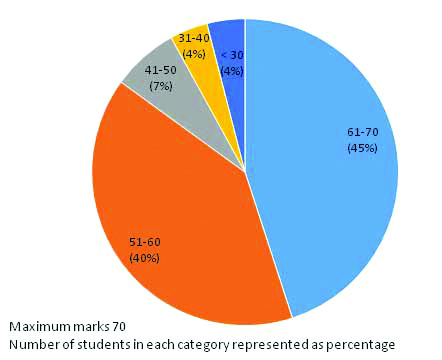
As shown in [Table/Fig-2], maximum number of students (85%) scored between 51-70 marks in the activity. Correlation of marks obtained in arranging the slides in appropriate order to the marks obtained in the diagnosis yielded r-values in the range 0.1 to 0.4 for the seven different case scenarios in the activity. Percentage of students who got zero marks in diagnosis inspite of arranging the slides in the right order ranged from 14% to 73% in the seven cases administered. However, it is important to note that all students who got the diagnosis right had full marks in arranging the slides.
Marks obtained by the students in the activity.
Correlation of aggregate marks obtained in the previous three internal assessment examinations (theory component) by all the students (n=81) to the marks obtained in the activity was weak (r=0.14). Students who scored the highest marks (between 801-900 i.e., distinction marks) in the internal assessment examinations showed a better correlation (r=0.3) than students who scored lower.
When the aggregate marks of internal assessment examinations were correlated with the marks obtained for correct diagnosis, it was found that students who had marks in the range 801-900, showed a better correlation with the seven case scenarios (r=0.4-0.7) when compared to students who had scored below 800 (r=0.01-0.2).
In all the seven case scenarios, the marks obtained for arranging the slides was above 90%. However, the marks obtained in diagnosis varied widely from 22%-78%. Thus, the marks obtained in diagnosis were consistently lower than the marks obtained in arranging the slides.
Student feedback was collected using a 5 point Likert scale which was graded from strongly agree (five points) to strongly disagree (one point). As shown in [Table/Fig-1], more than 87% of students were in agreement with positive attributes of the activity. The students were affirmative that the activity promoted active learning in an integrated format. They also felt that it helped build problem solving skills which are most important to medical students. When asked for additional suggestions to improve the activity, they strongly reiterated that more activities like this should be conducted in every block to ensure that students learn to analyse cases. They also wanted such activities for future batches of students.
Discussion
It is well known that properly designed computer-assisted activities promote the self directed approach in the student that encourages deep, retentive learning [7]. It also offers unique presentational opportunities to teachers, in that, learning material in different media can be integrated. The study can be designed using text, graphics, sound and moving images which cause inputs via multiple senses [8,9]. Though, majority (85%) of the students scored more than 50 out of 70 marks in the study, closer analysis reveals a few important findings. It is obvious that the present study required students to recall and relate the facts which they had learnt during their entire year, apply it to the case and give a diagnosis. Hence, it is no surprise that students who had scored extremely well in the theory component of the curriculum, fared better than those who did not. The fact that all students who got the diagnosis right in all cases had arranged the slides in the right order emphasises the importance of following the right procedure while investigating a case or a patient. Wrong diagnosis given by students inspite of arranging the slides correctly, may be attributed to poor ability to recall and apply knowledge. This may also be due to the fact that all the topics chosen for designing the case scenarios had aspects of the disease not dealt within their curriculum. This might have added a quantum of confusion to their reasoning. It is also possible that these students might be those who depended more on rote learning rather than understanding the concepts [10]. From the teachers perspective, it was opined that the study fulfilled the objectives with which it was planned. They felt that the students performance in the study was commendable in the first part of the study which involved arranging the slides, which tested the skill set of correlating the case history with relevant clinical and laboratory investigations, culminating in the treatment. They also felt that key clinical investigations could have been highlighted to draw the attention of the students, so as to improve their performance in the diagnosis component. Though, designing the case scenarios according to the needs of the first year MBBS students was time consuming, other aspects involved in executing the study were quite speedy and enjoyable.
Conclusion
Though, the cream of the class (based on performance in theory examinations) did splendidly well in aligning the components of the case scenarios and giving the right diagnosis, achieving percipience was not possible for majority of students because of inability to apply their knowledge in diagnosing the cases. These students need to reorient their learning strategies towards deeper understanding and it is necessary to sensitise the teachers to help them achieve this goal. They also need to be exposed to more activities of this type to improve their problem solving skills. This study was a unique attempt to test problem solving skills using the digital mode. It is recommended that such activities be included in the formative assessment of students, which in the context of medical education in India, would move the curriculum towards the directives of the MCI stated in the vision 2015 document. The fact that students themselves requested for more such activities, 38 is encouraging for the faculty and may lead to more such innovations in building and testing problem solving skills.
*The numbers indicate the number of students who responded to each one of the items in the questionnaire. For calculating the collective opinion of students, the strongly agree and agree were clubbed together and expressed as a percentage
[1]. Vision 2015, Medical Council of India. Available at: http://www.mciindia.org/announcement/MCI_booklet.Pdf (last accessed on: 09 October 2013) [Google Scholar]
[2]. Ali SS, Mittal R, Problem-based learning in Indian medical educationAnn Health Health Sci 2014 1(1):01-04.10.5958/j.2322-0422.1.1.001 [Google Scholar] [CrossRef]
[3]. Shrivastava SR, Shrivastava PS, Ramasamy J, Problem-based learning in undergraduate medical curriculum: an Indian perspectiveArch Med Health Sci 2013 1(2):200-01.10.4103/2321-4848.123057 [Google Scholar] [CrossRef]
[4]. Roche M, Adiga IK, Akshatha Nayak G, PBL trigger design by medical students: an effective active learning strategy outside the classroomJ Clin Diagn Res 2016 10(12):JC06-08.10.7860/JCDR/2016/21813.901528208882 [Google Scholar] [CrossRef] [PubMed]
[5]. Bonwell CC, Eison JA, Active learning: creating excitement in the classroom, ASHE-ERIC higher education report no.1 1991 Washington, DCeorge Washington University:1-21. [Google Scholar]
[6]. Kember D, Leung D, The influence of active learning experiences on the development of graduate capabilitiesStudies in Higher Education 2005 30(2):155-70.10.1080/03075070500043127 [Google Scholar] [CrossRef]
[7]. Diederen J, Gruppen H, Hartog R, Voragen A, Design and evaluation of digital learning material to support acquisition of quantitative problem-solving skills within food chemistryJ Sci Educ Technol 2005 14(5/6):495-507.10.1007/s10956-005-0224-0 [Google Scholar] [CrossRef]
[8]. Hemmi, Bayne S, The appropriation and repurposing of social technologies in higher educationJournal of Computer Assisted Learning 2009 25(1):19-30.10.1111/j.1365-2729.2008.00306.x [Google Scholar] [CrossRef]
[9]. Voge C, Hirvela K, Jarzemsky P, The (digital) natives are restless designing and implementing an interactive digital media assignmentNurse Educ 2012 37(2):56-61.10.1097/NNE.0b013e3182461b2e22327525 [Google Scholar] [CrossRef] [PubMed]
[10]. Mayer RE, Rote versus meaningful learningTheory Into Practice 2002 41(4):226-32.10.1207/s15430421tip4104_4 [Google Scholar] [CrossRef]