Duplicated RCA with Anomalous Origin of Left Circumflex Artery: A Rare Case Report
Pawan Kumar Garg1, Pushpinder Singh Khera2, Swarnava Tarafdar3, Binit Sureka4, Surender Deora5
1 Assistant Professor, Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
2 Additional Professor, Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
3 Senior Resident, Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
4 Assistant Professor, Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
5 Assistant Professor, Department of Cardiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Swarnava Tarafdar, 17E/361A, Chopasani Housing Board, Jodhpur-342008, Rajasthan, India.
E-mail: dr.tarafdarswarnava@gmail.com
Coronary artery anomalies are found in around 1-2% of patients undergoing coronary angiography. Uncovering of more coronary anomalies has increased with increase in awareness and easy availability of non invasive Computed Tomography Coronary Angiography (CTCA). We present a rare case of a 64-year-old female with a history of atypical chest pain and mild ST depression ECG changes who underwent CTCA. The present case revealed unusual findings of an anomalous origin of the Left Circumflex Coronary artery (LCx) from the proximal Right Coronary Artery (RCA) with duplicated right coronary artery after arising as a common trunk from right coronary cusp. In the present case report we attempted to highlight the rarity of this coronary anomaly.
Common trunk, Coronary angiography, Coronary anomalies, Right coronary artery
Case Report
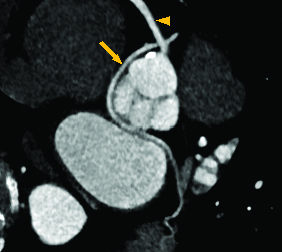
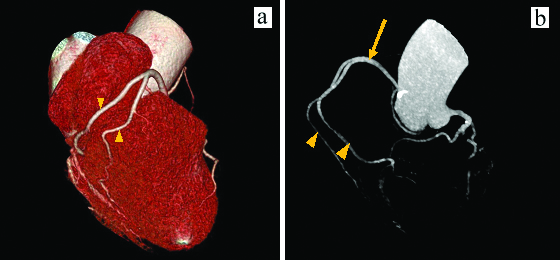
A 64-year-old female was admitted to the hospital with a recent history of chest pain and giddiness. She had no specific medical history. However, she had a history of diabetes mellitus and also a positive family history of premature atherosclerotic heart disease. On physical examination, cardiac and lung auscultation findings were normal. The chest X-ray findings were normal. Routine laboratory tests were nonspecific. The electrocardiogram revealed mild depression of ST in the leads of the inferior wall. She underwent CTCA to evaluate coronary artery disease. The CTCA was obtained in "Dual source 2×128 slice multi-detector CT machine" using retrospective ECG-gating with the administration of 80 mL of non ionic contrast at the rate of 5.5 mL/second. In the present patient, the LCx showed anomalous origin from the RCA with retroaortic course without significant compression or luminal narrowing was seen [Table/Fig-1]. The RCA shows duplication after common trunk of 4.5 cm arising from right coronary cusp [Table/Fig-2]. In addition no other haemodynamically significant abnormality was seen. The patient was later managed conservatively as the anomaly was not malignant and no haemodynamically significant stenosis was seen in the coronary arteries on CTCA.
Anomalous origin of LCx (arrow) from right coronary artery (arrow head) with retroaortic course.
Duplication of RCA (arrow head) after a common trunk (arrow) arising from right coronary cusp.
Discussion
The prevalence of coronary artery anomalies is usually cited as 1-2% of the general population [1,2]. Coronary artery anomalies are divided into haemodynamically significant anomalies (commonly associated with shunting, ischaemia or sudden cardiac death) and anomalies that are not haemodynamically significant. Atresia, interarterial course, origin from pulmonary artery and congenital fistula are considered to be haemodynamically significant anomalies. On the other hand duplication, origin from the aorta in an anomalous position which includes arteries that arise from the contralateral cusp or contralateral artery which takes a prepulmonic, transseptal or retroaortic course, high origin from aorta, origin from other systemic vascular structures, shepherd’s crook RCA and systemic termination are haemodynamically insignificant coronary anomalies [3]. Ectopic origin of the LCx is the most common coronary anomaly and can be found in around 0.37-0.7% of patients. The anomalous LCx most commonly arises from a separate ostium within the right sinus or as a proximal branch of the RCA [4,5]. The retroaortic LCx usually passes into the space between the posterior aorta (the noncoronary cusp) and the interatrial septum [6]. In anomalous origin of LCx, patients may develop coronary symptoms due to kinking or compression in their retroaortic course. However, in addition to this, duplication of RCA was also evident in the present case, whose association is a rarer variant and only few cases are reported [7,8]. Although, the anomaly being benign and asymptomatic, few cases of sudden death, myocardial infarction and angina pectoris have been reported [9]. Incomplete treatment can result from an insufficient knowledge of the existence of double RCA before any invasive procedure as if only one artery is catheterised during angiography and patient having coronary atherosclerotic disease in the other artery [10]. The double RCA anomaly is seen mainly in males, though the present patient was female [11]. Barthe JE et al., reported for the first time about double RCA anomaly. They observed double RCA originating from single ostium with the vessels within right atrioventricular groove. They reported that after the origin of the conus artery and a ventricular branch, the most anterior RCA descended towards the acute margin of the heart and terminated in a small Posterior Descending Artery (PDA) and the second RCA terminated in a small PDA and in posterolateral branches [12]. However, in the present case both right coronary arteries were originating from a common trunk which was arising from right coronary cusp, both were almost identical in size and both gave rise to a PDA. A classification of double RCA has been given by a Turkish author where most of the studies concerning anomaly have been reported and present anomaly falls in class G2 [13]. To our knowledge no G2 atypical double RCA associated with anomalous origin of LCx has been reported till date.
Conclusion
An anomalous origin of the LCx coronary artery with duplication of RCA is an extremely rare entity. The CTCA has become the standard of reference for evaluation of coronary artery anomalies over more invasive catheter angiography and therefore presently the primary modality for evaluation of coronary anomalies.
[1]. Fujimoto S, Kondo T, Orihara T, Sugiyama J, Kondo M, Kodama T, Prevalence of anomalous origin of coronary artery detected by multi-detector computed tomography at one centerJ Cardiol 2011 57(1):69-76.10.1016/j.jjcc.2010.10.00621146363 [Google Scholar] [CrossRef] [PubMed]
[2]. Frescura C, Basso C, Thiene G, Corrado D, Pennelli T, Angelini A, Anomalous origin of coronary arteries and risk of sudden death: a study based on an autopsy population of congenital heart diseaseHum Pathol 1998 29(7):689-95.10.1016/S0046-8177(98)90277-5 [Google Scholar] [CrossRef]
[3]. Shriki JE, Shinbane JS, Rashid MA, Hindoyan A, Withey JG, DeFrance A, Identifying, characterizing, and classifying congenital anomalies of the coronary arteriesRadiographics 2012 32(2):453-68.10.1148/rg.32211509722411942 [Google Scholar] [CrossRef] [PubMed]
[4]. Rozenman Y, Schechter D, Gilon D, Gotsman MS, Anomalous origin of the circumflex coronary artery from the right sinus of Valsalva as a cause of ischemia at old ageClin Cardiol 1993 16(12):900-01.10.1002/clc.49601612138168277 [Google Scholar] [CrossRef] [PubMed]
[5]. Levin DC, Fellows KE, Abrams HL, Haemodynamically significant primary anomalies of the coronary arteries. Angiographic aspectsCirculation 1978 58(1):25-34.10.1161/01.CIR.58.1.25348342 [Google Scholar] [CrossRef] [PubMed]
[6]. Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N, Primary congenital anomalies of the coronary arteries: a coronary: arteriographic studyInt J Cardiol 2000 74(1):39-46.10.1016/S0167-5273(00)00243-6 [Google Scholar] [CrossRef]
[7]. Young Hyman PJ, Tommaso CL, Singleton RT, A new double coronary artery anomaly: the right coronary artery originating above the coronary sinus giving off the circumflex arteryJ Am Coll Cardiol 1984 4:1329-31.10.1016/S0735-1097(84)80159-X [Google Scholar] [CrossRef]
[8]. Garg N, Goel PK, Sinha N, Double right coronary artery with anomalous left main and septal arteries originating from the right coronary sinusIndian Heart J 2002 54(4):428-31. [Google Scholar]
[9]. Corrado D, Penelli T, Piovesana P, Thiene G, Anomalous origin of the left circumflex coronary artery from the right aortic sinus of Valsalva and sudden deathCardiovasc Pathol 1994 3(14):269-71.10.1016/1054-8807(94)90013-2 [Google Scholar] [CrossRef]
[10]. Kheirkhah J, Habibifar A, Moladoust H, A case of double right coronary artery with separate ostiumJ Tehran Heart Cent 2014 9(3):135-36. [Google Scholar]
[11]. Misuraca L, Rutigliano D, Pestrichella V, Contegiacomo G, Balbarini A, A very rare congenital abnormality: double right coronary artery: A case reportJ Cardiovasc Med 2009 10(8):643-45.10.2459/JCM.0b013e32832ce97d19455049 [Google Scholar] [CrossRef] [PubMed]
[12]. Barthe JE, Benito M, Sala J, Houbani AJ, Quintana E, Esplugas E, Double right coronary arteryAm J Cardiol 1994 73(8):62210.1016/0002-9149(94)90352-2 [Google Scholar] [CrossRef]
[13]. Vural M, Suggestions for definition and classification of double right coronary artery, which is frequently seen in Turkey despite its rarity in the literatureAnadolu Kardiyol Derg (Turkish) 2008 8(4):303-04. [Google Scholar]