Gender Specific Knee Replacement-Do Indian Females Need It
V Senthil Jayapal1, Karthick Anand2, Saravanan Ananda Kumar3
1 Consultant Surgeon, Department of Orthopaedics, G Viswanatham Hospital, Trichy, Tamil Nadu, India.
2 Assistant Professor, Department of Orthopaedics, Sri Venkateshwaraa Medical College and Research Centre, Puducherry, India.
3 Consultant, Department of Orthopaedics, ABC Hospital, Trichy, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Karthick Anand, A2, Harmony Appartment, Avvai Street, Gorimedu-605006, Puducherry, India.
E-mail: karthick13985@gmail.com
Introduction
Total knee replacement is a revolutionary procedure aimed at relieving pain improving knee function and the quality of life, Indian women are more prone for osteoarthritis and recent researches have led on to manufacturing implants specific to their anatomy to achieve the above mentioned goals.
Aim
The study aimed at analysing whether these modifications in the newly designed gender specific implants translate to any additional significant improvement in functional outcome in comparison to the commonly used traditional knee implants.
Materials and Methods
It was a prospective comparative study done in 30 knees of 30 women patients aged between 55-70 years in GV Hospital, Trichy, India between July 2011-January 2013. A total of 15 patients (Group B) had Zimmer Legacy Posterior Stabilized (LPS) knee implant and the other 15 (Group A) had Zimmer gender specific knee implants. Patients were followed up for 24 months post surgery, preoperative and postoperative data were recorded according to the knee society scoring system. All the patients were operated by standard anterior midline incision by a single surgeon and underwent the same postoperative protocol.
Results
The average age in Group A was 59.93 and in group B was 59.4. The mean preoperative Knee Score (KS) and Functional Score (FS) was 50.2 and 49.3 in Group A and B respectively. The range of motion increased following surgery in all patients but there was no statistically significant difference noted between the two groups. The postoperative KS and FS were assessed at 6 weeks, 3 months, 6 months, 12 months and 24 months and statistical significance using Student’s t-test, on SPSS 13.0 (SPSS Inc., Chicago, Illinois) was done during each follow up. There was no statistical significant difference in KS and FS between the groups at the end of 24 months.
Conclusion
Based on the results of our study we found no significant advantage of using gender specific implants oriented to female knees. Our study shows the goal of the design of the gender-specific high-flexion knee prosthesis has not been achieved.
Functional score, Implant design, Knee replacement, Knee score
Introduction
Knee replacement implants of different types have evolved over the years with the aim of achieving good patient outcomes and increased longevity of the implants [1]. The concept that implants specifically matching the anatomy of females will help achieving the above mentioned goals led on to the development of gender specific knee implants [2,3]. There is paucity of literature among Indian women about the real benefit of these implants. Indian women expect implants with maximal longevity allowing a high functional activity like squatting and sitting cross legged. Theoretically a gender specific knee implant distinctively matching the anatomy of the female knees should help them fulfill these expectations [3-5]. These implants have been in use in western and other developed nations since 2005 with studies showing no obvious benefits of them. Our study was carried out to find whether the aim was achieved in women operated for primary osteoarthritis of knee as there is no literature from India.
The gender specific knee replacement implant was defined as an implant matching the narrow mediolateral diameter for any given anteroposterior dimension of the female knee with increased angle of trochlear groove and decreased anterior flange thickness and width [5-7]. Our study analyses whether the gender specific implants offer any additional functional outcome improvements in comparison to the commonly used traditional knee implants.
Materials and Methods
It was a prospective comparative study conducted in GV hospital, Trichy, India from June 2011 to January 2013 in 30 knees of 30 women. In 15 knees, Zimmer gender specific knee replacement implants was used and among the rest 15, Zimmer traditional LPS knee implants was used. Patient randomly choose the implants by picking from the lots and were grouped into A and B [Table/Fig-1].
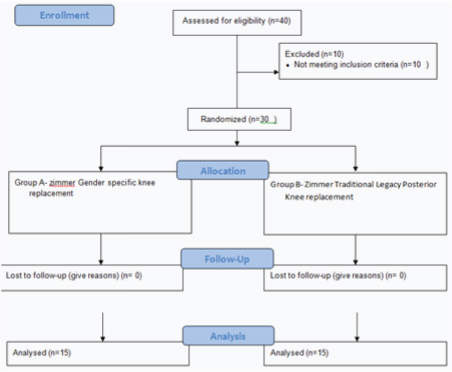
Group A was women with gender specific implants and Group B was women with traditional LPS implants. After obtaining the local ethical committee approval and informed written consent from the patient surgery was performed. We included only primary osteoarthritis of the knee.
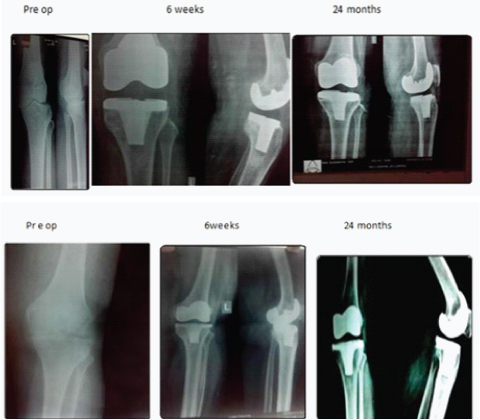
Preoperative and postoperative outcomes were recorded according to the old Knee Society System (KSS) [8]. The knee society scoring system consists of two parts a KS and FS. All the patients were operated by standard anterior midline incision and underwent the same postoperative protocol. X-rays of the knee AP and lateral were taken in the immediate postoperative patients [Table/Fig-2].
Preoperative and postoperative radiographic evaluation.
Group A: Gender specific knee
Group B: LPS knee
There were no patients lost to follow-up. We excluded conditions which could adversely affect the postoperative outcome like preoperative complex knee deformity, bone defects requiring grafting and additional screw fixation. The patients were followed up at 6 weeks, 3 months, 6 months, 12 months and 24 months. We also assessed any statistical significance within each group between 6 and 12 months and between 12 and 24 months follow-up. At each follow-up the knee society scoring and X-rays of the knee were taken (none of the patients were excluded but they had lower outcome scores). A KS and FS score in range of 80-100 was considered an excellent outcome.
Statistical Analysis
Statistical analysis was done using non parametric unpaired t-test, on SPSS 13.0 (SPSS Inc., Chicago, Illinois). A p-value <0.05 was taken as significant.
Results
The average age in Group A was 59.93 years and in Group B was 59.4 years. We operated in 17 right sided knees and 13 left sided knees. The mean KS and FS preoperative in Group A was 50.2 and 49.3 respectively. The average range of motion was 85 degrees in Group A and 88 degrees in Group B. The average postoperative range of motion was 115.3 degrees in Group A and 115 degrees in Group B. The postoperative KS and FS were assessed at 6 weeks, 3 months, 6 months, 12 months and 24 months and tabulated [Table/Fig-3,4].
Postoperative Knee Score (KS) of Knee scoring system.
| Time period | Knee score |
|---|
| GS mean (SD) | LPS mean (SD) | p-value |
|---|
| 6 Weeks | 81.60 (5.77) | 81.8 (6.05) | 0.90 |
| 3 Months | 87.40 (3.89) | 89.3 (1.86) | 0.09 |
| 6 Months | 88.53 (4.69) | 90.13 (2.56) | 0.24 |
| 12 Months | 92.00 (3.13) | 93.00 (2.10) | 0.29 |
| 24 Months | 94.6 (1.00) | 93.8 (2.89) | 0.38 |
GS-Gender specific knee implant, LPS- Legacy Posterior Stabilised
Postoperative Functional Score (FS) of knee scoring system.
| Time period | Functional Score | p-value |
|---|
| GS mean (SD) | LPS mean (SD) |
|---|
| 6 Weeks | 63.3 (4.88) | 66.0 (7.37) | 0.25 |
| 3 Months | 76 (9.86) | 76 (9.86) | 1.00 |
| 6 Months | 87.3 (7.04) | 86 (5.07) | 0.55 |
| 12 Months | 89.09 (8.31) | 91.8 (4.05) | 0.33 |
| 24 Months | 93.3 (5.77) | 98.0 (4.47) | 0.24 |
GS-Gender specific knee implant, LPS- Legacy Posterior Stabilized
Within both the groups, there was statistically significant results in both knee and functional scores between 6 months and 12 months follow-up [Table/Fig-5]. There were no statistically significant difference in both knee and functional scores within the groups between 12 and 24 months follow-up. There was no statistically significant difference in the functional outcome between traditional knee (LPS) and gender specific knee arthroplasty at 24 months follow-up.
Comparison of KSS within GS group at 6 and 12 months.
| Group | 6 Months Mean (Sd) | 12 MonthsMean (Sd) | p-value |
|---|
| GS* | KS‡ | 88.5 (4.69) | 92 (3.13) | 0.002 |
| FS§ | 87.3 (7.04) | 9.0 (8.31) | 0.022 |
| LPS† | KS | 90.1 (2.56) | 93 (2.10) | 0.001 |
| FS | 86 (5.07) | 91.5 (4.05) | 0.003 |
*GS-Gender specific knee implant. †Legacy posterior stabilizing. ‡Knee score. §functional score.
Discussion
There has been a constant debate on whether improving the anatomic fit of knee implants will translate to clinical improvement in patients postoperatively, bearing this in mind implant companies started designing implants exactly matching to the female distal femur [9-11].
There is no study in Indian population to decide the advantage of gender specific implants. Few western studies [12,13] assessed the implant design and the outcome of it in improving the postoperative range of motion. In our study, the mean postoperative range of flexion in the gender-specific prosthesis was 115.7 degrees, range (105-125 degrees) and in the traditional prosthesis it was 115 degrees (100-120 degrees) suggesting no gross difference in the range of motion due to the differences in implant design. The results are similar and comparable to the available western literature [12-14].
The other change in trochlear groove which theoretically reduces the rate of any patellar subluxation was highlighted as a prominent change in these implants but our study showed no benefit of such change as none of the patients in any group had patella subluxation [7,14,15].
All patients in our study showed increased functional outcomes irrespective of the implants and there was no implant related complication over the two-year follow-up. The results of our study in Indian women were similar to results of other studies done in western population [9,14].
Limitation
A small sample size with midterm follow-up.
Conclusion
Based on our study, the goal of design modification has not been attained as there was no statistically significant difference in the functional outcome between traditional knee (LPS) and gender specific knee arthroplasty at 24 months follow-up. Whatever be the implant, a meticulous surgery will only yield the best possible functional outcome.
GS-Gender specific knee implant, LPS- Legacy Posterior Stabilised
GS-Gender specific knee implant, LPS- Legacy Posterior Stabilized
*GS-Gender specific knee implant. †Legacy posterior stabilizing. ‡Knee score. §functional score.
[1]. Rankin AE, Bostrom M, Hozack W, Jacobs J, McCarthy J, O’Connor M, Gender-specific knee replacements: a technology overviewJ Am Acad Orthop Surg 2008 16(2):63-67.10.5435/00124635-200802000-00003 [Google Scholar] [CrossRef]
[2]. Booth RE Jr, Sex and total knee: gender-sensitive designsOrthopaedics 2006 29(9):768-69.10.3928/01477447-20060901-2817004583 [Google Scholar] [CrossRef] [PubMed]
[3]. Chin KR, Dalury DF, Zurakowski D, Scott RD, Intraoperative measurements of male and female distal femurs during primary total knee arthroplastyJ Knee Surg 2002 15(4):213-17. [Google Scholar]
[4]. Conley S, Rosenberg A, Crowninshield R, The female knee: anatomic variationsJ Am Acad Orthop Surg 2007 15(Suppl 1):S31-36.10.5435/00124635-200700001-0000917766787 [Google Scholar] [CrossRef] [PubMed]
[5]. Csintalan RP, Schutz MM, Woo J, McMahon PJ, Lee TQ, Gender differences in patellofemoral joint biomechanicsClin Orthop Relat Res 2002 402:260-69.10.1097/00003086-200209000-0002612218492 [Google Scholar] [CrossRef] [PubMed]
[6]. Berger RA, Crossett LS, Jacobs JJ, Rubash HE, Malrotation causing patellofemoral complications after total knee arthroplastyClin Orthop Relat Res 1998 (356):144-53.10.1097/00003086-199811000-000219917679 [Google Scholar] [CrossRef] [PubMed]
[7]. Gillespie RJ, Levine A, Fitzgerald SJ, Kolaczko J, DeMaio M, Marcus RE, Gender differences in the anatomy of the distal femurJ Bone Joint Surg Br 2011 93(3):357-63.10.1302/0301-620X.93B3.2470821357958 [Google Scholar] [CrossRef] [PubMed]
[8]. Insall J, Dorr L, Scott R, Norman W, Rationale of the Knee Society clinical rating systemClin Orthop Relat Res 1989 (248):13-14.10.1097/00003086-198911000-00004 [Google Scholar] [CrossRef]
[9]. Mahoney OM, Kinsey T, Overhang of the femoral component in total knee arthroplasty: risk factors and clinical consequencesJ Bone Joint Surg Am 2010 92(5):1115-21.10.2106/JBJS.H.0043420439656 [Google Scholar] [CrossRef] [PubMed]
[10]. Pierson JL, Ritter MA, Keating EM, Faris PM, Meding JB, Berend ME, The effect of stuffing the patellofemoral compartment on the outcome of total knee arthroplastyJ Bone Joint Surg Am 2007 89(10):2195-203.10.2106/JBJS.E.0122317908896 [Google Scholar] [CrossRef] [PubMed]
[11]. Woodland L, Francis R, Parameters and comparisons of the quadriceps angle of college-aged men and women in the supine and standing positionsAm J Sports Med 1992 20(2):208-11.10.1177/0363546592020002201558251 [Google Scholar] [CrossRef] [PubMed]
[12]. Thomsen M, Husted H, Bencke J, Curtis D, Holm G, Troelsen A, Do we need a gender-specific total knee replacement? A randomised controlled trial comparing a high-flex and a gender-specific posterior designJ Bone Joint Surg Br 2012 94(6):787-92.10.1302/0301-620X.94B6.2878122628593 [Google Scholar] [CrossRef] [PubMed]
[13]. Johnson AJ, Costa CR, Mont MA, Do we need gender-specific total joint arthroplasty?Clin Orthop Relat Res 2011 469(7):1852-58.10.1007/s11999-011-1769-221264555 [Google Scholar] [CrossRef] [PubMed]
[14]. Kim YH, Choi Y, Kim JS, Comparison of standard and gender-specific posterior-cruciate-retaining high-flexion total knee replacements: a prospective, randomised studyJ Bone Joint Surg Br 2010 92(5):639-45.10.1302/0301-620X.92B5.2412920435999 [Google Scholar] [CrossRef] [PubMed]
[15]. Hitt K, Shurman JR, Greene K, McCarthy J, Moskal J, Hoeman T, Anthropometric measurements of the human kneeJ Bone Joint Surg Am 2003 85-A(Suppl 4):115-22.10.2106/00004623-200300004-00015 [Google Scholar] [CrossRef]