Fracture and loosening of the implant can pose a serious impact as the fractured segment remaining inside the implant may prevent it from functioning efficiently. The harmony between the implant supported prosthesis and implant could be disrupted, leading to failure of the upper structure. Fistula formation and soft tissue inflammation are frequently associated with loose abutment screws.
This case report involved an evaluation of the screw threads of a loosened abutment compared with those of a fractured abutment removed from the same patient by Scanning Electron Microscopy (SEM). According to the results of the SEM analysis, deformities in the screw threads of the loosened abutment were evaluated, and whether a loosened abutment should be rescrewed was considered.
In this case report an unused abutment screw, broken screw, and loosened abutment screw were analysed by SEM. In the loosened abutment screw, the thread was deformed in the concavities to a greater extent, than in the convexities. The metal structure appeared strained without any cracks. In the fractured abutment screw, the metal structure in the convexities appeared strained with small cracks present at grain boundaries. Crack growth appeared to be related to the high number of crack coalescence events.
A significant difference was observed between screw threads with abutment loosening and screw threads without abutment loosening. Therefore, a loosened abutment should not be rescrewed because it increases the risk of abutment fracture.
Dental implants, Fatigue, Fractography
Case Report
A 59-year-old male edentulous patient was referred to the Department of Prosthodontology due to a fractured locator (Zest Anchor, Inc., Carlsbad, CA, USA) abutment.
Upon clinical examination, the patient had a mandibular overdenture supported by two implants at tooth #33 and #43 regions with locator attachments [Table/Fig-1]. In the upper jaw, there was a precision attachment removable denture supported by implant supported fixed prostheses. The implants were placed at tooth #12, #14, #22, and #24 regions. The screw of the locator abutment at tooth #33 region was fractured and the screw of the locator abutment at tooth #43 region was loosened.
Intraoral view. The patient had a precision attachment removable denture supported by implant-supported fixed prostheses in the upper jaw, and an implant-supported overdenture with locator attachments in the lower jaw.

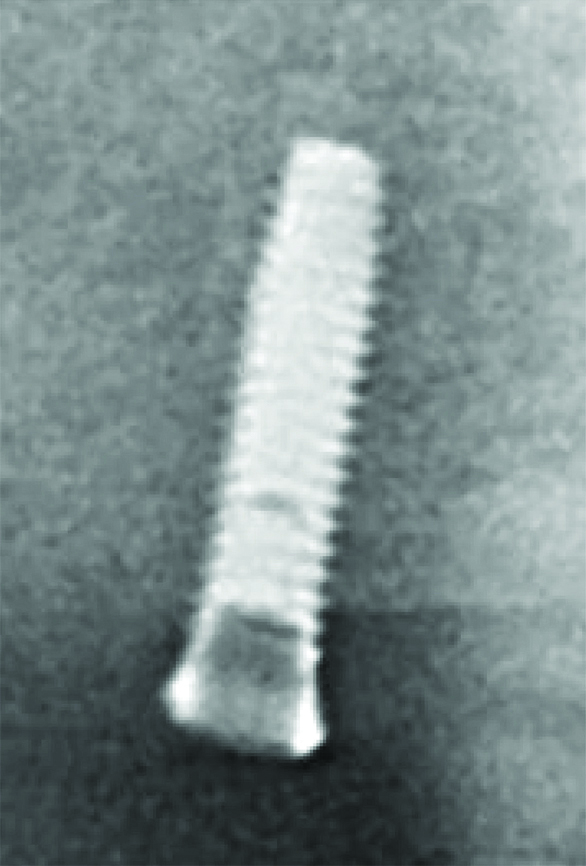
A periapical radiograph was taken, which, together with a clinical examination, showed that the locator abutment at tooth #33 region was fractured on first thread of the screw [Table/Fig-2]. The fractured part of the screw was still inside the implant. The other locator abutment at tooth #43 region was also loosened. The fractured screw was successfully removed using an ultrasonic instrument [Table/Fig-3].
Radiograph of tooth #33 region. A fractured abutment screw is evident.
Images of the fractured and loosened abutments.

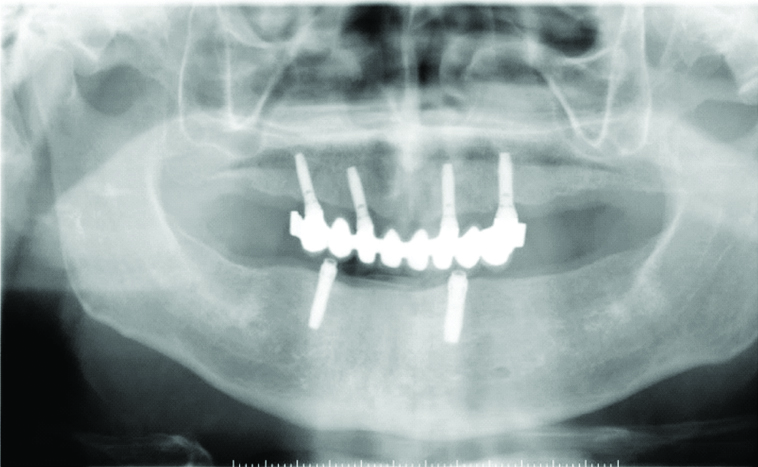
Additionally, the occlusion of the dentures was controlled and bilaterally balanced occlusion was obtained. No problems were noted at 0.5-, 1-, and 5-year follow up examinations [Table/Fig-4].
Panoramic radiograph taken at the 5-year follow up examination.
The threads of the loosened and fractured screws were compared with a new locator abutment of the same implant system by SEM [Table/Fig-5a,6a-7b].
Scanning electron micrographs (magnification: 75× and 100×, respectively) of an unused abutment screw showing some irregularities (arrows).
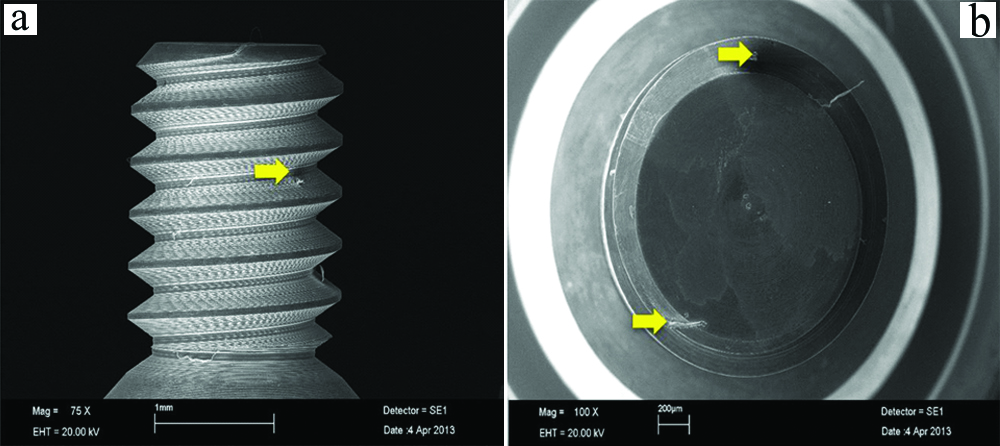
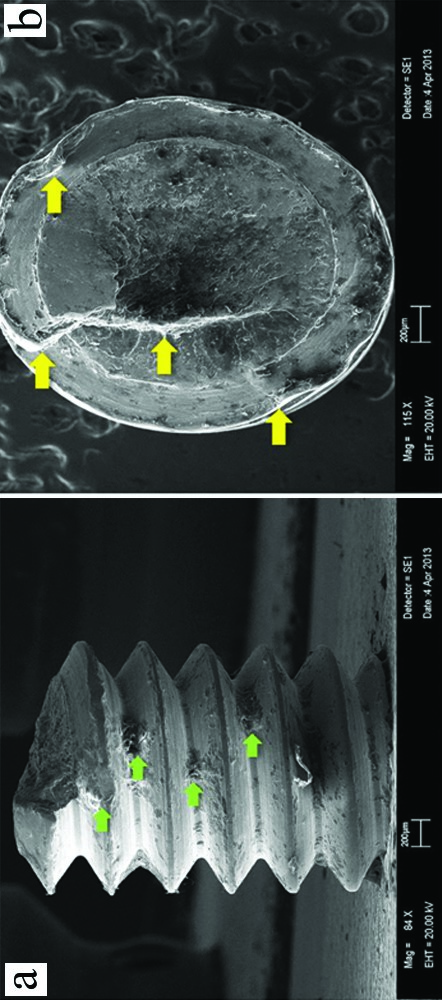
Scanning electron micrographs (magnification: 75× and 100×, respectively) of a loosened abutment screw. Green arrows, deformed thread concavities. Yellow arrows, fractures progressing horizontally from the convexities of the screw to the inner parts.
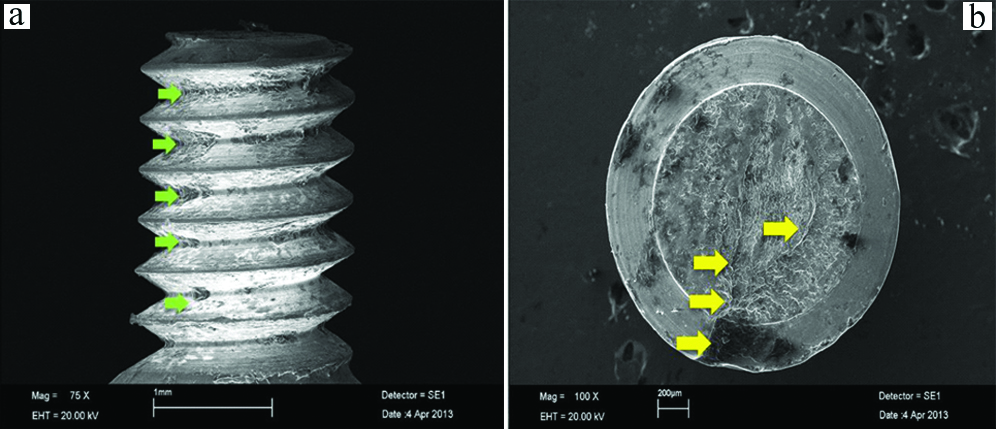
Scanning electron micrographs (magnification: 75× and 100×, respectively) of a fractured abutment screw. Green arrows, deformed thread convexities. Yellow arrows, crack growth related to the high number of crack coalescence events. There was increased fragmentation at the fracture site.
Screw threads of the unused abutment: No macroscopic alterations or deformations were observed. No alterations or deformations in the convexities of the screw thread were present, but some irregularities were noted [Table/Fig-5a,b].
Screw threads of the loosened abutment: Several alterations and deformations were evident in the concavities and convexities of the screw threads of the loosened abutment. The thread appeared deformed in the concavities more than the convexities. The metal structure appeared strained without any cracks. Fractures progressing horizontally from the convexities of the screw to the inner parts were noted [Table/Fig-6a,b].
In the screw threads of the fractured abutment: SEM of the fractured abutment showed a fracture at the junction of the first screw thread and the shoulder of the abutment. Many alterations and deformations were present in the concavities and convexities of the screw threads of the fractured abutment. The thread appeared deformed in the convexities more than the concavities, in contrast to the loosened abutment. The metal structure in the convexities appeared strained with small cracks present at grain boundaries. Crack growth appeared to be related to the high number of crack coalescence events. There was increased fragmentation at the fracture site [Table/Fig-7a,b].
In the patient, the main problem was a non conforming indication. In the upper jaw, the denture was supported by implant supported fixed prosthesis on four implants; in contrast, the mandibular overdenture was supported by two implants with stud attachments. Another possible explanation for the fracture was unrecognised screw loosening due to non axial or excessive prosthetic loading, poor denture support, poor balance, or occlusal rocking. After the new abutments were placed the occlusion of the dentures was controlled and bilaterally balanced occlusion was obtained in order to prevent any loosening in the future.
Discussion
Dental implants are commonly used in contemporary dentistry [1,2], but they can fail biologically or mechanically [3]. Biological factors include unsuccessful osseointegration or the presence of peri-implantitis, while mechanical failures include crown fracture, framework fracture, screw loosening, and screw fracture [3,4]. The most common fracture is on the hexagonal head and not in the main body of the screw [5]. Abutment screw fracture is an uncommon (0.5% to 8%) but challenging technical complication in implant retained restorations and may occur due to bruxism, an unfavourable superstructure, overloading, malfunction, premature occlusal contacts, metal fatigue after screw loosening, and a component misfit [6,7]. A loose screw is more prone to excessive lateral forces [6]. Fracture of the implant abutment screw can be a serious problem as the remaining fragment may prevent the implant from functioning efficiently [8]. The harmony between the upper structure and implant could be disrupted, leading to failure of the upper structure [5,9]. Fistula formation and soft tissue inflammation are frequently associated with loose abutment screws [8,9].
Abutment screw loosening or fracture of the abutment screw are symptoms of a non conforming indication, incompatible mechanic/material compounds, and/or unbalanced occlusal schema and chewing function [6,7].
The previous studies about loosened abutment screws showed that using a loosened abutment screw can increase the risk of fracture of the abutment [10-12]. In this case report numerous alterations and deformations were evident in the concavities and convexities of threads in the loosened and fractured screws. In agreement with the findings of Scarano A et al., macroscopic differences were observed between the unused abutment screw and the loosened and fractured abutment screws [10]. There were some irregularities on the surface of the unused abutment screw, and fractures progressing horizontally from the convexities of the thread to the inner parts were noted in the loosened abutment screw.
In the fractured abutment, the metal structure in the convexities appeared strained, with small cracks at grain boundaries. Crack growth appeared to be related to the high number of crack coalescence events. There was increased fragmentation at the fracture site. In this case report, significant difference was observed between screw threads with abutment loosening and screw threads without abutment loosening. Therefore, a loosened abutment should not be rescrewed because it increases the risk of abutment fracture.
The cause of implant failure can be determined by checking the occlusion, eliminating premature contacts, and equilibrating the chewing force [6,7,9]. A detailed clinical examination should be performed to identify parafunctional activities, including bruxism, which may cause component fractures [9]. The patient can use his/her overdentures without any problem if such factors are eliminated.
Conclusion
In conclusion, it was observed that a loosened abutment screw can lead to fracture, according to the deformations in its structure. For this reason, changing the loosened abutment screws with the new ones will help to reduce the fracture risk. In addition to these, torqueing the abutment screw at the requested torque is important.
It is highly recommended that a detailed clinical examination be performed to identify parafunctional activities, such as bruxism, which may cause component fractures. In these cases, the overdenture patient should be warned about taking off his dentures at nights, or if he uses fixed prosthesis; a night splint should be prepared in order to prevent excessive load.
[1]. Sanchez-Perez A, Moya-Villaescusa MJ, Jornet-Garcia A, Gomez S, Etiology, risk factors and management of implant fracturesMed Oral Patol Oral Cir Bucal 2010 15(3):e504-08.10.4317/medoral.15.e50420038899 [Google Scholar] [CrossRef] [PubMed]
[2]. Tolman DE, Laney WR, Tissue-integrated prosthesis complicationsInt J Oral Maxillofac Implants 1992 7(4):477-84. [Google Scholar]
[3]. Balshi TJ, An analysis and management of fractured implants: a clinical reportThe Int J Oral Maxillofac Implants 1996 11(5):660-66. [Google Scholar]
[4]. Nergiz I, Schmage P, Shahin R, Removal of a fractured implant abutment screw: a clinical reportJ Prosthet Dent 2004 91(6):513-17.10.1016/j.prosdent.2004.03.01015211290 [Google Scholar] [CrossRef] [PubMed]
[5]. Zarb GA, Schmitt A, The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto study. Part III: Problems and complications encounteredJ Prosthet Dent 1990 64(2):185-94.10.1016/0022-3913(90)90177-E [Google Scholar] [CrossRef]
[6]. Canpolat C, Ozkurt-Kayahan Z, Kazazoglu E, Management of a fractured ımplant abutment screw: a clinical reportJ Prosthodont 2014 23(6):402-05.10.1111/jopr.1211124393481 [Google Scholar] [CrossRef] [PubMed]
[7]. Goodacre CJ, Kan JY, Rungcharassaeng K, Clinical complications of osseointegrated implantsJ Prosthet Dent 1999 81(5):537-52.10.1016/S0022-3913(99)70208-8 [Google Scholar] [CrossRef]
[8]. Walia MS, Arora S, Luthra R, Walia PK, Removal of fractured dental implant screw using a new technique: a case reportJ Oral Implantol 2012 38(6):747-50.10.1563/AAID-JOI-D-10-0019522891679 [Google Scholar] [CrossRef] [PubMed]
[9]. Kim SK, Koak JY, Heo SJ, Taylor TD, Ryoo S, Lee SY, Screw loosening with interchangeable abutments in internally connected implants after cyclic loadingThe Int J Oral Maxillofac Implants 2012 27(1):42-47. [Google Scholar]
[10]. Scarano A, Quaranta M, Traini T, Piattelli M, Piattelli A, SEM and fractography analysis of screw thread loosening in dental implantsInt J Immunopathol Pharmacol 2007 20(1):19-22.10.1177/039463200702001s0517897496 [Google Scholar] [CrossRef] [PubMed]
[11]. Scarano A, Murmura G, Sinjiari B, Sollazzo V, Spinelli G, Carinci F, Analysis and structural examination of screw loosening in oral implantsInt J Immunopathol Pharmacol 2011 24(2):77-81.10.1177/03946320110240S21421781450 [Google Scholar] [CrossRef] [PubMed]
[12]. Maalhagh-Fard A, Jacobs LC, Retrieval of a stripped abutment screw: a clinical reportJ Prosthet Dent 2010 104:212-15.10.1016/S0022-3913(10)00133-2 [Google Scholar] [CrossRef]