A major portion of the population that is deaf in the world is illiterate as only 20% of the total 70 million deaf people have gained formal education. This condition is found even in developed nations and is more deteriorated in developing countries [3]. Such a situation may lead to the problem of communication while the patients with impaired hearing are undergoing dental and medical care. This communication gap widens more due to lack of the required knowledge and training by the dental staff while dealing with the patients having impaired hearing. Oral and dental abnormalities have been significant health problems for disabled patients, including those having hearing impairment or blindness. The contentment of life is quite important and the oral cavity plays a vital role in its achievement through functions such as mastication, aesthetics, phonetics, communication and expression [4].
The prevalence of dental caries is high ranging from 46% to 95% in both deciduous and permanent teeth, among deaf population; the reasons being the lack of access to oral health educative and preventive measures among the isolated deaf population. They are unaware about the good oral hygiene measures and possess a negative conception of dental care, leading to poor oral hygiene rates in more than 50% of the deaf population [5]. Moreover, dental professionals being unfamiliar with the proper ways of communicating with such patients, become helpless while recording a proper case history and explaining the treatment plan to them. So, misconception may arise due to inadequate communication between health care providers and the patients with impaired hearing. In addition to the appropriate non verbal methods (such as lip reading, sign language, mimicry, drawings, figures, writing, body language and gestures), the dentists need to utilize the psychological approach, kindness, creativity, endurance and mutual respect while dealing with the deaf patients. Such an approach would definitely bridge the gap between the patients with impaired hearing and the dental professionals.
In order to progress in the oral health service delivery practice and outcome, feedback from the patients regarding dental care and treatment is of utmost importance. Hence, the present study was undertaken to evaluate the dental treatment experiences of patients with hearing impairment in Southern Saudi Arabia.
Materials and Methods
A cross-sectional questionnaire based study was conducted from April 2017 to June 2017 among the individuals with impaired hearing in four different Institutions of Deaf in Southern Saudi Arabia. A total sample of 200 individuals with impaired hearing falling between the age range of 18 to 45 years were randomly selected for participating in the study; out of which 154 subjects fulfilled the inclusion and exclusion criteria and hence making a final sample. All those subjects who had only hearing impairment and who gave the consent of participation in the study were included and all those who had other disabilities or systemic diseases and who were not willing to participate in the study were excluded from it. The total sample of 154 subjects included (n=42, 27.3%) males and (n=112, 72.7%) females. Prior to the study, the ethical approval was obtained from King Khalid University College of Dentistry Scientific Research Committee after submitting the research proposal to the committee. A close-ended self administered questionnaire was given to the study participants in their respective Institutions by one researcher who was helped by the “sign language expert present in the impaired hearing centre for communicating with the study subjects. The questionnaire included two parts; the first part comprised of questions related to demographic data (age, gender and occupation) and other part included questions related to the experience of the participants while undergoing their dental treatment. The second part of the questionnaire included only nine questions so that the respondents would easily respond without losing interest. The Cronbach’s Alpha was used to assess internal reliability of questionnaire and it was found to be satisfactory (α=0.8). The questions enquired about the difficulties faced by the patients with impaired hearing while receiving dental treatment. The awareness of dental surgeons regarding the ways of communication was enquired, the level of satisfaction of dental treatment and type of dental treatment received were all asked through the questionnaire. For ease of understanding, the questionnaire was translated into the local language (Arabic), other than in English. The duly filled questionnaire was collected next day from the respondents. The participants were assured for confidentiality of their responses as well as their identity.
Statistical Analysis
The data thus obtained was statistically analysed using SPSS version 17.0 (Statistical Package for Social Sciences; SPSS Inc., Chicago, IL, USA, 2001). Descriptive analysis and Chi-square tests were used. Statistical significance was set at p-value ≤ 0.05.
Results
In the present study, out of the total of 154 study subjects, (n=112, 72.7%) were females and (n=42, 27.3%) were males. Majority (n=70, 45.5%) of the respondents belonged to age group 18-25 years, 54 (35.1%) of subjects were within age group of 26 to 35 years and (n=30, 19.5%) of the subjects were of the age group 36 to 45 years. A (n=66, 42.9%) of the participants were students, (n=42, 27.3%) were not doing anything, (n=29, 18.8%) were workers and (n=17, 11%) were trainees [Table/Fig-1].
Frequency distribution of respondents.
| Variables | Frequency (n) | Percentage (%) |
|---|
| Age: |
| 18-25 Years | 70 | 45.5% |
| 26-35 Years | 54 | 35.1% |
| 36-45 Years | 30 | 19.5% |
| Mean age : 26.38±0.651 |
| Gender: |
| Male | 42 | 27.3% |
| Female | 112 | 72.7% |
| Occupation: |
| Students | 66 | 42.9% |
| Trainee | 17 | 11% |
| Worker | 29 | 18.8% |
| Not doing anything | 42 | 27.3% |
It was found that the most commonly used method of communication by the respondents with impaired hearing was sign language; followed by the combination of lip reading and sign language. A total of (n=120, 77.9%) of the respondents had visited the general dentists for their or their child’s dental treatment, (n=31, 20.1%) had visited the pedodontists while (n=3, 1.9%) of the respondents had not visited any dentist for treatment. The difference between the responses was found to be statistically significant (p-value ≤0.001). A total of (n=93, 60.4%) of the respondents reported that the dental staff was unaware about their hearing impairment before appointment date. A total of (n=111, 72.1%) of the respondents reported that they were not enquired about their preferred way of communication by the assisting dental staff before the start of treatment, while only (n=43, 27.9%) of the respondents were being enquired about the same. The difference between the responses was statistically significant (p-value ≤0.001). Majority (n=45, 29.2%) of the respondents had undergone tooth extractions, while (n=25, 16.2%) had undergone dental restorations as well as tooth extractions, (n=21, 13.6%) of the respondents had undergone tooth scaling and (n=2, 1.3%) had experienced sealant and fluoride applications. Majority (n=72, 46.8%) of the respondents encountered difficulties (such as being called from the waiting room, communication with dentists/dental nurse and in understanding about the treatment) during their appointment with the dentists. Frequency of response to the familiarity of dentist or dental staff with lip reading, sign language or other special communication methods is given in [Table/Fig-2].
Frequency of response to the familiarity of dentist or dental staff with lip reading, sign language or other special communication methods.
| Response | Frequency, n(%) |
|---|
| Yes | 17 (11.0%) |
| Yes, to some extent | 69 (44.8%) |
| No, not at all | 68 (44.2%) |
Chi-square = 34.455; df=2; p-value<0.001**(statistically significant)
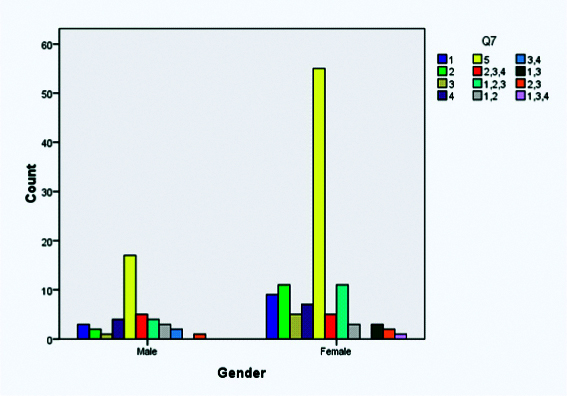
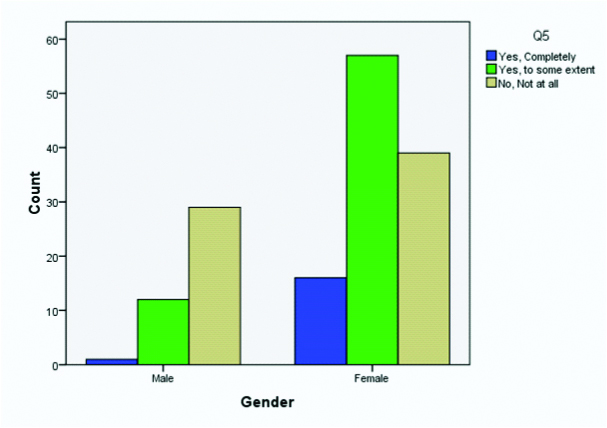
A total of (n=41, 6.6%) of the respondents rated their dental visit experience as “very unpleasant’ and (n=30, 19.5%) of the respondents rated it as being unpleasant [Table/Fig-3]. Frequency of responses on asking the respondents about receiving advice on dental health, good dental practices and prevention of dental diseases in a way that they could completely understand, is given in [Table/Fig-4]. A statistical significant difference was found when the responses of Q5 and Q7 [Appendix-1] were compared based on gender [Table/Fig-5,6] respectively.
Frequency of responses on asking the respondents about their dental visit experience.
| Response | Frequency, n (%) |
|---|
| Pleasant | 34 (22.1%) |
| Satisfactory | 49 (31.8%) |
| Unpleasant | 30 (19.5%) |
| Very unpleasant | 41 (26.6%) |
Frequency of responses on asking the respondents about receiving advice on dental health, good dental practices and prevention of dental diseases in a way that they could completely understand.
| Response | Frequency, n(%) |
|---|
| Yes | 66 (42.9%) |
| No | 88 (57.1%) |
Chi-square= 3.143, df=1;p-value=0.076
Comparison of responses for Q7 on the basis of gender.
p-value<0.001**(statistically significant).
Comparison of responses for Q5 on the basis of gender.
p-value<0.001**(statistically significant)
Discussion
A two-way process that involves a sender and a receiver gives rise to communication. Communication can be described as: “A shared system of signals which requires orderly encoding and apt decoding of signals.” Good communication is fundamental to good clinical practice. For proper understanding between the health care provider and the patient, there needs to be a sound communication system which is obvious between normal individuals but it is not the same with those patients having impaired hearing. The possible causes for loss of hearing can be exposure to very loud noises over a long period of time, viral or bacterial infections, heart ailments or stroke, head injuries, tumors, certain medicines, heredity, or changes in the ear that happen with aging and or a traumatic event. The results, however, are the same in that the individual manifests some degree of difficulty in daily communication [6].
Community that has impaired hearing are at a greater risk of oral diseases because of neglect, unawareness, inaccessibility to routine dental services and poor oral hygiene. Due to the difficulties in communication faced by the patients with impaired hearing while undergoing treatment and they did not receive the required dental care [7]. Hence, the present study was carried out to assess the dental treatment experiences of patients with impaired hearing in Southern Saudi Arabia.
It was found that the most commonly used method of communication among the subjects with impaired hearing, study was the sign language, followed by the combined methods of lip reading and sign language. This finding is suggestive of the fact that the dental professionals should be aware of the methods of communication especially the “sign language” which is possible through sign language courses or by getting in touch with the impaired hearing associations [8]. Sign language has been found to be the most common method of communication among the deaf community in the study carried out previously [9].
In the present study, majority (n=120, 77.9%) of the patients with impaired hearing agreed that they visited the general dentists for their or their children’s dental treatment. This finding was in accordance with the previous studies where high attendance to dentists by patients with impaired hearing was found [10,11]. Many of female respondents agreed that they took their children to pedodontist for treatment when compared to the male respondents; and the difference between the responses based on gender was found to be statistically significant.
In the present study, when the participants of the study were asked whether the dentist or other dental staff were aware of their hearing impairment in advance of their appointment date; the majority (n=93, 60.4%) said that the dentists were unaware about their impairment and rest ((n=61, 39.6%) agreed that they were aware about the same. These results were indicative of the fact that dentists are not much aware about the ways of dealing with the patients with impaired hearing; the dental staff should be prompt enough to know about the details of the patients in advance of their day of appointment so that they could manage less waiting period for such patients [12]. It is being documented in previous study that patients with hearing disability should be given the chance of visiting the dental office prior to the actual day of appointment for dental treatment, so that they get familiar with its environment, smells and staff [13].
In the present study, it was found that only (n=17, 11%) of the respondents felt that the dentists had a complete knowledge of lip reading, sign language or other special communication methods, while (n=69, 44.8%) of the respondents said that dentists were aware about the ways of communication to some extent and (n=68, 44.2%) felt that the dentists were not having any knowledge about the same. Such findings were evidence of the fact that less dentists’ awareness about the required modes of communication would certainly become one of the barriers for receiving dental care by the patients with impaired hearing. The results were similar to the findings of the previous study done by Champion J and Holt R, 2000 [2].
Around (n=45, 29.2%) of the respondents had undergone tooth extractions in the present study, (n=25, 16.2%) of the subjects with impaired hearing underwent tooth restorations as well as tooth extractions while (n=23, 14.9%) had experienced all types of treatments and (n=21, 13.6%) of subjects had undergone tooth cleaning. These findings clearly indicate that the patients who had impaired hearing mostly report to the dentists at a late stage of tooth disease when it is indicated for extraction rather than at earlier stages of restoration of teeth. Hence, the people with impaired hearing lack awareness about oral health and oral hygiene maintenance. Moreover, the least percentage of subjects with impaired hearing underwent preventive measures like fluoride and sealant application which shows their oral health negligence. These findings were in accordance with previous study wherein majority (48.04%) of study subjects received dental extractions [9]. Hence, the oral health education programs should be arranged for disabled community by the concerned authorities which should involve the participation of oral and general health care providers in collaboration with the experts of impaired hearing and the staff of the Institutions of deaf community.
In the present study, around (n=72, 47%) of the respondents faced difficulties in being called from waiting room, communicating with dentist/dental staff and in understanding about the treatment plan; during dental appointments. These findings were similar to those in previous studies [2]. The problems faced by the patients with impaired hearing are due to the unfamiliarity of dental professionals about the appropriate ways of dealing with patients with impaired hearing. It is the moral obligation of the dentists to treat all patients without disparity; under the law, dentists and other health care providers must provide effective communication, including supplying “auxiliary aids and services” as necessary to achieve “effective communication” [12].
In the present study, (n=41, 26.6%) of the respondents rated their dental visit experience as ‘very unpleasant’ and (n=30, 19.5%) of the respondents rated it as being unpleasant while as only (n=34, 22.1%) rated their dental experience as pleasant. It has been mentioned previously that people with hearing problems often receive unethical dental treatment and care due to their individual or systemic factors [14]. This finding requires a serious concern for the disabled patients especially the impaired hearing ones and as such the dental professionals need to understand their role and obligations towards the patients with special needs. It would not only be beneficial for the patients with impaired hearing but it would definitely safeguard the reputation of the dentists in the society as a whole as the doctor-patient bond has been considered as the cornerstone of healthcare delivery system.
Limitation
The study subjects were not classified based on the severity of impairment in hearing. Moreover, the oral health status of the study participants was not being examined.
Conclusion
Majority of the respondents encountered difficulties during their appointment with the dentists, such as being called from the waiting room, communication with dentists/dental nurse and in understanding about the treatment. A huge chunk of the respondents rated their dental visit experience as “very unpleasant’ while others rated it as being unpleasant. The dentists should be aware of the modes of communication while dealing with the patients with impaired hearing so that such patients could avail the health services easily.
It is recommended that dentists should make use of the method of communication which the patients with impaired hearing can understand. Visits should be planned and fixed in such a way that the patients with impaired hearing especially children do not have to wait too long in the waiting halls so as to avoid their anxiety levels. The point about hearing impairment should be mentioned and highlighted in the manual and computer records in the dental clinic so that care would be taken accordingly in recall visits. Recall visits should be fixed at shorter intervals. Dental students should be taught about the methods of communication with the disabled patients including the ones with impaired hearing, during their formative years of bachelor’s course.
Chi-square = 34.455; df=2; p-value<0.001**(statistically significant)
Chi-square= 3.143, df=1;p-value=0.076