Sever’s Disease in a Patient Receiving Growth Hormone with no Causative Relation
Erdal Kurnaz1, Senay Savas-Erdeve2, Zehra Aycan3, Semra Çetinkaya4
1 Attending Physician, Paediatric Endocrinology Clinic, Dr. Sami Ulus Obstetrics and Gynecology and Pediatrics Training and Research Hospital, Ankara, Turkey.
2 Associate Professor, Paediatric Endocrinology Clinic, Dr. Sami Ulus Obstetrics and Gynecology and Pediatrics Training and Research Hospital, Ankara, Turkey.
3 Professor Doctor, Paediatric Endocrinology Clinic, Dr. Sami Ulus Obstetrics and Gynecology and Pediatrics Training and Research Hospital, Ankara, Turkey.
4 Professor Doctor, Paediatric Endocrinology Clinic, Dr. Sami Ulus Obstetrics and Gynecology and Pediatrics Training and Research Hospital, Ankara, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Erdal Kurnaz, Attending Physician, Dr. Sami Ulus Obstetrics and Gynecology and Pediatrics Training and Research Hospital, Paediatric Endocrinology Clinic, Altındag/Ankara-06020, Turkey.
E-mail: erdalkurnaz44@gmail.com
Growth Hormone (GH) shows its main effect on bones and muscle tissues. There are reports of orthopaedic complications including carpal tunnel syndrome, Legg-Calve-Perthe’s disease, scoliosis, and slipped capital femoral epiphysis with GH use in the literature, except for calcaneal apophysitis (Sever’s disease). We hereby present the case of a 13-year-old male who was treated with GH for GH deficiency and developed Sever’s disease in the first year of treatment.
Calcaneal apophysitis, Heel pain, Somatropin treatment
Case Report
A 13-year-old male receiving GH treatment for Isolated Growth Hormone Deficiency (IGHD) presented outside his routine follow up schedule with symptoms of pain in both heels and limping for one month without a history of trauma. The weight and length at birth had been 3000 grams and 50 cm, respectively. The short stature had become more prominent after the age of four years. The physical examination at first presentation to our hospital revealed a calendar age of 11 years 4 months, height 129.9 cm (-2.6 SDS), body weight 23.8 kg (-2.69 SDS), and weight according to height 82% of the 50th centile. Other systemic examination findings were normal. The patient was prepubertal. There was nothing of significance in the laboratory investigations. The bone age was consistent with an age of 8 years. Midparental height was 170.1 cm (-0.49 SDS). Peak GH response to the L-dopa and insulin stimulation tests was 1.57 and 1.04 ng/mL, respectively. The patient’s annual growth rate was 4.4 cm (-0.87 SDS) and started on GH at a dose of 0.03 mg/kg/day with a diagnosis of IGHD. The patient grew 7.4 cm in height in the first year of treatment.
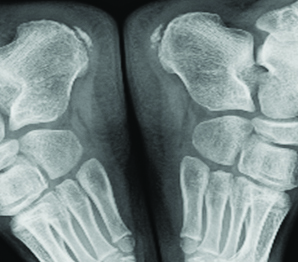
The physical examination at the final presentation to the hospital revealed a calendar age of 13 years 1 month, height 141 cm (-2.06 SDS) body weight 28.4 kg (-2.62 SDS), weight according to height 81%, and testis volumes of 5/5. There was pain in both heels increasing with palpation but with no increase in temperature, hyperaemia or swelling. He could not put his weight on his heels when walking. Laboratory tests revealed haemoglobin 13.4 gm/dL, leukocytes 5420/μL, and thrombocytes 218.000/μL with no atypical cells in the peripheral smear. The lateral foot graph revealed a sclerotic and fragmented apophysis [Table/Fig-1,2]. The patients GH treatment was continued, and he was recommended bed rest and in case of excessive pain the patient was advised nonsteroidal anti-inflammatory drugs. Follow up was undertaken jointly with the Department of Orthopaedics. After three months of follow up the pain in both heels and limping was regressed.
Fragmentation appearance of calcaneal apophysis on lateral foot graph.

Fragmentation of both apophyses.
Discussion
The increased use of GH has led to increased information on its complications. Orthopaedic complications related to the GH (carpal tunnel syndrome, Legg-Calve-Perthe’s disease, scoliosis, and slipped capital femoral epiphysis) are rare and there is no clear pathological association between the use of GH and these complications [1]. Calcaneal apophysitis (Sever’s disease) is an inflammation of the apophysis and is caused by the constant pull of the Achilles tendon. Symptom onset is at around 11-15 years of age in males and 8-13 years in females [2]. The incidence in the general population has been reported as 3.7/1000 [3]. The mechanisms leading to calcaneal apophysitis are not fully known. Some studies have identified obesity and high levels of athletic activity as risk factors [4,5].
These children were reported to have higher body mass index and weight and to be taller than their peers in a recent study [5]. It is possible that the higher impact forces in children with higher body mass/weight causes the calcaneal apophysitis. However, another study suggests that there is no evidence to support that weight and activity levels are risk factors for Sever’s disease [6]. The current patient did not have any of these risk factors. He was quite short before treatment and there was no significant difference in body weight according to height at the end of the first year of treatment. Our case also had no history of participation in any regular sports activity.
Calcaneal apophysitis differs from the orthopaedic complications related to the GH [1]. Calcaneal apophysitis is an inflammation of the apophysis and the most common aetiology of heel pain in growing children. GH has been used for many years, and there is no association with calcaneal apophysitis in the literature. We thus decided to continue GH treatment. The child complained of heel pain during the first year of GH treatment, but this disappeared spontaneously. It is usually managed conservatively with anti-inflammatory medications and restriction of physical activity. The cartilage destruction would cause tissue destruction that will be followed by local inflammatory response [7]. On the basis of current pathophysiological insights, proteoglycan synthesis can be improved by GH which could reduce the inflammation and intra-articular tissue damage [7,8]. We believe that the association can be incidental and that with an anti-inflammatory effect GH can result in an improvement in calcaneal apophysitis.
Calcaneal apophysitis is self-limiting and the treatment is therefore symptomatic. The child is advised to decrease physical activity until the painful symptoms decrease, usually for 3 to 4 weeks [9]. Physical therapy can be useful and focusses on Achilles tendon stretching. Exercises that stretch the heel cord decrease the stress on the apophysis and help relieve symptoms. Nonsteroidal anti-inflammatory drugs such as ibuprofen are also used to control both the pain and inflammation [9]. This case report was previously published as poster presentation in ESPE abstracts [10].
Informed consent: Written informed consent was obtained from the patient.
Conclusion
We did not come across any information on a relationship between GH usage and calcaneal apophysitis development. Recovery of the child was possible without interrupting the GH treatment. However, studies comparing patients treated with GH and healthy controls are required regarding such an association.
[1]. Haidar RK, Nasrallah MP, Der-Boghossian AH, Ghanem IB, Orthopedic complications related to growth hormone therapy in a pediatric populationJ Pediatr Orthop B 2011 20(1):57-61.10.1097/BPB.0b013e32833ed96720811297 [Google Scholar] [CrossRef] [PubMed]
[2]. Micheli LJ, The traction apophysitisesClin Sports Med 1987 6(2):389-404. [Google Scholar]
[3]. Wiegerinck JI, Yntema C, Brouwer HJ, Struijs PA, Incidence of calcaneal apophysitis in the general populationEur J Pediatr 2014 173(5):677-79.10.1007/s00431-013-2219-924297670 [Google Scholar] [CrossRef] [PubMed]
[4]. McKenzie DC, Taunton JE, Clement DB, Smart GW, McNicol KL, Calcaneal epiphysitis in adolescent athletesCan J Appl Sport Sci 1981 6(3):123-25. [Google Scholar]
[5]. James AM, Williams CM, Luscombe M, Hunter R, Haines TP, Factors associated with pain severity in children with calcaneal apophysitis (Sever disease)J Pediatr 2015 167(2):455-59.10.1016/j.jpeds.2015.04.05326001316 [Google Scholar] [CrossRef] [PubMed]
[6]. Scharfbillig RW, Jones S, Scutter S, Sever’s disease: a prospective study of risk factorsJ Am Podiatr Med Assoc 2011 101(2):133-45.10.7547/101013321406697 [Google Scholar] [CrossRef] [PubMed]
[7]. Heemskerk VH, Daemen MA, Buurman WA, Insulin-like growth factor-1 (IGF-1) and growth hormone (GH) in immunity and inflammationCytokine Growth Factor Rev 1999 10(1):5-14.10.1016/S1359-6101(98)00022-7 [Google Scholar] [CrossRef]
[8]. Touati G, Prieur AM, Ruiz JC, Noel M, Czernichow P, Beneficial effects of one-year growth hormone administration to children with juvenile chronic arthritis on chronic steroid therapy. I. Effects on growth velocity and body compositionJ Clin Endocrinol Metab 1998 83(2):403-09.10.1210/jcem.83.2.45699467548 [Google Scholar] [CrossRef] [PubMed]
[9]. Joseph AM, Labib IK, Pediatric heel painClinics in Pediatric Medicine and Surgery 2013 30(4):503-11.10.1016/j.cpm.2013.07.00324075133 [Google Scholar] [CrossRef] [PubMed]
[10]. Kurnaz E, Erdeve SS, Aycan Z, Cetinkaya S, Calcaneal apophysitis (Sever’s disease) development in a case using growth hormoneESPE Abstracts 2016 86:P-P2-682Available from: http://abstracts.eurospe.org/hrp/0086/eposters/hrp0086p2-p682_eposter.pdf [Google Scholar]