Global burden due to Coronary Artery Disease (CAD) is on the rise and there is an immediate demand for strategies to control over these CAD related risk factors [1]. Psychological factors are independent risk factors for coronary heart disease which can be handled specifically with yoga meditation techniques [1,2]. Unregulated lifestyle contributes to the CAD and death, surgery alone cannot improve the health after CABG [3].
In established disease with impending risk of mortality, CABG surgery is necessary to ensure survival. However, it has been shown that, without life style change only CABG cannot prevent mortality. Lifestyle modification that includes exercise, diet and yoga related programs helps in prevention and treatment of CAD along with medication and surgical intervention [4,5]. Perceived QOL is the fundamental parameter which can evaluate the overall wellbeing of CABG [6]. Add on yoga along with conventional rehabilitation was proven to be effective by preventing re-occurrence of arterial occlusion [7]. The YLSP incorporates principles and practices of yoga that include injunctions of righteous and moral living (Yama, Niyamas), Physical postures (Asanas), breathing practices (Pranayama), relaxation techniques and meditation.
Few studies pointed the beneficial effects of yoga based intervention in cardiac rehabilitation in CAD [8]. There were no studies on yoga based lifestyle change before we planned the randomised controlled study on integrated YLSP as an add-on during post CABG rehabilitation [9]. This was a collaborative study between the Yoga University and a Tertiary Cardiac Hospital in Bengaluru, India, funded by the Central Health Ministry of Government of India. In this study, 300 subjects were randomised into add on yoga and control groups. Significantly better increase in left ventricular ejection fraction, decrease in body mass index and lipid levels were seen in the add on yoga group as compared to control group, at one year follow-up. This data which were captured WHOQOL-BREF are yet to be published. The present study, reports the changes in quality of life at one year follow up of the same participants recruited.
Materials and Methods
A two group, single blind, prospective, longitudinal, randomised controlled trial was carried out during July 2005 to January 2007 at Narayana Hrudayalaya Institute of Cardiac Sciences (NHICSc), Bangalore,India, that conducts CABGs. The present study got trial registry as with registry number CTRI/2008/091/000293 and prepared as per consort guidelines [Table/Fig-1]. Out of 1026 patients admitted for CABG, we recruited 300 patients after screening process, using random number generation they were divided into two groups using computer generated random number table (www.randomizer.org) by using sealed envelope method.
Consort guideline statement for the recruitment of participants
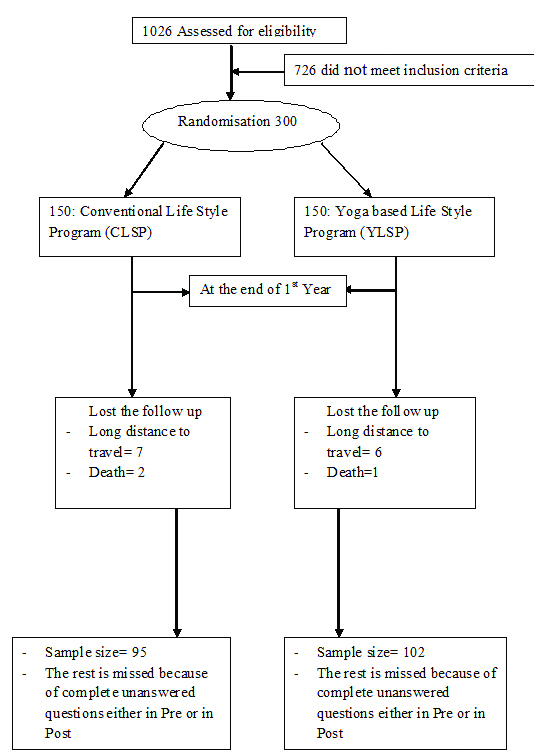
Inclusion criteria: 1) Men posted for elective CABG surgery; 2) Those diagnosed with double and triple vessel disease by angiography; and 3) Those residing within 200 kilometers distance from hospital premises.
Exclusion Criteria: 1) Those with ejection fraction of less than 30%; 2) Those planned for CABG with valve surgeries; 3) Emergency CABG; 4) Those with a history of renal failure, (or) other systemic diseases; 5) Those with physical disabilities that prevented them from practicing yoga module; and 6) Those with earlier experience of yoga were excluded.
The approval for the study protocol was obtained by the Institutional Ethics Committees of both the institutions involved in the present study (Narayana Hrudayalaya Institute of Cardiac Sciences and Swami Vivekananda Yoga Anusandhana Samsthana University, Bengaluru, India). The present study was funded by the ministry of health and family welfare, government of India, New Delhi. A written informed consent was obtained from all participants before the recruitment.
Blinding and Masking
As this was an interventional life style study that involves patient’s understanding and self discipline, double-blind cross over design was not possible. The answer sheets of the QOL were coded and the researcher who did the scoring was blinded to the subject’s group.
Measurement
The WHOQOL-BREF was used as the tool for assessment of their quality of life after one year [10]. WHOQOL-BREF developed by World Health Organisation, has 24 questions under four domains namely D1: Physical (seven items), D2: Mental (six items), D3: Social (three items) and D4: environmental health (eight items). First and second questions related to the “overall quality of life” and “general health” facets were not included for scoring. The range of scores was 4-20 for each domain and scales were in a positive direction i.e., higher scores denote higher quality of life. The internal consistency of WHOQOL-BREF ranged from 0.66-0.87 (Chronbach’s alpha co-efficient). This has good validity and test re-test reliability and is recommended for use in health surveys to assess the efficacy of any intervention at suitable intervals [2]. This has been used for assessment of CAD patients in earlier studies [9]. We used the questionnaire that was available in English and Kannada (local state language).
Intervention
The conventional protocol was common to both the groups, included physiotherapy based breathing exercises during the postoperative hospital stay and advice for long term post-CABG cardiac rehabilitation with study material that included Pharmacotherapy advice by the clinician, a diet sheet prepared by the hospital nutritionist, and ‘physiotherapy’ exercises [Table/Fig-2]. The experimental group was taught the modules specially designed for post-CABG rehabilitation that included Asanas, Pranayama, relaxation techniques and meditation along with diet and counseling on lifestyle modification. The developed module was based on concepts of Ashtanga yoga [Table/Fig-3]. Use of a spirometer for physiotherapy based breathing exercises was taught to both groups on preoperative day by the physiotherapy team which the patients continued to practice during the postoperative period of hospital stay. The YLSP Group had sessions with the yoga therapist on preoperative days to train them in Deep Relaxation Techniques (DRT-10 minutes), Quick Relaxation Technique (QRT-4 minutes), Nadi Shuddhi Pranayama (NSP 12 rounds-6 minutes) and yogic counselling to ally their anxiety. During the first two postoperative days while, in the intensive care unit, the nurses played the prerecorded Compact Disk (CD) using an ear phone that had audio instructions to practice only the DRT and QRT four times a day. After they were transferred to the regular ward, the therapists visited them daily and ensured that they had learnt the practices and were advised to continue the 20 minutes practice (DRT-10 minutes, QRT- 4 minutes and NS- 6 times) four times a day both during hospital stay (5-6 days) and at home after discharge. At the time of follow up visit in the sixth week, they were taught the remaining set of practices in a two hour yoga session and also they were given a prerecorded DVD with video of the practices with instructions and an e-book ‘yoga for hypertension and heart diseases’ and were asked to continue the practices daily at home [Table/Fig-3] [11]. Regular follow up with documentation of their practice was done by weekly phone calls by the therapist who maintained a log book of the dialogue. Review yoga session for one hour under the supervision of the same yoga therapist was given when they came to the hospital for sixth and twelfth month follow up. Follow up was done by phone calls by the therapist if the patients failed to keep up the check up dates. WHOQOL-BREF was documented at the twelfth month follow-up visit.
Intervention of conventional life style program.
| S. No | Duration | Session details |
|---|
| 1 | Pre operative day to 6 weeks | Breathing PracticesPhysiotherapy Exercises for:Wrist, back of hand, elbows, neck, back and legs |
| 2 | 6 weeks to 6 months | Breathing exercises-Inhale through nose and exhale forcibly through mouthBreathing through lung exerciserAdditional Physiotherapy exercisesfor;Wrist, hand, elbows, shoulder rotation, neck, spine, slow side bending, knee cap tightening, knee movementssupine rest |
| 3 | 6-12 months | Additional Physiotherapy exercises in Standing positionSit-ups, Hip rotation, Knee rotation, Forward drill, Backward drill, Sideward drill, Full arm rotation, Free walkingSitting in a chairAnkle bending & Toe bendingLeg spread exercises with support- Side ways, front and backSupine rest |
Intervention of yoga based life style program.
| S. No | Duration | Session details |
|---|
| 1 | Pre operative day to 6 weeks | Deep Relaxation Technique (DRT)Mind Sound Resonance Techniques (MSRT)Nadisodhana Pranayama- Alternate Nostril Yoga Breathing- |
| 2 | 6 weeks to 6 months | SukshmavyayamaManibandhaShaktivikasaka- Wrist movementsKaraprastaShaktivikasaka- Hand jerky extensionKaphoniShaktivikasaka- Elbow movementsGrivaShaktivikasaka I & II- Neck movementsKati Shakthivikasaka I &II-Spine movementsNetraShaktivikasaka- Eye movementsPadasanchala- Lower limb movementsQuick Relaxation Technique (QRT), DRT and MSRT |
| 3 | 6-12 months | Yogic Breathing PracticesPrasarita Hasta Swasah- Hands in & Out BreathingUtkasita Hasta Swasah- Hands Stretch BreathingVyaghraSwasah- Tiger BreathingEkapadauttanasana Swasah- Straight Leg raise breathingStanding Asanas- 20 minutesArdha Kati Chakrasana- Lateral Half Wheel PostureTrikonasana- Triangle postureVrikshasana- Tree PostureGarudasana- Eagle postureSitting AsanasVakrasana- Spinal Twist With Leg straight postureArdhaMatsyendrasana- Half Spinal twist postureVajrasana- Diamond postureProne Lying AsanasBhujangasana- Serpent postureSupine Lying: QRT, DRT, and MSRT |
Statistical Analysis
SPSS version 20.0 was used to analyse the data. Since, the data was not normally distributed on Kolmogorov-Smirnov test, non-parametric tests i.e., Wilcoxon’s signed Rank test was used for comparing the pre and post intervention changes of YLSP. Mann-Whitney U-test was used to compare the between group mean values of both groups. The level of significance was fixed at p-value less than or equal to 0.05.
Results
The trial profile represents the procedure of the present study until the end of first year [Table/Fig-1]. A total of 300 subjects (150 in each group) who satisfied the selection criteria were recruited. After using computer imputation method, the total subjects analysed were: 141 in CLSP and 143 in YLSP Groups at baseline and 95 in CLSP and 102 in YLSP at the end of one year. The reasons for non availability of follow up data were: (a) Hospital distance: seven in control and six in experimental groups lived in different towns and could not come to NHICSc because of time constraints and had their follow-up check up with their family doctor. We could not obtain the QOL forms although these were in touch with the researcher through phone calls; (b) Death: from the available data there were two deaths in control group and one death in yoga group. The information on others (47 subjects in YLSP and 53 subjects in CLSP) could not be traced as the phone numbers, email ids and postal addresses were redundant and they had not reported to the hospital for follow up.
Demographic details are shown in [Table/Fig-4] there was no significant difference between groups in the sample size, age and gender (Chi-square test). All of them were married, belonged to low socio-economic status and were graduate/post graduates. Most of them had hypertension, diabetes and obesity. There was no significant difference between groups with p=0.75 in other risk factors such as family history of CAD, Smoking, Tobacco and the duration of CAD before the admission for CABG. Results of the QOL-BREF are shown in [Table/Fig-5].
Baseline characteristics of studied population.
| Categories | Groups | chi-test(p-value) |
|---|
| CLSP | YLSP |
|---|
| Sample Size(N) | 150 | 150 | - |
| Gender | Male | Male | - |
| Age range (in Years) | 35-65 | 35-65 | - |
| Educational Level | School | 25 | 28 | 2.04 (0.56) |
| Under Graduation | 47 | 41 |
| Graduation | 36 | 45 |
| Post Graduation | 42 | 36 |
| Religion | Hindu | 138 | 142 | 0.85 (0.355) |
| Others | 12 | 8 |
| Economic Status | Lower Class | 150 | 150 | |
| Angiogram Report | Single Vessel Disease | 26 | 16 | 13.99 (0.003) |
| Double Vessel Disease | 27 | 45 |
| Triple Vessel Disease | 95 | 88 |
| Myocardial Infarction | 50 | 25 |
| Associated problems | Diabetes Mellitus | 74 | 83 | 2.12 (0.54) |
| Hyper Tension | 91 | 85 |
| Obesity | 41 | 55 |
| Others | 5 | 6 |
| Risk factors | Alcohol | 18 | 24 | 1.19 (0.75) |
| Family History | 26 | 34 |
| Smoking | 19 | 26 |
| Tobacco | 21 | 19 |
| Duration of Coronary Artery Disease | Less than 1 year | 83 | 92 | 0.55 (0.75) |
| 1 to 5 year | 59 | 58 |
| 5 to 10 year | 8 | 11 |
CLSP: Conventional life style program; YLSP: Yoga based life style program
Level of significance was set as p<0.05
Results: Comparison of QOL domains from baseline to 1st year after CABG.
| Sub-scale | Group | n | Baseline; Mean±SD | 1st year; Mean±SD | WSRT p-value | % Change |
|---|
| D1 | CLSP | 95 | 22.84±5.5 | 22.72±4.2 | 0.684 | -0.52 |
| YLSP | 102 | 22.30±3.9 | 25.32±3.8 | <0.001** | 11.92 |
| MWT | | 0.896 | <0.001** | | |
| D2 | CLSP | 95 | 19.38±2.8 | 18.61±4.0 | 0.103 | -4.13 |
| YLSP | 102 | 19.86±3.7 | 21.23±3.2 | 0.001** | 6.45 |
| MWT | | 0.0158 | <0.001** | | |
| D3 | CLSP | 95 | 10.58±1.8 | 9.43±3.1 | 0.002** | -12.19 |
| YLSP | 102 | 10.27±2.5 | 10.88±2.1 | 0.038* | 5.60 |
| D4 | MWT | | 0.471 | 0.01* | | |
| CLSP | 95 | 25.32±3.6 | 24.48±5.9 | 0.495 | -3.82 |
| YLSP | 102 | 25.68±5.1 | 28.31±4.0 | <0.001** | 9.29 |
| MWT | | 0.379 | <0.001** | | |
| Total score | CLSP | 95 | 78.12±10.6 | 75.24±14.9 | 0.178 | -3.82 |
| YLSP | 102 | 78.12±13.2 | 85.75±11.2 | <0.001** | 8.89 |
| MWT | | 0.480 | <0.001** | | |
Wilcoxon’s Signed-Rank Test;*= p ≤0.05, Statistically Significant; **= p ≤0.001, Highly Significant
D1: Physical Health; D2: Mental Health; D3: Social Interactions; D4: Environmental Health, Gr: Group; MWT: Mann-Whitney Test; WSRT: Wilcoxon Signed Ranks Test, Y: Yoga Based Life Style Program; C: Conventional Life Style Program; N: Sample Size; SD: Standard Deviation
WHOQOL-BREF: Physical health scores showed significant improvement in YLSP group after one year (p<0.001) with non-significant change in CLSP group (p=0.684). There was a significant difference between groups (p<0.001). Mental health scores showed significant improvement in YLSP group after one year (p=0.001) with non-significant change in control (p=0.103) group and a significant difference between groups (p<0.001). Social Relationship scores showed significant improvement in the YLSP group after one year (p=0.038) and higher significance in control group (p=0.002) with significant difference between groups (p=0.01). Environmental health scores showed significant improvement in the YLSP group after one year (p<0.001) and non-significant change in the control (p=0.495) group with a significant difference between groups (p<0.001). The total score showed significant improvement in the YLSP group after one year (p<0.001) and non-significant change in control (p=0.178) group with a significant difference between groups (p<0.001).
Discussion
The present two armed randomised control study on integrated yoga as a lifestyle modification program reports the QOL, one year after CABG. There was significant (p=0.001) better improvement in total score of WHOQOL-BREF and also in the domains of physical, mental and environmental health in YLSP as compared to CLSP group. The male subjects of age group 35-65 years showed significant improvements in all domains of QOL by the end of first year of CABG. The similar age specific study showed a positive correlation with social relations and performance of daily activities [12]. The Asana with physical body movements can improve the physical characteristics of older adults irrespective of their age [13]. Graduation level of education (30%) with less than one year of CAD (61.3%) showed the improvement in QOL with yoga. Maximum (94.7%) of CABG, Hindu culture from South India showed improvement with yoga in the present study. In line to this quote a previous study showed how the cultural differences affect the participation in social activities especially at old age [14]. Male CABG patients of low economic status were reported improvements of QOL in the present study. Maximum percentage angiogram was triple vessel disease with hypertension as the associated problem (58.2%) with prior risk factor of family history (33%) shown improvements of QOL with yoga. Recovery may be because of the survival rate at early postoperative phase just like a recent study which shown the correlation of risk factors (history of smoking, myocardial infarction, diabetes) at one year after CABG [15]. Young age of 46.98 years have presented specific elective CABG with the associated problems like hypertension, hyperlipidemia, smoking and obesity [16].
Physical Domain of WHOQOL-BREF
There was better improvement in the physical domain of WHOQOL-BREF in YLSP than the CLSP group. This domain looks at: Activities of Daily Living (ADL), mobility and need for medical aids. Yoga based module consisted of Asana (physical practices) that involved safe simple stretches followed by deep rest to the stretched part with awareness. Patanjali, the off quoted yoga sage defines Asana (physical postures) as a posture which is maintained with ease and effortlessness for long durations (Sthira Sukham Asanam). The next aphorism (Prayatna Shaithilya and Ananta Samapatti), says that the experience of the joy of restful awareness of the stretched part can achieved through mindful relaxation and expanded awareness while maintaining in the final posture [17]. Thus, the improvement seen in this facet after yoga could be traced to stretches combined with breathing and relaxation during the practice of Asanas. Improved spinal flexibility has been demonstrated in several studies in the patients with back pain, which supports the improvement found in better mobility in this domain of QOL [18,19].
Sleep and rest, Energy and fatigue: It was found in earlier study that yoga can significantly improve the quality of sleep in elderly patients [20,21]. The deep relaxation to all parts of the body after the regular practice of YLSP could have contributed to reduced fatigue, better sleep and rested feeling.
Dependence on medicinal substances and reduction of pain is the effect of local relaxation after the stretches that would have cleared the unrecognised musculoskeletal spasms in different parts of the body [22].
Improved work capacity after yoga postures could be similar to the benefits observed after physiotherapy exercises that are known to improve the cardiac output and micro vascular oxygenation [13]. Asanas, which are slow and progressive physical practices like endurance training can influence the metabolic changes in cardiac functions [23]. It has been shown that short term inspiratory muscle training improves aerobic capacity of muscles which may benefit in long-term [22]. Special breathing practices used in yoga module in The present study may have allowed better peak oxygen uptake contributing to better stamina and work capacity [24].
Psychological Health Domain
The second domain of WHOQOL-BREF has the following facets namely: (a) the bodily image and appearance, Negative feelings, positive feelings, Self-esteem; (b) cognitive functions such as thinking, learning, memory and concentration; and (c) Spirituality/Religion/Personal beliefs.
The multi disciplinary approach of yoga that includes pranayama and meditation leads to mastery over the modifications of mind (Chitta Vritti Nirodhah) as defined by patanjali [17]. The Vrittis or the modifications of the mind, in this context of CAD include persistent emotional responses to stressfully demanding situations of life such as anxiety or frustration that may further result in cognitive impairment [25]. The yoga texts recognise these responses to stress as uncontrolled repetitive thoughts (Perseverative Cognition) that result in psychosomatic problems [26]. Improvement found in these two facets of psychological health namely: (a) better positive feelings, self-esteem, bodily image and appearance; and (b) better cognitive functions, could be traced to reduction of the perseverative negative thoughts that was at the root of all these feelings. Reduction of stress and anxiety that results from a stable calm state of mind has been reported in patients with CAD after yoga intervention [17]. Significant improvement in QOL and lower risk of rehospitalisation after CABG has been observed in Optimistic persons [27]. The relaxation techniques which may have reduced the cortisol levels and hypertension which could contribute to stress reduction as observed by Herlitz J et al., who showed lesser number of disturbing symptoms and better QOL after CABG in those whose hypertension was under good control [28].
Social Relationships Domain
The present domain of WHOQOL-BREF that includes, Personal relationships, social support and sexual activity also improved better in yoga than control group in the present study. Better interpersonal relationship has been reported in pregnant women in the earlier study [29,30]. As described in yoga texts (Kleshas, Patanjali), perseverative adherence to one’s perception of the behavior and attitudes of their near and dear appears to be the root of the problems of interpersonal relationship Kleshas contemporary science and ancient wisdom [23,26]. The lectures followed by discussion with senior yoga therapists have helped the participants to develop the personal autonomy to find contentment without expectation. Better satisfaction in sexual activity could have resulted from better physical stamina and feeling of wellness.
Environmental Health Domain
The present domain did show significant changes (p=0.001) in yoga group as it involves facets such as of financial resources, freedom/physical safety and security, health and social care: accessibility and quality, home environment, opportunities for acquiring new information and skills, participation in and opportunities for recreation/leisure activities, physical environment (pollution/noise/traffic/climate) and transport, which are necessary for achievers in their youth. As most of the patients were almost retired after CABG surgery, they were not faced with these needs. Most of these men had well supported family and led a contented spiritually oriented life after understanding the yogic life style that changed their mindset to a blissfully free state of existence (Samtavam Yoga Uchyate) [31].
Limitation
As the present study was an interventional study no blinding was possible. As expected in any long term follow up in an asymptomatic disease, the response to follow up was poor due to several reasons as highlighted in figure of study profile. Many other variables such as risk factor analysis, documentation of complications and hospitalisation, and the regularity of home practice of yoga module would have helped us to know the long term effects. The present paper reports only one variable which could not be included in earlier publication on other variables due to logistic reasons. We did not carry out intention to treat analysis by extrapolating the data to missing cases.
Conclusion
Conventional rehabilitation with all aspects of lifestyle could significantly improve the social health after one year of CABG procedure at old age of males. But yoga based lifestyle program is an effective adjuvant to conventional lifestyle program for post CABG rehabilitation in improving the overall wellbeing by the end of one year of life in terms of all domains of WHOQOL-BREFF. Hence, add-on yoga as YLSP into the conventional program benefits the postoperative QOL of CABG males at old age.
Financial Support
This was a collaborative study between the Yoga Teaching University and a Tertiary Cardiac Hospital in Bengaluru, India, funded by the AYUSH, Ministry of Department of Health and Family Welfare, New Delhi, India.
CLSP: Conventional life style program; YLSP: Yoga based life style program
Level of significance was set as p<0.05
Wilcoxon’s Signed-Rank Test;*= p ≤0.05, Statistically Significant; **= p ≤0.001, Highly Significant
D1: Physical Health; D2: Mental Health; D3: Social Interactions; D4: Environmental Health, Gr: Group; MWT: Mann-Whitney Test; WSRT: Wilcoxon Signed Ranks Test, Y: Yoga Based Life Style Program; C: Conventional Life Style Program; N: Sample Size; SD: Standard Deviation