Congenital club foot is a complex deformity with four components: cavus, adduction, varus and equinus. Incidence of club foot is approximately 1 in 1000 live births. It is bilateral in about 50% of the cases [1]. The goal of the treatment is achieving correction of four deformities and maintenance of correction so that the patient has a functional, pain free, plantigrade foot. Non operative treatment of club foot, primarily by Ponseti method of serial manipulation and casting is the mainstay of management with percutaneous achilistenotomy with the option of surgical correction, reserved for resistant cases [1,2].
Ponseti method of treatment should begin as early as possible. It has a treatment phase which includes gentle manipulation and weekly casting. Percutaneous Achilles tenotomy is necessary in most cases to correct equinus and to prevent development of a rocker-bottom deformity. The final cast is applied with the foot in 60° of abduction and ankle in 15° dorsiflexion for three weeks. In the maintenance phase, the correction is maintained in brace with foot in of 70° of external rotation and 15° of dorsiflexion. For first three months, it is applied for 23 hours a day and then to wear for sleep time for 2 to 3 years [1-3].
Ponseti recommended the evaluation of treatment strictly by palpation but still radiography is considered by few orthopaedicians. Follow up and monitoring of correction by clinical examination is subjective and dependent on clinical experience. The clinical grading of club foot is limited by inter observer variability and inaccurate assessment of deformities [4]. Various modalities have been used to study the deformities and assess the completeness of correction. Ultrasound has been used to monitor treatment but is limited by intra observer and inter-observer variability. Advantages of ultrasound are absence of radiation, dynamic capability and visualisation of cartilaginous structures and soft tissues. Magnetic resonance imaging is expensive and not suitable for serial evaluation [5-8].
Analytical radiography is a method for studying the four major deformities of club feet [5-7]. Although, the correlation of radiographs to clinical results and its utility in clinical management is controversial, radiographs permit reasonably accurate assessment of the club foot as early as two weeks after birth and the exact degree of correction after treatment can be assessed. Different parameters have been described in studies to define the anatomical deviations, in anteroposterior and lateral radiographs and to record accurately the deformity correction for the evaluation of any corrective procedure [7,8].
This study was undertaken to record the deformities in club foot using radiographs and to evaluate the role of radiographs to assess completeness of correction in treated feet.
Materials and Methods
A non-randomised, interventional study was conducted in patients with idiopathic club foot, in our institute from September 2013 to October 2015. One foot was taken as one unit in the study. Ponseti’s method of casting was used as a method of treatment to treat 27 patients with a total of 44 club feet. Inclusion criteria for study were: age less than one year, both male and female, having unilateral or bilateral idiopathic club foot. All infants with any prior treatment for club foot, with no consent from parents/guardians, atypical club foot with associated neurological or other lower limb disorders were excluded from the study. Institutional Ethical Committee clearance was taken prior to commencement of the study. Written informed consent was obtained by parents/guardians prior to their inclusion in the study.
All infants were assessed clinically on their first visit and data on detailed history, general physical, local examinations was recorded and classified as per the system of Pirani S et al., [9]. Radiographs were taken at the first visit before treatment and were repeated at the end of treatment when the foot was deemed to be normal as per the Pirani score. Anteroposterior and lateral projections were taken. The child was positioned by the investigator with the help of the parent/guardian. The parameters studied included the TCA-AP, the TMT-AP, the TCA LT, the TiC-LT. and the TCI.
Manipulation, casting and Achilles tenotomy was done by same group of orthopaedic surgeons who were well experienced with the Ponseti technique. All radiographic parameters were recorded by radiologist.
All the values were recorded on a standard form and statistical analysis was done using the Statistical Package for Social Sciences (SPSS version 17.0). The Student’s paired t-test was used to compare the variables before and after treatment and a “p value” of less than 0.05 was considered significant.
Results
Twenty-seven patients with a total of 44 club feet were included in the study, including 18 males and 9 females. The deformity was bilateral in 17 patients and unilateral in 10 patients. The mean age at presentation was 3.08 months. An average of seven casts was needed for the deformity correction with a standard deviation of 1.52. Tenotomy was done in 41 feet while it was not done in three feet. The mean values of radiological parameters at presentation and after the deformity correction are as given in [Table/Fig-1]. The Student’s paired t-test showed significant changes for all parameters at the end of treatment (p-value <0.05).
Radiological parameters at presentation and after treatment.
| Angles (n=44) | At presentation Mean (Std. Deviation) | After deformity correction Mean (Std. Deviation) | p-value* |
|---|
| TCA-AP | 21.41 (9.17) | 33.82 (8.81) | 0.0001 |
| TMT-AP | 29.07 (18.04) | 2.14 (10.27) | 0.0001 |
| TCA-LT | 18.05 (8.42) | 34 (4.48) | 0.0001 |
| TiC-LT | 102.95 (15.12) | 64.31 (8.87) | 0.0001 |
| TCI | 39.41 (12.67) | 67.82 (10.17) | 0.0001 |
TCA-AP-Antero-posterior talo-calcaneal angle
TMT-AP-Anterior talo-first talo-first metatarsal angle
TCA-LT-Lateral talo-calcaneal angle
TiC-LT-Lateral tibio-calcaneal angle
*p-value <0.05 is considered statistically significant
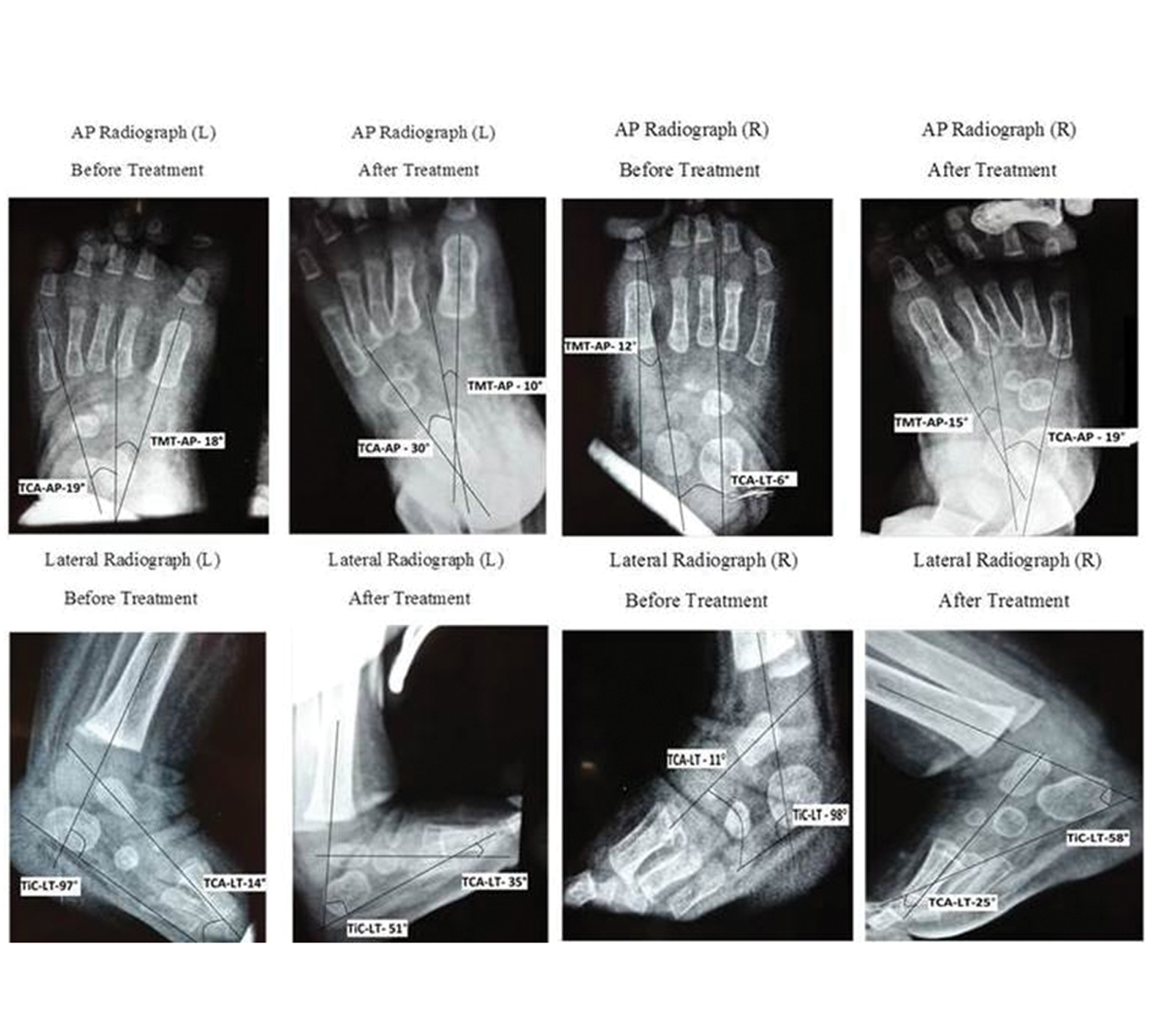
The TCA-AP before treatment had a mean value of 21.41° with a range of 6° to 60°. The TCA-AP after treatment had a mean value of 33.82° with a range of 16° to 64°. The TMT-AP had a mean value of 29.07° with a range of 60° to -16°. The TMT-AP had a mean of 2.143° following treatment with a range of -24° to 32°. Six feet had TMT-AP values greater than 12°, one foot had a value of 60° prior to treatment and 32° following treatment. Five feet had a persisting mild, residual adductus deformity, identified by radiographs The TCA-LT had a mean of 18.05°, prior to treatment with a range of 4° to 46°. The TCA-LT after correction had a mean value of 34° with a range of 25° to 48°. The TCI had a mean of 39.41° before treatment with a range of 17° to 95°. Sixteen out of 17 feet had a pre treatment TCI value higher than 40. The TCI after treatment had a mean of 67.82° with a range of 44° to 102°. The TiC-LT at presentation had a mean value of 102.95° with a range of 51° to 136°. The TiC-LT after treatment had a mean value 64.31° with a range of 46° to 87°. [Table/Fig-2,3 and 4].
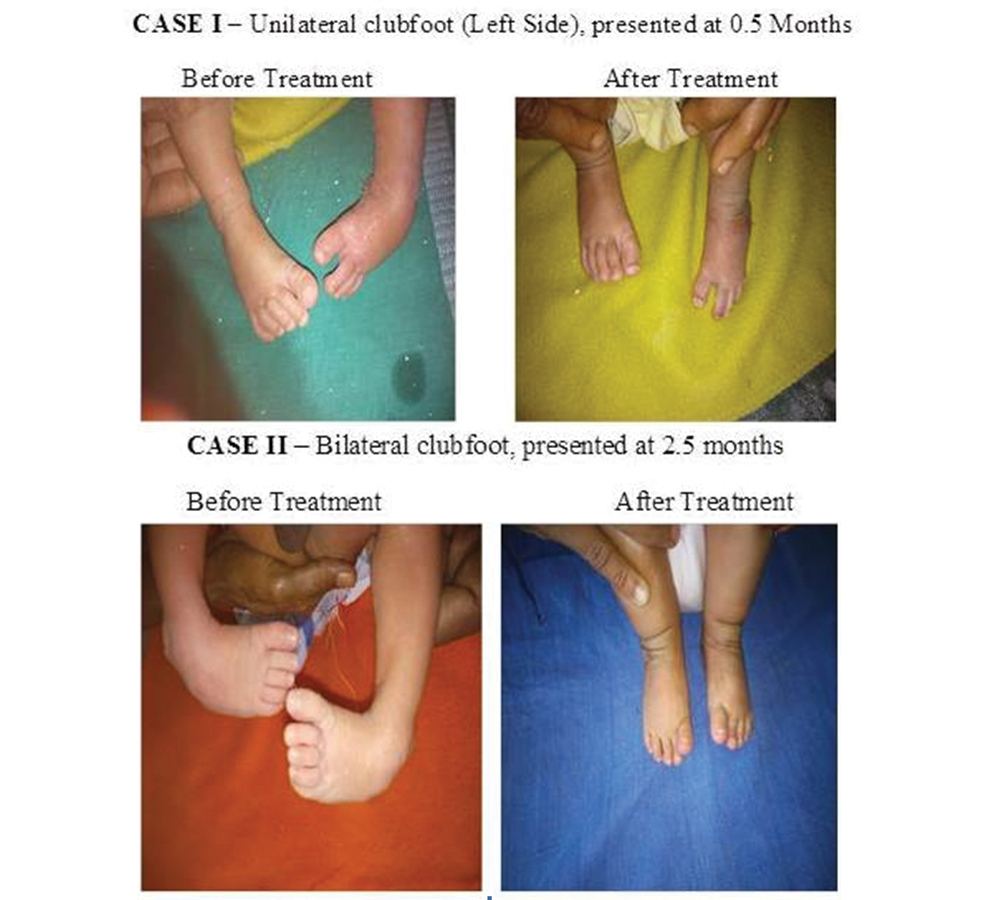
Case I and II:Clinical pictures before and after treatment.

Discussion
Critical evaluation of results of the treatment method is necessary to determine its efficacy. Clinical assessment is a widely used method of assessment of the treatment outcomes in club foot treated by Ponseti method. Radiography is used occasionally for evaluation. When radiographs are taken, positioning of the foot on the film plate accurately is required to obtain good quality radiographs. Hence, all the feet were positioned by the investigator to minimise errors. It has been mentioned in the literature that there was a bias in the drawing of the lines to represent axes of ossific nuclei, which often appeared circular at a very young age [6,7].
There was a large overlap of the TCA-AP values of untreated and treated club foot in this study. Radler C et al., reported that in normal feet in infants, the TCA-AP° ranges from 15° to 55° [6]. This suggested that the varus deformity was corrected after treatment. When literature is reviewed, very few authors noted TCA-AP as reliable guide for assessment of club foot correction. Hence TCA-AP value is a poor parameter to assess hindfoot varus and alone, it cannot be used to assess correction of varus deformity following treatment [1,6-8].
Measurements of TMT-AP in a positive direction are abnormal and indicate forefoot adduction. Only two feet had values which were in the normal range of 0 to -20°. It is thought that these feet had flexible adductus deformity which was fully corrected while positioning the infant for X-ray. If these two values were ignored, the lower limit of TMT-AP was 8°.
Six of the feet had TMT-AP values greater than 12° which was the dividing line between normal and club feet after treatment. One foot had a value of 60° prior to treatment and 32° following treatment. With such a large value, it would have been expected to visualise the adductus deformity clinically; however, clinically no adductus was visualized. It was suspected that this skewed value was due to the erroneous positioning while taking radiographs. If this foot was excluded, the remaining five feet had a persisting mild residual adductus deformity, identified by radiographs, though clinically they appeared normal. There was no worsening of deformity on subsequent follow ups. Radiographs were able to detect deformities which were too subtle to be detected clinically. Review of literature suggests that the TMT-AP is a good parameter to assess correction of adductus, especially when used with the TCA-AP [1,7,8].
The TCA-LT value of less than 35° was consistently seen in club foot and was suggestive of hind foot varus. Radler C et al., in his study had similar results, with a TCA-LT value of 36.51° [6] and Prasad P et al., had an average of 33.80. Two feet had a value equal to or greater than 35°. It is assumed that both these feet had very mild deformities which were corrected while positioning for radiograph [8].
If the two untreated feet with TCA-LT values greater than 35° were excluded, there was an overlap of 11 values. The TCA-LT was not a good parameter to study the correction of the hindfoot varus deformity, though its validity improved when used with another parameter to assess correction.
Normal range of TCI is 0°-55° [6,7]. One foot had a TCI of 95°, the deformity in this case was mild and was correctable on positioning for the radiograph, which explained the cause for a high TCI value. If the TCI was compared, omitting the foot with the TCI of 95°, the upper limit of the range was 55° and was similar to the studies in literature [1,6-8].
The TCI has been considered as one of the very good indicators of hind-foot varus deformity by many authors [1,8]. A TCI of 40° was taken as a dividing line between normal and club feet. Sixteen out of 17 feet with a pre-treatment TCI value higher than 40 had gross equinus. Hence, judging deformity correction, solely based on the TCI values will give wrong results. TCI may be used along with other parameters to assess correction.
The TCA greater than 85° was suggestive of an equinus deformity. All but one had angles greater than 85°. One case had an angle of 51°, it was suspected that the equines deformity was flexible and fully correctable while positioning for radiograph.
The TiC-LT after treatment had a mean value 64.32° with a range of 46° to 87°. In a study by Radler C et al., the mean TIC-LT after treatment was 68.72° which was similar to the values of the present study [6]. The TiC-LT was a good parameter to study the correction of equinus after treatment.
Most commonly used clinical classification systems were studied by Wainwright AM et al., and they found none of them to be satisfactory. There is a need for imaging method to assess and use as a guide to treating foot deformities in children [4].
Bhargava SK et al., studied radiographic and sonographic parameters and concluded that both varied significantly between cases and controls. Sonography however, not only assessed all components of club foot comprehensively but also the sonographic parameters that correlated well with the severity of these components. Sonography was suggested as a superior, radiation free imaging modality for club foot [7].
Prasad P et al., studied radiography with 12 parameters. They opined that neither a single nor multiple parameters represent all deformities in the club foot [8]. They suggested the routine use of radiography during follow up of surgically treated club feet and also suggested that instead of considering any one radiological parameter, many parameters should assess each of the various deformities, would provide a better radiological assessment of the club foot as a whole.
An ethical issue faced during the study was the exposure of infants to radiation. In a study by Radler C et al., the radiographs involved a radiation of 40 kV at 3.2 mAs resulting in a dose 0.37 mGy. In the present study, the values were similar. The benefits of additional information provided by radiographic assessment of club feet out weight the risk of radiation exposure [6].
In our study, we found that the TCA-AP, TCA-LT and TCI were poor parameters to assess hindfoot varus and cannot be used alone to assess the correction of varus deformity following treatment. The TMT-AP was a good parameter to assess adductus and its correction after treatment. The TiC-LT is a good parameter to judge equinus deformity and its correction after treatment. When the above five parameters are used together, it is possible to accurately judge the deformity in an untreated club foot and assess the completeness of correction after treatment.
Limitation
The limitations of our study was small sample of the study, absence of randomisation and control group and there was no correlation with clinical and functional outcomes. Follow up of cases was not done.
Conclusion
Analytical radiology with multiple parameters tends to be more objective and critical in assessing deformities in a club foot. Improper positioning while taking radiographs was the most common problem faced. This could be minimised by following the standardised technique of radiography and taking due care.
TCA-AP-Antero-posterior talo-calcaneal angle
TMT-AP-Anterior talo-first talo-first metatarsal angle
TCA-LT-Lateral talo-calcaneal angle
TiC-LT-Lateral tibio-calcaneal angle
*p-value <0.05 is considered statistically significant