Craniovertebral Junction Compression due to Posterior C1 Arch in Morquio Syndrome: A Diagnostic Dilemma
Basharath Husseni Khan1, Ajit Singh2, Girish Menon3, Tom Devasia4
1 MBBS Student, Department of Medicine, Kasturba Medical College and Hospital, Manipal, Karnataka, India.
2 Research Associate and PhD, Department of Cardiology, Kasturba Medical College and Hospital, Manipal, Karnataka, India.
3 Professor, Department of Neurology, Kasturba Medical College and Hospital, Manipal, Karnataka, India.
4 Professor and Head, Department of Cardiology, Kasturba Medical College and Hospital, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ajit Singh, Research Associate and PhD, Department of Cardiology, Kasturba Medical College, Manipal Academy of Higher Education, Manipal-576104, Karnataka, India
E-mail: ajitjsingh.mcops@gmail.com
Cervical instability, Dysmorphic face, Foramen magnum decompression, Ligamentous laxity, Telecanthus
A nine-year-old female patient reported with chief complaints of abnormal presentation of the neck, weakness in left lower limb with an abnormal gait. Symptoms were insidious, progressive but not associated with pain. She reported difficulty in running and playing for past one year. She was an active kid with good performance in academics. She was born at term gestation, by normal vaginal delivery. She was immunized as per National Immunization Schedule (NIS) and had achieved milestones at the appropriate age.
On physical examination, it was found that patient had generalized ligamentous laxity, dysmorphic facies, telecanthus, short stature (height of the girl-105 cm), pectus carinatum and cubitus valgus. The spine was normal. All the major joints like elbow, wrist, knee, and hip were normal with a normal range of movements except that the 4th metatarsal of both feet were short. She had normal sensation. Her motor examination was also normal, but the reflexes were exaggerated.
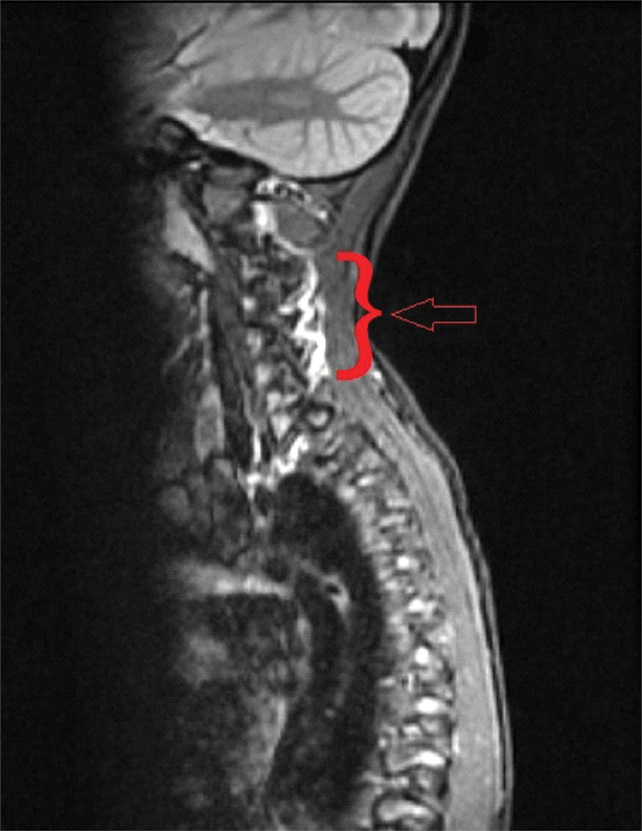
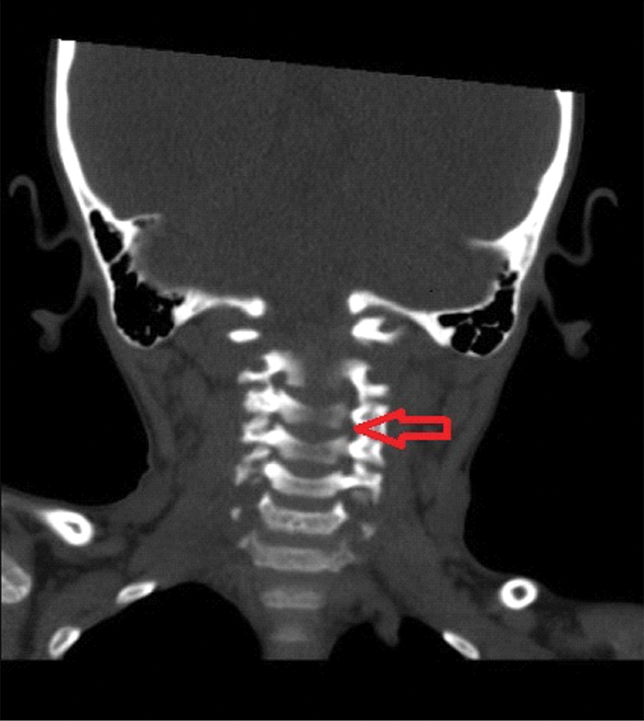
The patient underwent a clinical, radiological and genetic evaluation and her blood sample was sent for enzyme assay. Cardiology evaluation was performed to rule out any birth defects. Echocardiogram showed left ventricular hypertrophy which was not requiring any urgent treatment or intervention. Neurosurgery opinion was taken for cervical instability in view of severe compression at foramen magnum. A Magnetic Resonance Imaging (MRI) for whole spine was done which showed the evidence of platyspondyly with anterior middle 1/3 breaking of vertebra involving cervical, dorsal and lumbar spine. Odontoid hypoplasia with soft tissue anterior to the spinal cord was seen, causing spinal canal stenosis with intramedullary hyperintensities [Table/Fig-1]. A Computed Tomographic (CT) scan confirmed the findings, showing bullet shaped vertebrae and narrowing of the spinal canal at the cervicomedullary junction [Table/Fig-2]. Neck X-ray showed the same evidence as MRI and CT scan [Table/Fig-3]. These features were suggestive of compressive myelopathy. Galactosamine-6-sulfatase enzyme assay was done which showed its deficiency and confirmed the diagnosis of Morquio syndrome Type A.
MRI for whole spine was done which showed the evidence of platyspondyly with anterior middle 1/3 breaking of vertebra involving cervical, dorsal and lumbar spine.
CT scan showing the narrowing of the spinal canal at the cervicomedullary junction.
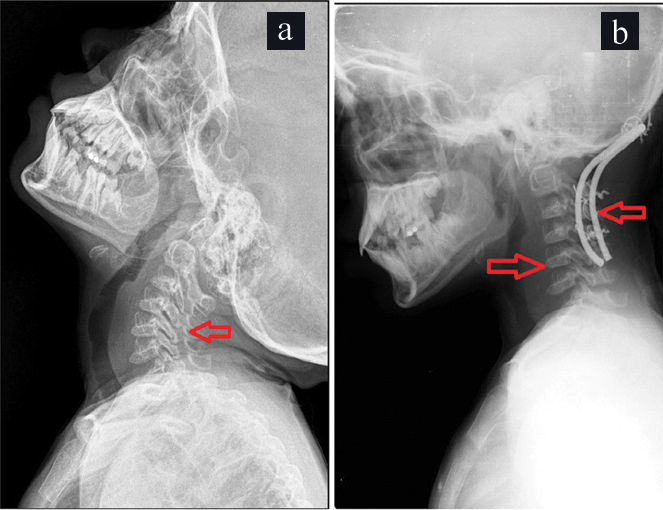
X-ray before a) and after b) the occipitocervical fusion.
a) Shows narrowing of the spinal canal at the cervicomedullary junction and cranio-vertebral compression;
b) Shows bullet shaped vertebrae, foramen magnum decompression and occipito-cervical fusion using sublaminar Sontagg-Dickman wiring and contoured titanium rods.
The patient was advised for surgery involving foramen magnum decompression with removal of the posterior arch of C1. Foramen magnum decompression with removal of the posterior arch of C1 with occipitocervical fusion using sublaminar Sontagg-Dickman wiring and contoured titanium rods was done under general anaesthesia [Table/Fig-3]. Postoperative period was uneventful and she was discharged in the conscious and alert state with stable vitals. Motor system and reflexes were normal. She was advised to take muscle relaxants and NSAIDs for one week with vitamin and calcium supplements. Patient was doing well at 3 months follow up.
Morquio syndrome also referred as Mucopolysaccharidosis IV (MPS IV). MPS IV was first noted by Morquio in 1929, as consisting of skeletal abnormalities, corneal clouding, and cardiac valvular disease [1]. It is categorised into type A and B. In type A; there is a deficiency of enzyme N-acetyl-galactosamine-6-sulfatase caused by a mutation in GLANS gene and in type B, there is a deficiency of enzyme β-galactosidases caused by a mutation in GLB1 gene. It leads to accumulation of Keratin sulfate and Chondroitin-6-sulfate. It especially accumulates in bone that manifests as skeletal abnormalities; also it can accumulate in valves of the heart and cause cardiac valvular disease. In this case leukocytes (blood specimen) were sent for N-acetyl-galactosamine-6-sulfatase enzyme assay which confirmed the Morquio A Type syndrome [2].
Odontoid hypoplasia is one of the most common features of this syndrome. It occurs as the keratin sulfate interferes and delays the ossification of odontoid process. It causes atlantoaxial instability, cervical stenosis and cord compression that presents as chronic compressive myelopathy or as sudden cord [3]. As this syndrome can cause the progressive neurological deficit, acute traumatic quadriparesis or even sudden death due to respiratory arrest as a result of spinal cord compression, it is recommended for a surgical correction by Occipitocervical fusion. The objective of this surgical treatment is to stabilize the spine and halt neurological deterioration [4,5].
Morquio syndrome most commonly manifests as odontoid hypoplasia and cervical stenosis resulting in atlantoaxial instability and cervical myelopathy which may be fatal. Documentation of this syndrome is restricted to isolated case reports and case series, and a greater understanding of the real life limitations of the patients is the need of the hour.
[1]. Tomatsu S, Hendriksz C, Harmatz P, Beck M, Simon J, Wood T, A review of the clinical presentation and diagnosis of Mucopolysaccharidosis IVAMolecular Genetics and Metabolism 2013 108(2):S90-S91.10.1016/j.ymgme.2012.11.246 [Google Scholar] [CrossRef]
[2]. Beighton P, Craig J, Atlanto-axial subluxat ion in the Morquio syndromeBone & Joint Journal 1973 55(3):478-81.10.1302/0301-620X.55B3.478 [Google Scholar] [CrossRef]
[3]. Houten J, Kinon M, Goodrich J, Morquio’s syndrome and craniocervical instabilityPediatric Neurosurgery 2011 47(3):238-40.10.1159/00033431022213779 [Google Scholar] [CrossRef] [PubMed]
[4]. Charrow J, Alden T, Breathnach C, Hendriksz G, Link C, Diagnostic evaluation, monitoring, and perioperative management of spinal cord compression in patients with Morquio syndromeMolecular Genetics and Metabolism 2015 114(1):11-18.10.1016/j.ymgme.2014.10.01025496828 [Google Scholar] [CrossRef] [PubMed]
[5]. Buyukkaya A, Özel M, Onbas Ö, Cervical involvement in Morquio syndromeThe Spine Journal 2015 15(11):e710.1016/j.spinee.2015.06.03526096480 [Google Scholar] [CrossRef] [PubMed]