Anomalous High Transverse Course of Brachiocephalic Trunk and its Clinical Significance: A Rare Case Report
Manisha R Gaikwad1, Krishna S Patil2, Amit P Tirpude3, Naina S Wakode4
1 Additional Professor and Head, Department of Anatomy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
2 Junior Resident, Department of Anatomy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
3 Assistant Professor, Department of Anatomy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
4 Associate Professor, Department of Anatomy, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manisha R Gaikwad, Additional Professor and Head, Department of Anatomy, All India Institute of Medical Sciences, Dumduma, Bhubaneswar-751019, Odisha, India.
E-mail: manishagaikwad6719@yahoo.in
The branching pattern and the course of brachiocephalic trunk in relation to the trachea, thyroid gland has profound surgical importance. Any alteration in the normal course of the brachiocephalic trunk, if accidently ruptured during emergency tracheostomy or thyroid surgeries may lead to haemorrhage. Hence, anomalous course of vessels in the neck and thorax should be kept in mind to prevent iatrogenic injury to abnormal vessels. We present a case with a variable course of brachiocephalic trunk passing left to right transversely crossing trachea in a formalin fixed female cadaver. In this case report, brachiocephalic trunk had its origin from the arch of aorta to the left of trachea corresponding to the left margin of manubrium sterni. Then, it ascended along the left margin of trachea up to the lower border of the left lobe of thyroid gland taking a sharp bend of approximately 90° to hook around and cross the trachea transversely to the right side along the inferior margin of the right lobe of thyroid gland. Knowledge of the variable rather transverse course of the brachiocephalic trunk appears to be important in various surgical approaches such as tracheostomies, thyroidectomies and mediastinoscopies.
Arch of aorta, Innominate artery, Tracheostomy, Thyroid gland
Case Report
During the routine dissection of the neck region in formalin fixed 85-year-old, human female cadaver for undergraduates in Department of Anatomy, the structures in superior mediastinum were traced. Lungs were in situ on both the sides after identifying the structures at hilum. There was no gross abnormality in relation to the medial surfaces of both the lungs. As we dissected and cut open the fibrous pericardium to enter the middle mediastinum, the three branches arising from the arch of aorta were identified. The various measurements were taken using Digital Vernier Calliper (YAMAYO) (accuracy 0.01) and digital camera for capturing images.
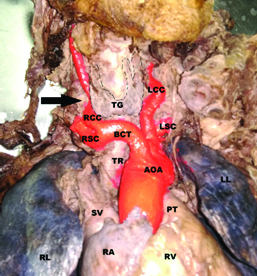
The present case report describes the anomalous course of brachiocephalic trunk and its branches as shown in the [Table/Fig-1]. The brachiocephalic trunk had its origin from arch of aorta to the left of the trachea corresponding to left margin of manubrium sterni. Then it ascended along the left margin of trachea upto the lower border of left lobe of thyroid gland which measured 23.10 mm in length (from its point of origin from arch of aorta upto point of bifurcation into right subclavian and right common carotid arteries) and 10.98 mm in diameter (externally) at midpoint between two sternoclavicular joints. It then took a sharp bend approximately 90° to hook around and cross the trachea to the right side along the inferior margin of right lobe of thyroid gland and measured 21.06 mm of length and 10.46 mm in diameter (externally). At the right margin of trachea below the right lobe of the thyroid, the brachiocephalic trunk divided into the right common carotid and right subclavian artery. The right common carotid artery after division was seen running very close to the right lobe of the thyroid gland, it traversed a deeper plane and curved posterosuperior to right thyroid lobe almost encircling it. There was significant narrowing of right common carotid artery behind the right lateral thyroid lobe and measured 4.68 mm in diameter, whereas the diameter of same artery before and beyond narrowing was found to be more measuring 7.60 mm and 6.94 mm respectively. The right subclavian artery curved around the right common carotid artery until it reached upper border of first rib and coursed between the scalenus anterior and scalenus medius muscles.
Photograph showing anomalous course of brachiocephalic trunk. (AOA-Arch of aorta), (PT-Pulmonary trunk), (BCT- Brachiocephalic trunk), (RCC-Right common carotid artery), (RSC-Right subclavian artery), (LCC-Left common carotid artery), (LSC-Left subclavian artery), (TG-Thyroid Gland demarcated by dotted line), (TR-Trachea), (RA-Right atrium), (RV-Right ventricle), (SV-Superior venacava), (RL-Right lung), (LL-Left lung), Black arrow-showing narrowing of RCC
Discussion
Usually the brachiocephalic trunk arises from the aortic arch in the upper mediastinum and ascends obliquely to divide at the level of the right sternoclavicular joint into the right common carotid and subclavian arteries. Compression syndrome can occur because of anomalous course of the Innominate Artery (IA) in paediatric patients which should not be overlooked [1].
Although, Nomina anatomica uses the term “brachiocephalic trunk” for the right branch of the aortic arch, the overwhelming majority of literature continues to refer to the vessel as the IA, and the respiratory compromise due to tracheal compression by the brachiocephalic trunk is referred as IA compression syndrome [2]. Thorough knowledge of the aortic branches is important in operative procedures of anterior neck structures like tracheostomies, thyroidectomies and mediastinoscopies. Any deviation from the normal course/anatomy can interfere with the surgery and cause vascular catastrophe [3].
The brachiocephalic trunk is the first branch of the arch of aorta measuring about 4-5 cm in length [4]. Any variations in the development of great vessels has significant clinical importance as they supply vital organs and are associated with other major vessels, nerves and important structures in the neck and inlet of thorax. They may produce respiratory distress in paediatric patient and increase the risk of injury during surgery of neck region. Hence, the clinicians and surgeons should be aware of such variations and proceed carefully. In the present report, we describe the anomalous course of the brachiocephalic trunk and its branches.
Normally, the brachiocephalic trunk arises from the arch of aorta posterior to manubrium sterni and then ascends posterolaterally to the right of trachea and then it divides into two main branches, the right subclavian artery and right common carotid artery, whereas in present case the origin of artery is on the left of the trachea and in close proximity of thyroid gland [4]. The 90° turn at the inferior border of the right lobe of thyroid gland and hooking around the trachea which may compress the trachea leading to tracheomalacia. The right common carotid artery had significant narrowing behind the right thyroid lobe which may not compensate enough if there is any obstruction in its counterpart and therefore may end up causing deprivation of the blood supply to brain and important structures of head and neck.
The anomalies of the great vessels are usually due to variation in the fusion and abnormal absorption of the aortic arches during development. In a case reported by Gupta RK and Mehta CD, describes the anomalous course of brachiocephalic artery which is similar to present report, the origin of the brachiocephalic artery was located 1.5 cm horizontally to the left of the median plane, as the first branch of the arch of aorta. It coursed upwards towards the left for ½ an inch and then turned acutely with angle of 90°, to the right and crossed the trachea horizontally in front, overlying the fifth sixth and seventh tracheal rings, along the lower border of the thyroid gland [5].
Karunakaran K et al., reported a rare anomaly during surgery of multinodular goitre, they found right common carotid artery abnormally superficial and crossing the lower pole of the thyroid gland because the brachiocephalic trunk arises from arch of aorta near the left sternoclavicular joint instead of its normal origin near the right sternoclavicular joint. They added that the surgery would have ended in a vascular catastrophe, if they have not been meticulous [6]. Another study done by Iterezote AM et al., on 110 anterior cervical areas of formalin fixed cadavers, they found one case (0.9%) with variation of brachiocephalic trunk measuring 3.4 cm in length and 1.9 cm of diameter, bifurcating anterior to the trachea into right subclavian artery and right common carotid artery. The artery ascended surrounding the right lobe of the thyroid gland maintaining a distance of 0.8 cm [7].
Sharma NA and Garud RS, reported a case of brachiocephalic trunk, which included a high arch of aorta with an abnormally wide brachiocephalic trunk overlapping the left half of the cervical trachea, pretracheal (subisthmic) course of right subclavian and right common carotid artery. And also, unusual origin of the left sided superior thyroid artery from the left common carotid artery and an accessory inferior thyroid artery originating from the aortic arch [8].
A study on anatomical variation in the branching pattern of human aortic arch was done by Budhiraja V et al., on 52 cadavers and found that in 33 (63.5%) cadavers the aortic arch showed classical branching pattern, 19 (36.5%) cadavers showed variations in the branching pattern as 10 (19.2%) cadavers had two branches, 8 (15.3%) cadavers had four branches, and 1 (1.9%) cadaver showed three branches. The point of origin of brachiocephalic trunk in 50 cases were on right side of the midvertebral line, whereas in 2 (3.8%) cases the point of origin was on left of midvertebral line, here the brachiocephalic trunk crossed obliquely upward in front of trachea to reach from left to right side of the trachea [9].
Such anomaly of brachiocephalic trunk is rarely seen and has great clinical importance. If this patient had underwent emergency tracheostomy in her life, brachiocephalic trunk could have been injured, leading to vascular catastrophe. Hence, the knowledge and awareness of such variations would be of great importance during surgery of head and neck region.
Conclusion
As this rare case was noted during routine dissection for teaching undergraduate students, hence the students should be made aware about such variations. Thus, anatomic knowledge of the variations in the course of the aortic arch branches is to be kept in mind while performing emergency procedures in ICU or surgeries of structures in neck such as tracheostomies, thyroidectomies and mediastinoscopies. As minor damage to the great vessels of neck can lead to severe vascular catastrophe.
[1]. Hawkins JA, Bailey WW, Clark SM, Innominate artery compression of the trachea. Treatment by reimplantation of the innominate arteryJ Thorac Cardiovasc Surg 1992 103(4):678-82. [Google Scholar]
[2]. Fawcett SL, Gomez AC, Hughes JA, Set P, Anatomical variation in the position of the brachiocephalic trunk (innominate artery) with respect to the trachea: a computed tomography-based study and literature review of innominate artery compression syndromeClin Anat 2010 23(1):61-69.10.1002/ca.2088419918870 [Google Scholar] [CrossRef] [PubMed]
[3]. Upadhyaya PK, Bertellotti R, Laeeq A, Sugimoto J, Beware of the aberrant innominate arteryAnn Thorac Surg 2008 85(2):653-54.10.1016/j.athoracsur.2007.08.04418222291 [Google Scholar] [CrossRef] [PubMed]
[4]. Standring S, Gray’s AnatomyThe anatomical basis of the clinical practices 2008 40th edChurchill Livingstone Elsvier:985 [Google Scholar]
[5]. Gupta RK, Mehta CD, Anomalous origin and potentially hazardous course of the brachiocephalic arteryJ Anat Soc India 2007 56(2):38-41. [Google Scholar]
[6]. Karunakaran K, Pandian MD, Ganesan R, Gobinath M, Anomalous course of right common carotid artery in a case of papillary carcinoma thyroidIndian J Surg 2013 75(2):145-46.10.1007/s12262-012-0440-924426411 [Google Scholar] [CrossRef] [PubMed]
[7]. Iterezote AM, Medeiros AD, Barbosa Filho RC, Petrella S, Andrade Junior LC, Marques SR, Anatomical variation of the brachiocephalic trunk and common carotid artery in neck dissectionInt J Morphol 2009 27(2):601-03.10.4067/S0717-95022009000200046 [Google Scholar] [CrossRef]
[8]. Sharma NA, Garud RS, Dangerous course of the brachiocephalic trunk and variations of arteries in the cervical region-a cadaveric case reportEur J Anat 2012 16(1):74-78. [Google Scholar]
[9]. Budhiraja V, Rastogi R, Jain V, Bankwar V, Raghuwanshi S, Anatomical variations in the branching pattern of human aortic arch: a cadaveric study from central IndiaInternational Scholarly Research Notices 2013 (2013):82896910.5402/2013/82896925938106 [Google Scholar] [CrossRef] [PubMed]