Otoacariasis or parasitic otitis, is the infestation of the ear with ticks/mites and is a common condition in the livestock and domestic animals. Although, less common, cases of human otoacariasis caused by mites can be occupational in origin and ear being in permanent contact with biotic elements of the biosphere is one of the commonest organs predisposed for various microorganisms to settle in. The local lesions observed in otitis such as skin congestion, increased vascular permeability and raised temperature creates favourable conditions for their development. We here describe a unique case of human otoacariasis caused by mixed aetiology–mites, fungi and bacteria in a 45-year-old female, a grain dealer by profession. To the best of our knowledge this is the first report of human otoacariasis by Cosmoglyphus (Acari: Acaridae) species.
Acinetobacter, Aspergillus, Hypopi, Otoacariasis
Case Report
A 45-year-old female grain dealer by profession presented to Ear, Nose, Throat (ENT) clinic of our hospital with a complaint of feeling a foreign body and severe itching in the right External Auditory Canal (EAC) and associated discharge since four months with accompanying otalgia for around six days. She had previous ear treatment with repeated courses of antibiotics prescribed by private practitioners for three months without any relief.
Standard health checkup was normal. Otoscopic examination of left ear was normal, except for skin lining the right ear canal, which showed thickening and scaling of skin with thick sheets of cell debris and thick purulent discharge. Ear swabs and ear washings from right EAC were collected and were sent for microscopic examination (20% KOH preparation, giemsa stained smear and wet mount), aerobic culture and fungal culture. Sample collection and processing was done as per standard microbiological procedures [1].
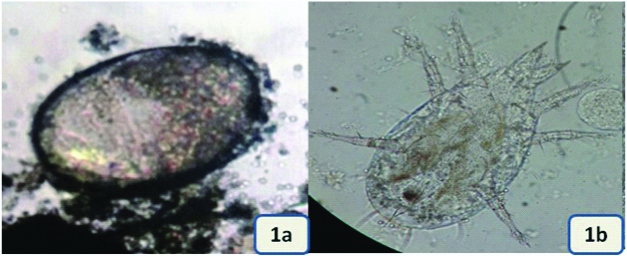
Briefly ear discharge was obtained from the diseased ear of the patient, using four separate pre sterilised swabs. First swab and the ear washings collected were used for preparation of Potassium Hydroxide (KOH) mount, wet mount and smear for giemsa staining. Microscopic examination of the giemsa stained smears showed fungal hyphae with dichotomous branching and few suspended conidia. In wet mount preparations plenty of eggs, larvae and nymphal stages, morphologically suggestive of a mite were seen [Table/Fig-1a,b]. Photographs of the same were clicked and were sent to an entomologist for identification and comments. Second swab was used for aerobic bacterial culture and was plated on 5% sheep Blood Agar (BA), MacConkey’s agar and Chocolate Agar (CA). The plates were incubated at 37°C for 48 hour. Remaining two swabs were used for fungal culture and were inoculated on two slants of sabouraud dextrose agar with chloramphenicol (0.05%) and were then incubated at 28°C and 37°C, separately. The slants were later examined for gross and the microscopic morphology of the fungi. Organisms were identified using standard procedures [2,3].
a) Egg of the mite observed in wet mount preparation (Binocular, light microscope: 400X); b) Mite hypopus observed in wet mount preparation (Binocular, light microscope: 100X).
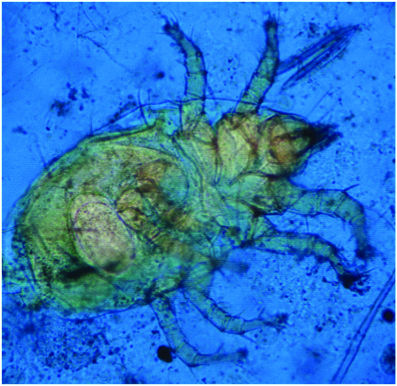
The aerobic culture yielded a moderate growth of Acinetobacter baumannii and the fungal culture showed the growth of Aspergillus niger. A lactophenol cotton blue mount from fungal growth revealed that the mite population was present in association with fungus and probably was feeding on fungus demonstrating its fungivorous character. The photographs were clicked and sent to an entomologist for his comments [Table/Fig-2].
Microscopic photograph of mite hypopus in lactophenol cotton blue mount preparations (Binocular, light microscope: 100X).
Meanwhile, the otologist was informed about the mixed aetiology of mites, fungi and bacteria from the patient samples. Repeat samples taken for confirmation revealed the same picture. Later the reports from entomologist suggested that the mite hypopi belonged to family: Acaridae, genus: Cosmoglyphus with a note that the case of human otoacariasis due to Cosmoglyphus species has not been reported before. Mite hypopus was characteristically shaped with convex dorsal surface, wide and very thin margins forming flat membranes around body and covering basal articles of front two legs and palposoma. Suctorial plate was very small, far from posterior margin of the body, and the posterior legs were completely ventral.
Patient was treated with aural toilet and 1% permethrin ear drops and symptoms resolved after three courses of treatment over five weeks period. Simultaneously treatment with repeated courses of antibiotics {0.3% gentamycin otic solution-four drops TDS×5 days, followed by Cortisporin (neomycin sulphate equivalent to 3.5 mg, polymyxin B sulphate equivalent to 10,000 polymyxin B units and 1% hydrocortisone)-four drops TDS×5 days} and an antifungal (1% clotrimazole otic solution-four drops QID×7 days) was also given. At the end of the therapy symptoms resolved and the otoscopic examination revealed clear EAC. Samples taken one week after treatment did not yield any growth, and patient experienced no further problem.
Discussion
Otoacariasis also called as parasitic otitis, is infestation of the ear with ticks/mites and is a common condition in the livestock and domestic animals. Cases of human otoacariasis by ticks have been reported from various countries but ear infestation caused by mites is less common and under reported. Due to their small size, mites are able to exploit specific habitat and ecological niches, unavailable to arthropods [4]. The ear by remaining in permanent contact with biotic elements of the biosphere is one of the commonest organs predisposed for various microorganisms to settle in. The local lesions observed in otitis such as skin congestion, increased vascular permeability and raised temperature creates favourable conditions for their development [5].
Otitis externa is a common condition causing discomfort and discharge from the ear which can sometimes be occupational in origin. Divers are an occupational group recognised as being at risk of otitis externa, which in most cases is due to bacterial or fungal infection. Mites (Acari: Acaridae) have been found in the EAC of humans and have been reported as a cause of otoacariasis by various authors [4,6-8]. Several species of mites have been reported to infest stored products and to cause otoacariasis as an occupational problem [4,6,7]. Rossiter A, described two cases of otitis externa caused by infestation with Dermanyssus gallinae (the red poultry mite) in poultry workers [6]. Paleri V and Ruckley RW, reported a case of recurrent infestation of mastoid cavities with the storage mite Sancassania berlesei due to occupational exposure [7]. Samung Y et al., reported a similar case of mite infestation due to Suidasia pontifica in an agricultural worker [4].
Mites belonging to family Acaridae infest stored foods (preferably in damp places), prefer high relative humidity (atleast 60%), and usually are fungivores [9]. Kurnatowski P and Filipiak A, during their study on mites described the fungivorous character of mites as they fed on hyphae of various fungi available [5]. Live spores of fungi (such as Penicillium and Aspergillus) can be found in the feces of these mites, which feed on the fungi growing on the grains. The spores can be thus widely distributed by mites and mildewing of grains is accelerated [9].
This patient was owner of a granary store and what authors speculate is that patient may have acquired infection while handling the contaminated and infested grain. Possibly the mites entered the ear from atmospheric dust or by direct transfer from hands. Moreover, patient presented to the clinic during rainy season when the humidity is quite high. Cosmoglyphus is known to occur more abundant in damp and humid stores and feeds on fungi growing on the grain. It is quite possible that mite would have acted as a vector for depositing Aspergillus niger spores into the ear which later got super infected by Acinetobacter baumannii. The fungi and bacteria might have served as source of food for mite. The Acinetobacter baumannii strain recovered was a sensitive strain which is quite unlikely of what is known about this bacterial genus; probably it was a community acquired strain; a coloniser in this case. The mixed aetiology of mite, fungi and bacteria was quite interesting and entirely a new experience for authors.
Cosmoglyphus a cosmopolitan genus of mites belongs to family Acaridae contains 18 species mostly represented only by their heteromorphic deutonymph (hypopus) [10]. The hypopi of all the known species are very close to each other and difficult to distinguish under a light microscope. Being a resource constrained rural setting; electron microscopy was not possible at this point.
On the basis of the reports in the literature and what is known about the feeding behaviour of mites in general we can say that they are facultative commensals surviving on secretions, exudates and microflora in ears of certain mammals [11]. Occasionally they can gain access to the human ears and can cause otoacariasis as a occupational problem. Also, it is more plausible to believe that environmental factors (hot, humid, damp climate), occupation (agricultural workers, veterinarians, poultry workers), and an underlying ear infection (otitis externa, otitis media, mastoiditis, etc.,) can predispose to mite infestation and can cause a resultant problem by their presence.
Mites are common inhabitants of stored products of all kinds including grain and grain based commodities at all stages of processing. They commonly infest grain during harvesting, transporting, processing for consumption and storage. The infestation of stored food products by mites is usually associated with the damage to the products in several ways. Storage mites directly endanger human and animal health due to allergenic contamination of food [12]. Also, mites are vectors of toxigenic fungi and this indirectly contributes to contamination of food and feed with mycotoxins [13]. Moreover, mites cause significant grain weight losses and decreased germinability. With due attention to the human health and also to the nutritional role of the stored food products it is necessary to minimise mite infestations at the primary stage only, this automatically will prevent human infestations. Observance to sanitation, removal of the remains from store, observance of material package and bags, preventing moisture penetration and control of temperature and humidity is all what is required to prevent the mite infestation into stored food products. Several species of mites have been reported to infest stored products and additional species of mites injurious to agricultural workers are expected to be found. It is suggested that good personal hygiene such as hand washing after handling products in the fields or in stores is an important preventive measure.
Conclusion
In conclusion intra aural mite infestation is a painful and distressing experience and needs to be handled quickly and delicately with proper expertise to prevent any complication. This observation highlights the importance of detailed medical history, proper physical examination, a high index of clinical suspicion coupled with extensive microbiological investigations and knowledge of the epidemiology of tick/mite borne diseases, which definitely are important, not only for correct diagnosis but also for institution of appropriate and effective treatment. To the best of our knowledge this is the first report of human otoacariasis by Cosmoglyphus species. Considering the fact that cases of mite infestation are probably under reported due to general lack of awareness about various mite species as an unusual aetiological agent, we are of the opinion that the patients, who are particularly coming from rural areas with persistent otalgia and ear discharge, should be examined carefully to exclude the possibility of mite infestation.
[1]. Forbes BA, Sahm DF, Weissfeld AS, Bailey and Scott’s Diagnostic microbiology 1998 10th edSt. Louis, Misssouri, USAMosby Inc [Google Scholar]
[2]. MacFaddin J, Biochemical tests for identification of medical bacteria 1976 3rd edPhiladelphiaLippincott Williams and Wilkins [Google Scholar]
[3]. Rippon JW, Medical mycology: the pathogenic fungi and the pathogenic actinomycetes 1988 3rd edPhiladelphiaWB Saunders Company:797 [Google Scholar]
[4]. Samung Y, Apiwathnasorn C, Wonglakorn S, Phayakkaphon A, The first reported case of mites, Suidasia pontifica, in the external ear canal of a Thai agricultural workerJ Trop Med Parasitol 2006 29:65-67. [Google Scholar]
[5]. Kurnatowski P, Filipiak A, Otomycosis: prevalence, clinical symptoms, therapeutic procedureMycoses 2001 44(11-12):472-79.10.1046/j.1439-0507.2001.d01-61.x11820260 [Google Scholar] [CrossRef] [PubMed]
[6]. Rossiter A, Occupational otitis externa in chicken catchersJ Laryngol Otol 1997 111(4):366-67.10.1017/S00222151001373389176622 [Google Scholar] [CrossRef] [PubMed]
[7]. Paleri V, Ruckley RW, Recurrent infestation of the mastoid cavity with Caloglyphus berlesei: an occupational hazardJ Laryngol Otol 2001 115(8):652-53.10.1258/002221501190851311535149 [Google Scholar] [CrossRef] [PubMed]
[8]. Cho JH, Kim JB, Cho CS, Huh S, Ree HI, An infestation of the mite Sancassania berlesei (Acari: Acaridae) in the external auditory canal of a Korean manJ Parasitol 1999 85(1):133-34.10.2307/328571710207379 [Google Scholar] [CrossRef] [PubMed]
[9]. Seiedy M, Saboori A, Allahyari H, Preliminary observations on mites found in domesticated animal food factories in Karaj, IranPersian Journal of Acarology 2012 1(2):119-25. [Google Scholar]
[10]. Fain A, Friend JA, Two new acarid hypopi (Acari, Astigmata) from the faeces of the numbat Myrmecobius fasciatus waterhouse (Marsupialia, Myrmecobiidae)Rec West Aust Mus 1984 11:101-08. [Google Scholar]
[11]. Al-Arfaj AM, Mullen GR, Rashad R, Abdel-Hameed A, Oconnor BM, Alkhalife IS, A human case of otoacariasis involving a histiostomatid mite (Acari: Histiostomatidae)Am J Trop Med Hyg 2007 76(5):967-71.10.4269/ajtmh.2007.76.96717488924 [Google Scholar] [CrossRef] [PubMed]
[12]. Olsson S, van Hage-Hamsten M, Allergens from house dust and storage mites: similarities and differences, with emphasis on the storage mite Lepidoglyphus destructorClin Exp Allergy 2000 30(7):912-19.10.1046/j.1365-2222.2000.00815.x10848912 [Google Scholar] [CrossRef] [PubMed]
[13]. Hubert J, Stejskal V, Munzbergová Z, Kubátová A, Vánová M, Zd’árková E, Mites and fungi in heavily infested stores in the Czech republicJ Econ Entomol 2004 97(6):2144-53.10.1093/jee/97.6.214415666776 [Google Scholar] [CrossRef] [PubMed]