Lipofibromatous Hamartoma of Median Nerve with Classical Radiological Features
Surya Nandan Prasad1, Madhuri Kumari2, Raghunandan Prasad3, Hira Lal4
1 Senior Resident, Department of Radiodiagnosis, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
2 Senior Resident, Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi, Delhi, India.
3 Assistant Professor, Department of Radiodiagnosis, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
4 Additional Professor, Department of Radiodiagnosis, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hira Lal, Additional Professor, Department of Radiodiagnosis, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Rae Bareli Road-226014, Lucknow, Uttar Pradesh, India.
E-mail: hiralal2007@yahoo.co.in
Musculoskeletal disease, Peripheral nerve disease, Radiology
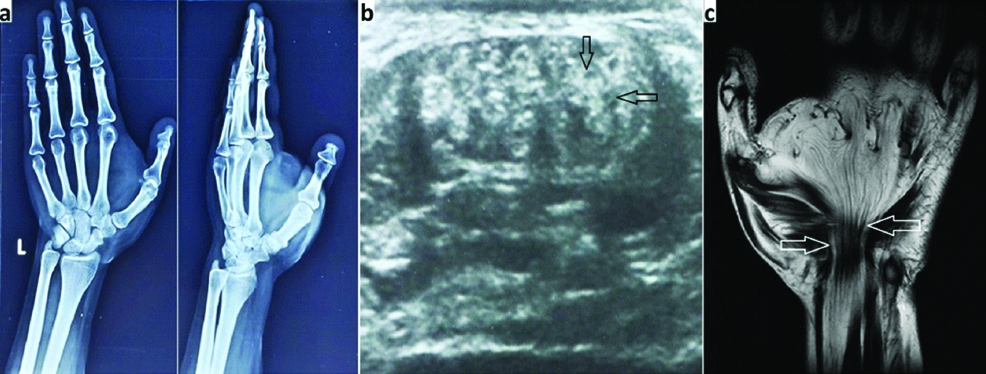
An 18-year-old female presented with an irregular soft swelling over left palm. The lesion was there for last seven years and showing mild gradual increase in size. She also had complain of occasional pain over swelling and tingling sensation in fingers of left hand besides cosmetic disfigurement of the hand. Radiographs showed presence of a soft tissue mass over left palm; however, bones were normal. On Ultrasonography (USG), the lesion was predominantly echogenic, irregular in shape, and traversed by multiple longitudinally oriented hypoechoic cable like structures. On Magnetic Resonance Imaging (MRI), left median nerve was replaced by multiple T1 hypointense cable like structures, traversing through the hypertrophied T1 hyperintense fatty tissue [Table/Fig-1,2]. Based on typical USG and MRI findings, a diagnosis of Lipofibromatous Hamartoma (LFH) of median nerve was made. Conservative management in the form of analgesics for occasional pain and a course of multivitamin capsules containing methylcobalamine were given to the patient. She was advised for a regular clinical and USG follow up.
a) Roentgenograms of left hand in posterioranterior and oblique projections showing soft tissue mass over left palm; b) USG showing echogenic fat content of the mass traversed by hypoechoic cable like fibres of median nerve (black arrows), giving appearance of “coaxial cables”; c) Coronal T1 weighted MRI image shows serpiginous, hypointense axons of median nerve (white arrows) surrounded by T1 hyperintense fat described as “spaghetti like appearance”.
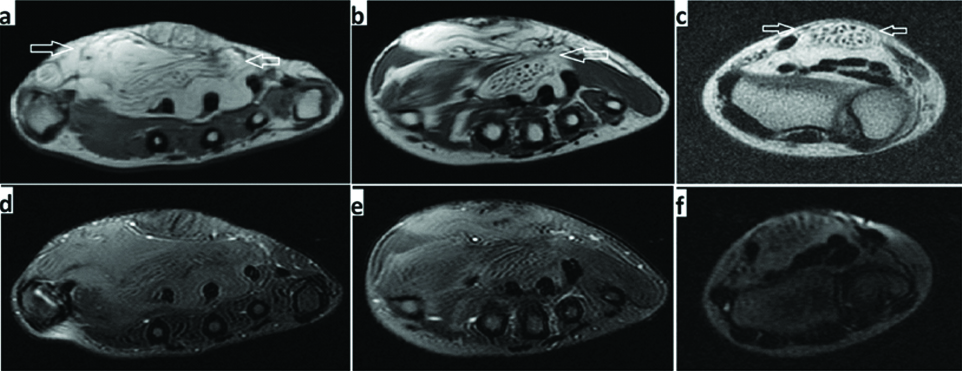
T1W axial MRI images at the level of distal palm; a) Mid palm; b) and distal radioulnar joint; c) Show fibrofatty infiltration of median nerve with nerve fibres surrounded by hyperintense mature fatty tissue, giving the appearance of “coaxial cables” (arrows). On corresponding fat suppressed images; d, e, and f) there is complete signal suppression suggestive of fatty nature of the mass.
Discussion: Lipofibromatous hamartoma of median nerve is a rare disease with less than 200 cases reported in literature till date [1-5]. Normal peripheral nerve is a bundle of axons tightly packed and surrounded by an external covering sheath called perineurium. On cross-sectional imaging, they appear as a cord like structure and devoid of interspersed adipose tissue. The LFH is characterised by proliferation of mature fat cells and fibrous septa within the epineurium and the perineurium of the peripheral nerves. Hypertrophied fat within perineurium separates the thickened axonal bundles causing enlargement of involved nerve and giving classical “coaxial cable” like appearance on USG and MRI in axial planes [4,5]. Median nerve, which lies in volar aspect of flexure tendons in forearm and innervate muscles of hand, is involved in up to 80% of cases [2,3,5]. Less commonly, other peripheral nerves of upper or lower extremity can also be involved [2,4]. Involvement of brachial plexus, radial or ulnar nerves in upper limb and peroneal and plantar nerves in lower limb has been reported in literature [3,5]. Exact aetiology of this condition is not known, but it is thought to have a congenital origin and becomes symptomatic mostly in 3rd-4th decade. Symptoms include pain, tingling sensations, paresthesia and may mimic carpal tunnel syndrome. A 30% of cases have association with macrodactyly [1-3,5]. The differentials, which need to be considered, are ganglion cyst, lipoma, vascular malformation, haemangioma and peripheral nerve sheath tumours [1]. Ganglion cysts are commonly found near wrist joint in relation to tendon sheath of a muscle and may communicate with adjacent synovial joint. They are anechoic or hypoechoic on USG and show fluid intensity on MRI. Lipoma is benign tumour of adipose tissue, which though shows signal suppression on fat saturated MRI sequences; it does not infiltrate the substance of the nerve to separate axonal bundles. Vascular malformations and haemangiomas are hyperintense on fat saturated T2 Weighted Images (T2WI) and enhance avidly on post contrast scans. Also, in cases of high flow vascular malformations, one may notice prominent flow voids within the lesion. Similarly, peripheral nerve sheath tumours are usually of variable signal intensity on T1 and T2WI, do not show fat suppression and demonstrate significant post contrast enhancement. Since, LFH has a classical appearance on MRI, usually it is not a problem to distinguish it from these conditions.
The MRI appearance is considered pathognomonic in LFH and obviate the need of biopsy [1,3,4]. MRI in coronal plane shows serpiginous, hypointense axons of median nerve surrounded by T1 hyperintense fat, described as “spaghetti like appearance” [Table/Fig-1c]. On MRI and USG in axial plane, these nerve fibres appear as multiple “coaxial-cable” like structures [Table/Fig-2] [1-5]. Conservative management and follow up is advised for asymptomatic patients. Surgery is reserved for the cases with significant neurological and functional impairments [1,3].
[1]. Tahiri Y, Xu L, Kanevsky J, Luc M, Lipofibromatous hamartoma of the median nerve: a comprehensive review and systematic approach to evaluation, diagnosis, and treatmentJ Hand Surg 2013 38(10):2055-67.10.1016/j.jhsa.2013.03.02223684521 [Google Scholar] [CrossRef] [PubMed]
[2]. Shekhani HN, Hanna T, Johnson JO, Lipofibromatous hamartoma of the median nerve: a case reportJ Radiol Case Rep 2016 10(11):01-07.10.3941/jrcr.v10i11.278728580055 [Google Scholar] [CrossRef] [PubMed]
[3]. Julien TP, Blazar PH, Lipofibromatous hamartoma: a review articleOrthop J 2009 [available at: www.orthojournalhms.org/volume11/manuscripts/PDF/V11_om_8.pdf; accessed on November 10, 2017] [Google Scholar]
[4]. Toms AP, Anastakis D, Bleakney RR, Marshall TJ, Lipofibromatous hamartoma of the upper extremity: a review of the radiologic findings for 15 patientsAm J Roentgenol 2006 186(3):805-11.10.2214/AJR.04.171716498111 [Google Scholar] [CrossRef] [PubMed]
[5]. Arora R, Arora AJ, Imaging features on sonography and MRI in a case of lipofibromatous hamartoma of the median nerveQuant Imaging Med Surg 2014 4(3):207-09. [Google Scholar]