Introduction
Single tooth anterior dental crossbite is a major aesthetic and functional concern to the parents during the early stages of dental development with evident incidence rate during the early mixed dentition period. Though several treatment modalities exist on the dental management of these patients with developing single tooth anterior crossbite, earlier literature has shown variation among dentists in management of such cases.
Aim
The purpose of this study was to evaluate and compare the total time duration and comfort equation of three different appliances used to manage the condition of single tooth developing anterior crossbite in children at Mogappair, Chennai, Tamil Nadu, India, using a semi structured printed questionnaire.
Materials and Methods
A total number of 30 patients was divided into three groups. 10 patients in each group had underwent treatment with fixed, removable and myofunctional appliances. The inter visit comfort assessment questionnaire in printed format containing five questions was given to all the parents at their first and last visit during their child’s dental treatment, at the waiting area of the department, inside the college campus. Chi-square test was used to analyse the data.
Results
Of the total patients (n=30), the time duration for correcting single tooth developing anterior crossbite by fixed appliance was 11 days, removable appliance was 15 days and myofunctional appliance was 21 days. Comfort equation was found to be better in fixed appliance when compared with removable and myofunctional appliance.
Conclusion
Several treatment modalities are available for the management of single tooth developing anterior crossbite. Based on the results of this study, the author suggest’s that further research is still needed with larger sample size in estimating the time duration and comfort equation used to manage single tooth developing anterior crossbite for providing effective paediatric dental care.
Introduction
The primary care of the paediatric dentist is to guide the child’s developing dentition, in line with the stage of orofacial growth and development [1]. Anterior dental crossbite is a malocclusion resulting from the lingual position of the maxillary anterior teeth in relationship with mandibular anterior teeth [2]. In any type of crossbite correcting appliance, the practitioner has to distinguish first whether crossbite is of dental origin or skeletal origin [3, 4-6]. Crossbite of dental origin does not involve the basal bone, it only involves the localized tipping of a tooth or teeth [7]. In case of simple anterior dental crossbite, the patient displays a normal skeletal pattern with abnormalities presenting in the axial inclination of the affected teeth [5]. According to Profitt, first enough space needs to be opened to bring the displaced tooth or teeth across the occlusion into its proper position, in case of anterior dental crossbite correction [8].
Crossbite is one of the most common dental conditions seen in the mixed dentition period with a significant prevalence rate of 4-5% [9, 10]. An array of factors may result in anterior crossbite which includes palatal eruption path of the maxillary anterior incisors; a repaired cleft lip; trauma to the primary incisor resulting in lingual/ palatal displacement of the permanent tooth germ; supernumerary anterior teeth; an over-retained necrotic or pulpless deciduous tooth or root; odontomas; crowding in the incisor region; arch length inadequacy; upper lip biting habit [6,7,9-12].
The consequences of anterior dental crossbite are abnormal enamel abrasion of the mandibular incisors, dental compensation of mandibular incisors leads to thinning of labial alveolar plate, and/or gingival recession [3, 4-6].
Earlier stage of anterior dental crossbite correction prevents anterior teeth mobility and fracture, periodontal pathosis, and temporomandibular joint disturbance [4,6,12,13].
Various techniques have been used to achieve this goal, such as transforce appliance, tongue blade therapy, composite inclined planes, reverse stainless steel crowns, removable acrylic appliances with lingual springs and fixed appliances [14,15]. However, the purpose of these appliances should not only be aimed to correct anterior dental crossbite, but additionally it should be economical, do not cause any damage to the associated soft tissues, and appliances should also be effortlessly placed, removed and easily tolerated by the patient [16,17]
Any dental appliance or prosthesis should be always aimed to improve the normal function like mastication and phonation. It should not disturb regular oral hygiene maintenance. The variables such as communication, mastication, pain or discomfort, oral hygiene and compliance rate can be collectively referred to as comfort equation. However, these comfort equation inevitably depend on the time duration of the corrective procedure.
Considering all the above mentioned aspects, three most commonly used (fixed, removable, myofunctional) appliances to correct single tooth developing anterior crossbite in early mixed dentition period [6,7,11] were used in this study.
The partial fixed appliance (or partial straight wire appliance) is indicated when more tooth movement is required and to correct the crowded and rotated teeth. Also, it is indicated in patients who exhibit minimal overbite that may require extrusion of the upper or lower anteriors to get adequate overbite at the end of the treatment [18,19].
The hawleys appliance with double cantilever spring is indicated only when there is adequate space for labialization of the teeth in crossbite and in the case of a deep over bite, the spring should be given along with a posterior bite plane to help in jumping the bite [18].
The catlan’s appliance is indicated only where the crossbite is due to palatally displaced maxillary incisor and the disadvantage is that the patient might encounters problem in speech during the therapy, and the appliance may need frequent recementation [18].
Total time duration and comfort equation taken by each appliance and the comfort equation during the course of treatment of the child through their parents were assessed and correlated in the present study.
Materials and Methods
This study was conducted in Department of Paedodontics and Preventive Dentistry, Thai Moogambigai Dental College and Hospital, Dr. MGR Educational and Research Institute University, Chennai from November 2016 to May 2017. Institutional Ethical Committee approval was obtained from Dr. MGR Educational and Research Institute University, Chennai, Tamil Nadu, India (Dr. MGRDU/TMDCH/2016–17/2811020).
After obtaining the informed parental consent, a total number of 33 children, aged 7 to 10 years, who demonstrated with single tooth anterior developing crossbite were included in the study. Three children did not come for the follow up, so they were excluded from the study. Medically compromised, differently abled and un-cooperative children were also excluded from the study.
The study group of 30 children (n=30) with single tooth developing anterior crossbite was randomly divided into three groups with the mean age of eight years [Table/Fig-1,2,3 and 4]. All the selected children with single tooth anterior developing crossbite had mild degree of malocclusion.
Children in each group on the basis of the appliance used.
| Group | Number of Children (n) | Type of Appliance | Appliance Used |
|---|
| I | 10 | Fixed Appliance | Partial straight wire appliance |
| II | 10 | Removable Appliance | Hawley’s appliance with double cantilever spring |
| III | 10 | Myofunctional Appliance | Catlan’s appliance |
Group 1: Fixed appliance (Partial straight wire appliance) case.
a) Pre operative, b) Intra operative, c) Post operative

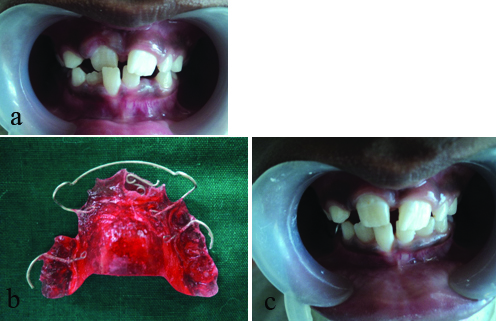
Group 2: Removable appliance (Hawley’s appliance with double cantilever spring) case.
a) Pre operative, b) Hawley’s appliance with double cantilever spring, c) Post operative
Group 3: Myofunctional appliance (Catlan’s appliance) case.
a) Pre operative, b) Intra operative, c) Post operative

After performing the preventive orthodontic procedure to treat the developing malocclusion, total treatment time duration and comfort equation of the same were estimated in this study.
Correction of anterior single tooth developing crossbite was assessed through scheduled periodic recall for activation of the appliance. Total time duration from initiation of treatment till the phase when the crossbite was relieved and occlusion was established, was recorded to obtain total time duration for each group.
Comfort equation of the children were assessed through a semi structured questionnaire by their parents by filling up during their intervisit, after the delivery of the appliances, which consisted of self explanatory objective questions based on comfort equation. The questionnaire composed of all closed ended questions. It focused on the total time duration and comfort equation of most commonly used three different appliances for the management of single tooth developing anterior crossbite in children.
A panel of three paediatric dentist and orthodontist were consulted to establish and content validity of the questionnaire. Based on the expert’s advice from the field of Paediatric Dentistry and Orthodontics, the questionnaire was modified. Consensus method was followed to assess the reliability of the questionnaire [20]. These were filled by the parents on the course of the treatment of their child’s anterior single tooth crossbite correction at first and at the last visit in front of the post graduate student in their own hand writing.
Participation of parent was completely voluntary and had the autonomy to depart from filling the questionnaire at any stage. The post graduate student did not provide any clarification or clear any doubts of the participants.
The completed printed questionnaires were collected safely and preserved for statistical analysis. Incentives or compensation was not offered to the participants for completing the questionnaire. From the questionnaire, comfort equation score was formulated and estimated for every participant in each group.
The guide chart will aid in assessing the comfort equation questionnaire and also guide the parent to fill the semi structured printed questionnaire [Table/Fig-5].
Guide chart of comfort equation questionnaire.
| S. No | Comfort Equation | Scoring Criteria |
|---|
| 1 | Communication | Yes | If the child had difficulty in communication during the course of the treatment |
| | No | If the child had no difficulty in communication during the course of the treatment |
| 2 | Mastication | Yes | If the child eat food normally during the course of the treatment |
| | No | If the child cannot eat food normally during the course of the treatment |
| 3 | Oral hygiene level | Yes | If the child had foul smell during the course of the treatment |
| | No | If the child does not had foul smell during the course of the treatment |
| 4 | Pain/ Discomfort level | Yes | If the child had pain and discomfort |
| | No | If the child does not had pain and discomfort |
| 5 | Rate the appliance | Poor | If the child is more uncomfortable, cannot eat food items properly, painful, foul smell and food gets lodged. |
| | Average | If the child is slightly uncomfortable, cannot eat food items regularly, painful at times, sometimes foul smell and food gets lodged. |
| | Good | If the child is comfortable, can take food regularly, not painfull, without any foul smell and food lodgment |
Average time duration taken to complete the correction of anterior single tooth developing crossbite was evaluated. Each parameter in the comfort equation questionnaire were statistically evaluated and compared in each group using chi-square test.
Results
The average time taken from the initiation of the treatment till the correction when the crossbite is relieved and occlusion is established for group I, group II, group III are 11,15 and 21 days respectively. [Table/Fig-6] shows base line data of total number of girls, boys, age groups and teeth involved.
Baseline data of total number of girls, boys, age groups and teeth involved.
| Age group | Sex | Total | Tooth Involved |
|---|
| Years | Male | Female | 11 | 21 |
|---|
| 7-8 | 6 | 4 | 10 | 04 | 06 |
| 8-9 | 2 | 7 | 09 | 06 | 03 |
| 9-10 | 5 | 6 | 11 | 07 | 04 |
All the parameters in the comfort equation questionnaire were evaluated individually between the groups. Communication problems, mastication difficulty, oral hygiene maintenance, pain and discomfort had been tabulated in [Table/Fig-7] during the first and last visit of child’s single tooth developing anterior crossbite correction.
Chi-square test to compare proportions between the groups at their first and second visit.
| Questions | Groups | p-value |
|---|
| Group I | Group II | Group III | Total |
|---|
| N | % | N | % | N | % | N | % |
|---|
| Communication problem-1st visit | Yes | 2 | 20.0 | 1 | 10.0 | 2 | 20.0 | 5 | 16.7 | 0.999 |
| No | 8 | 80.0 | 9 | 90.0 | 8 | 80.0 | 25 | 83.3 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Mastication-1st visit | Yes | 7 | 70.0 | 1 | 10.0 | 8 | 80.0 | 16 | 53.3 | 0.004 |
| No | 3 | 30.0 | 9 | 90.0 | 2 | 20.0 | 14 | 46.7 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Oral hygiene level-1st visit | Yes | 6 | 60.0 | 9 | 90.0 | 3 | 30.0 | 18 | 60.0 | 0.029 |
| No | 4 | 40.0 | 1 | 10.0 | 7 | 70.0 | 12 | 40.0 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Pain/Discomfort level-1st visit | Yes | 6 | 60.0 | 4 | 40.0 | 9 | 90.0 | 19 | 63.3 | 0.089 |
| No | 4 | 40.0 | 6 | 60.0 | 1 | 10.0 | 11 | 36.7 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Rate the appliance-1st visit | Good | 10 | 100.0 | 0 | .0 | 0 | .0 | 10 | 33.3 | <0.001 |
| Average | 0 | .0 | 10 | 100.0 | 0 | .0 | 10 | 33.3 |
| Poor | 0 | .0 | 0 | .0 | 10 | 100.0 | 10 | 33.3 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Communication problem-2nd visit | Yes | 0 | 0 | 1 | 10.0 | 2 | 20.0 | 3 | 10.0 | 0.754 |
| No | 10 | 100.0 | 9 | 90.0 | 8 | 80.0 | 27 | 90.0 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Mastication-2nd visit | Yes | 2 | 20.0 | 1 | 10.0 | 10 | 100.0 | 13 | 43.3 | <0.001 |
| No | 8 | 80.0 | 9 | 90.0 | 0 | 0.0 | 17 | 56.7 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Oral hygiene level-2nd visit | Yes | 10 | 100.0 | 9 | 90.0 | 7 | 70.0 | 26 | 86.7 | 0.286 |
| No | 0 | 0.0 | 1 | 10.0 | 3 | 30.0 | 4 | 13.3 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Pain/Discomfort level-2nd visit | Yes | 7 | 70.0 | 4 | 40.0 | 6 | 60.0 | 17 | 56.7 | 0.531 |
| No | 3 | 30.0 | 6 | 60.0 | 4 | 40.0 | 13 | 43.3 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
| Rate the appliance-2nd visit | Good | 10 | 100.0 | 0 | 0.0 | 0 | 0.0 | 10 | 33.3 | <0.001 |
| Average | 0 | 0.0 | 10 | 100.0 | 0 | 0.0 | 10 | 33.3 |
| Poor | 0 | 0.0 | 0 | 0.0 | 10 | 100.0 | 10 | 33.3 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 | 30 | 100.0 |
On evaluation of all overall rating the appliance in the questionnaire, comfort equation was better in group I, when compared with other two groups. Group I was found to be more effective and less time consuming towards single tooth developing anterior crossbite correction.
Discussion
The most important objective in paediatric dentistry is to maintain or improve arch integrity to allow permanent teeth to erupt and prevent the development of malocclusion. Condition of anterior dental crossbite is considered as primarily aesthetic and functional concern to children, parents and that seldom corrects itself [16].
However, early orthodontic intervention may need for developing Class III patients with moderate to severe anterior crossbite and deep bite [21].
Early interception of developing anterior single tooth crossbite results in better correction that can be established. Treatment may become more complicated, if the treatment is postponed to a later developmental stage [22,23].
Eight to eleven years is the ideal age to treat developing anterior tooth crossbite, as this is the period when the root is being formed and the tooth is in the active stage of eruption [24].
Interceptive orthodontics should be more of a passive guidance procedure rather than an active procedure. Anterior dental crossbite can be habitual or due to ectopic eruption, single tooth or segmental, which may lead to skeletal discrepancy resulting from functional forward shift of the mandible on closure [10]. During the early mixed dentition stage, the incidence rate of anterior dental crossbite is 4-5% [9,10].
It is a critical role for a clinician to decide whether it is skeletal or dental form, profilometric analysis and intra oral findings are the need for the hour in management of anterior single tooth developing crossbite (Fixed, Removable, Myofunctional appliance therapy) [25].
Tongue blade therapy, reveres stainless steel crown, lower anterior inclined plane (Catlan’s Appliance), removable appliance with finger spring, bonded resin composite slopes and Bruckl appliance are the alternative treatment modalities for correcting anterior dental crossbite [6,7,11].
Lee BD suggested three basic factors for the case selection and appliance design for the success of the treatment includes as adequate space in the arch to reposition the tooth, sufficient overbite to hold the tooth in position following correction, and a class I molar relation [4].
However, in the present study considering the prime importance of time and tolerance, time duration and comfort equation of three different appliances (Fixed, Removable and Myofunctional) employed to manage the condition of single tooth developing anterior crossbite in children were assessed.
The average time taken for correction of developing anterior single tooth crossbite in this present study were 11,15 and 21 days in group I,II,III respectively. There is a significant contrast to the study conducted by Kennedy DB and Osepchook M, with removable appliances which demonstrates with a standard time range from 6 to 12 weeks [26].
Analysing the comfort equation in our study, catlan’s appliance reported with communication problem. This is in line with the study evaluated by Graber TM and Croll TP, collectively reported with severe difficulty in speech, mastication and risk of anterior open bite if the appliance is cemented for more than six weeks [3,27,28].
This significant result can be effectively corrected by proper case selection and reinforced parent and patient counseling regarding the compliance and treatment to be rendered to the child.
In relevance to the methods used for correcting anterior single tooth developing crossbite, it should not cause damage to the tooth, nor the marginal periodontal tissue, since it is the occlusal and masticatory forces which move the tooth towards the labial side, sliding it along the created plane in a brief time [7].
The critical determinant obtained from this study was to choose appropriate treatment protocol and to minimize the difficulty faced by the child on the course of the treatment. It is always better to render effective treatment for a short period of time rather than prolonging the course of the treatment with limited efficiency.
Conclusion
Among the three different appliances used for the management of single tooth developing anterior crossbite, the total time duration and comfort equation was better in fixed appliance therapy. Further research is still needed with larger sample size in estimating the time duration and comfort equation used to manage anterior single tooth developing crossbite for providing more efficient and reliable data in establishing the benchmark in this context.
[1]. Al-Sehaibany F, White G, A three dimensional clinical approach for anterior crossbite treatment in early mixed dentition using an Ultrablock appliance: case reportJ Clin Pediatr Dent 1998 23(1):1-7. [Google Scholar]
[2]. Jirgensone I, Liepa A, Abeltins A, Anterior crossbite correction in primary and mixed dentition with removable inclined plane (Bruckl appliance)Stomatologija 2008 10(4):140-44. [Google Scholar]
[3]. Graber TM, Orthodontics: Principles and Practice 1988 3rd editionPhiladelphia, Pa, USAW. B. Saunders [Google Scholar]
[4]. Lee BD, Correction of crossbiteDent Clin North Am 1978 22(4):647-68. [Google Scholar]
[5]. McEvoy SA, Rapid correction of a simple one-tooth anterior cross bite due to an over-retained primary incisor: Clinical reportPediatr Dent 1983 5(4):280-82. [Google Scholar]
[6]. Valentine F, Howitt JW, Implications of early anterior crossbite correctionJ Dent Child 1970 37(5):420-27. [Google Scholar]
[7]. Bayrak S, Tunc ES, Treatment of anterior dental crossbite using bonded resin-composite slopes: case reportsEur J Dent 2008 2:303-07.10.1055/s-0039-169739719212539 [Google Scholar] [CrossRef] [PubMed]
[8]. Profitt WR, Fields HW, Sarve DM, Contemporary Orthodontics 1999 3rd editionSt. Louis, Mo, USAMosby [Google Scholar]
[9]. Major PW, Glover K, Treatment of anterior cross-bites in the early mixed dentitionJ Can Dent Assoc 1992 58(7):574-75.:578-79. [Google Scholar]
[10]. Hannuksela A, Vaananen A, Predisposing factors for malocclusion in 7-year-old children with special reference to atopic diseasesAm J Orthod Dentofacial Orthop 1987 92(4):299-03.10.1016/0889-5406(87)90330-1 [Google Scholar] [CrossRef]
[11]. Olsen CB, Anterior crossbite correction in uncooperative or disabled children. Case reportsAust Dent J 1996 41(5):304-09.10.1111/j.1834-7819.1996.tb03138.x8961603 [Google Scholar] [CrossRef] [PubMed]
[12]. Estreia F, Almerich J, Gascon F, Interceptive correction of anterior crossbiteJ Clin Pediatr Dent 1991 15(3):157-59. [Google Scholar]
[13]. Jacobs SG, Teeth in cross-bite: the role of removable appliancesAust Dent J 1989 34(1):20-28.10.1111/j.1834-7819.1989.tb03000.x2650668 [Google Scholar] [CrossRef] [PubMed]
[14]. Clark WJ, Arch development with transforce lingual appliancesWorld J Orthod 2005 6(1):9-16. [Google Scholar]
[15]. Vadiakas G, Viazis AD, Anterior cross bite correction in the early deciduous dentitionAm J Orthod Dentofacial Orthop 1992 102:160-62.10.1016/0889-5406(92)70029-A [Google Scholar] [CrossRef]
[16]. Park JH, Kim JW, Anterior cross bite correction with a series of clear removable appliances. A Case ReportJ Esthet Rest Dent 2009 21:149-59.10.1111/j.1708-8240.2009.00257.x19508256 [Google Scholar] [CrossRef] [PubMed]
[17]. Sari S, Gopalp H, Aras S, Correction of anterior dental cross bite with composite as an inclined planeInt J Paediatr Dent 2001 11:201-08.10.1046/j.1365-263X.2001.00256.x11484470 [Google Scholar] [CrossRef] [PubMed]
[18]. SI Balaji, Management of CrossbiteIn: Orthodontics The Art and Science 2012 5th edNew DelhiArya Medi:552-55. [Google Scholar]
[19]. Asher RS, Kuster CG, Erikson L, Anterior dental crossbite correction using a simple fixed appliance. A case reportPed Dent 1986 8(1):54-55. [Google Scholar]
[20]. Bourrée F, Michel P, Salmi LR, Consensus methods: Review of original methods and their main alternatives used in public healthRev Epidemiol Sante Publique 2008 56(6):415-23.10.1016/j.respe.2008.09.00619013039 [Google Scholar] [CrossRef] [PubMed]
[21]. Kiyak HA, Patient’s and parent’s expectations from early treatmentAm J Orthod Dentofacial Orthop 2006 129:S50-54.10.1016/j.ajodo.2005.09.01816644418 [Google Scholar] [CrossRef] [PubMed]
[22]. Kocadereli I, Early treatment of posterior and anterior crossbite in a child with bilaterally constricted maxilla: report of caseJ Dent Child 1998 65(1):41-46. [Google Scholar]
[23]. Tse CS, Correction of single tooth anterior crossbiteJ Clin Orthod 1997 31(3):188-90. [Google Scholar]
[24]. Prakash P, Durgesh BH, Anterior crossbite correction in early mixed dentition period using catlan’s appliance: a case reportISRN Dent 2011 :29893110.5402/2011/29893121991464 [Google Scholar] [CrossRef] [PubMed]
[25]. Pinkham JR, Pediatric dentistry: infancy through adolescence 2005 4th edNew DelhiSaunders:642-43. [Google Scholar]
[26]. Kennedy DB, Osepchook M, Unilateral posterior cross bite with mandibular shift: a reviewJ Can Dent Assoc 2005 71(8):569-73. [Google Scholar]
[27]. Croll TP, Riesenberg RE, Anterior cross bite correction in the primary dentition using the fixed inclined plane IIQuintessence Int 1988 19(1):45-51. [Google Scholar]
[28]. Croll TP, Riesenberg RE, Anterior cross bite correction in the primary dentition using the fixed inclined plane IQuintessence Int 1987 18(12):847-53. [Google Scholar]