Complete Spontaneous Resolution of Complex Renal Cyst: A Case Study
Arun Kumar Maurya1, Dilip Kumar Pal2
1 Resident, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
2 Professor and Head, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dilip Kumar Pal, Professor and Head, Department of Urology, Institute of Post Graduate Medical Education and Research, 244, A.J.C. Bose Road, Kolkata-700020, West Bengal, India.
E-mail: urologyipgmer@gmail.com
Renal cysts are the lesion which can bother to patient, treating nephrologists and urologist. Spectrum of presentation ranges from benign to malignant, familial to sporadic. In this case, we present a young 34-year-old female who initially came with a large renal cyst in her left kidney of Bosniak category IIF. Patient was then planned for regular follow up. Subsequent imaging revealed complete regression of the renal cyst.
Cystic, Kidney disease, Neoplasm
Case Report
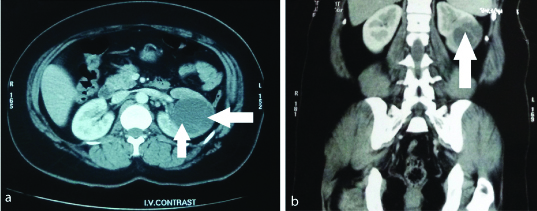
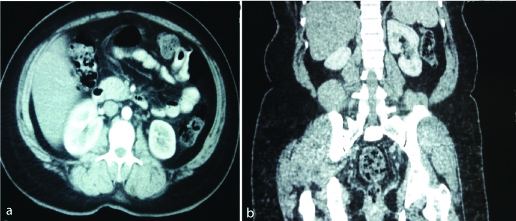
A 33-year-old hypertensive female visited to us with complaint of vague abdominal discomfort. Her abdominal ultrasonography report revealed a large left renal cyst with internal septas. Subsequent Contrast-Enhance Computed Tomography (CECT) imaging reviled a hypodense approx 53×45 mm cystic lesion in the mid cortex, septas were seen in the cyst with peripheral nodularity [Table/Fig-1a,b]. Overlying fat plane and capsule was intact. Her hypertension was managed and we advised her for follow up. Review scan after eight months revealed total resolution of previously detected left renal cyst with no features of any residual or new lesion [Table/Fig-2a,b]. There was no history of trauma, heamaturia or any kind of surgical intervention.
a) Axial section of CECT showing left renal cyst with septa are noted within the lesion along with thickening of the wall of the cyst (white arrow); b) Coronal view enumerating the cyst (white arrow).
a) Axial section of CECT in follow up showing complete resolution of cyst; b) Coronal view in follow up.
Discussion
Renal cysts are quite common radiological diagnosis and they are the most common benign renal lesion. In a 10 years follow up study it was noted that simple renal cyst increases in size and number both [1]. Benign renal cyst and cystic Renal Cell Carcinoma (RCC) differentiation remains the most difficult situation in imaging [2]. For this reason Bosniak developed a CT based classification for renal cysts in terms of likelihood of malignancy and management. Although, partial spontaneous regression of Bosniak category IV has been reported but it is among one of the few cases where complete resolution of large complex cyst has been occurred [3].
Renal cysts are the commonest renal masses and they represent greater than 70% of asymptomatic lesions. They can be considered benign when lacking in internal architecture, no enhancement after IV contrast and thin walls. Currently, Bosniak classification is used to define renal cyst. Bosniak I, II, IIF all are benign lesions. Except II F, no follow up is required. Analysis of septal thickness in lesion of category IIF is very difficult, so any thickness greater than hairline to wall or septum upgrade the cyst from category II to IIF. Although, length of the follow up has yet to be defined but data showed that lesion stable over five years period could be considered benign [4]. It is well reported in the literature that average increase in size of cyst is 1.9 mm/year but there could be increase or decrease in size as the age increases [1]. Resolution of the cyst could be due to spontaneous or traumatic rupture [5]. Although, rare but death also has been reported in the literature due to rupture of the cyst [6]. After diagnosis most of the simple or minimally complex cyst did not require any follow up or treatment [7]. Therapeutic option for benign symptomatic cystic lesion is aspiration sclerotherapy, cyst decortications and surgical resection. In one study where 39 patients of Bosniak category IIF were followed up over average period of 5.8 years, showed decrease of renal cyst size in only three patients [8]. To the best of our knowledge it is the first case report showing Bosniak category IIF cyst which has completely regressed.
Conclusion
Follow up computed tomography imaging is important for management of category IIF renal cyst. Although, rare but complete regression of minimally complex cyst is possible. Since, it is a rare phenomenon studies are lacking for follow up protocol after complete regression of complex cyst.
[1]. Terada N, Arai Y, Kinukawa N, Terai A, The 10-year natural history of simple renal cystsUrology 2008 71(1):7-11.10.1016/j.urology.2007.07.07518242354 [Google Scholar] [CrossRef] [PubMed]
[2]. Bosniak MA, The Bosniak renal cyst classification: 25 years laterRadiology 2012 262(3):781-85.10.1148/radiol.1111159522357882 [Google Scholar] [CrossRef] [PubMed]
[3]. Weibl P, Lutter I, Romancik M, Karwandgar M, Kollarik B, Obsitnik M, Spontaneous regression of complex cystic renal mass of bosniak class IV-a rare phenomenonBratisl Lek Listy 2009 110(3):195-96. [Google Scholar]
[4]. Gary M, Morton A, Bosniak Follow-up CT of moderately complex cystic lesions of the kidney (Bosniak Category IIF)Am J Roengenol 2003 181(3):627-33.10.2214/ajr.181.3.181062712933451 [Google Scholar] [CrossRef] [PubMed]
[5]. Papanicolaou N, Pfister RC, Yoder IC, Spontaneous and traumatic rupture of renal cyst: diagnosis and outcomeRadiology 1986 160(1):99-103.10.1148/radiology.160.1.37150543715054 [Google Scholar] [CrossRef] [PubMed]
[6]. Rainio J, De Giorgio F, Carbone A, Death from renal cyst: spontaneous or traumatic rupture?Am J Forensic Med Pathol 2006 27(2):193-95.10.1097/01.paf.0000220918.46766.f816738445 [Google Scholar] [CrossRef] [PubMed]
[7]. Eknoyan G, A clinical view of simple and complex renal cystsJ Am Soc Nephrol 2009 20(9):1874-76.10.1681/ASN.200804044118776117 [Google Scholar] [CrossRef] [PubMed]
[8]. Cameron LB, Jiang DH, Moodie K, Mitchell C, Solomon B, Parameswaran BK, Crizotinib Associated Renal Cysts (CARCs): incidence and patterns of evolutionCancer Imaging 2017 17(1):710.1186/s40644-017-0109-528209203 [Google Scholar] [CrossRef] [PubMed]