Acute Amoebic Appendicitis: A Rare Case Report
Manjari Kishore1, Devender Singh Chauhan2, Seema Rahar3, Shashikant Singh4
1 Senior Resident, Department of Pathology, Postgraduate Institute of Medical Education and Research, Dr. Ram Manohar Lohia Hospital, Delhi, India.
2 Assistant Professor, Department of Pathology, Postgraduate Institute of Medical Education and Research, Dr. Ram Manohar Lohia Hospital, Delhi, India.
3 Junior Resident, Department of Pathology, Postgraduate Institute of Medical Education and Research, Dr. Ram Manohar Lohia Hospital, Delhi, India.
4 Junior Resident, Department of Pathology, Postgraduate Institute of Medical Education and Research, Dr. Ram Manohar Lohia Hospital, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Devender Singh Chauhan, Room No. 405, PGI Building, Postgraduate Institute of Medical Education and Research, Dr. Ram Manohar Lohia Hospital, Delhi-110001, India.
E-mail: drdsc1318@gmail.com
Acute appendicitis is a common cause of acute pain abdomen. Amoebic infestation is still a rare cause of acute appendicitis. Herein, we report a rare case of amoebic appendicitis in a young female, who presented to emergency department with pain abdomen, fever and vomiting along with rebound tenderness. Laboratory investigation revealed leukocytosis and mild eosinophilia. Histopathological examination showed numerous trophozoites of Entamoeba histolytica in the ulcerated mucosa of the appendix. The present case report aim to highlight this rare cause of appendicitis which should be treated appropriately to prevent further complication.
Appendix, Entamoeba histolytica, Pain abdomen
Case Report
A 28-year-old female presented to hospital with acute pain abdomen and vomiting along with fever for last seven days. General examination revealed increased temperature (39.8°C) and pulse rate (108/minute). Abdominal examination showed signs of tenderness in right iliac fossa with rebound tenderness and rigidity.
Complete blood count revealed haemoglobin 11.8 gm/dL, total leukocyte count 18,500/μL with neutrophilia. Rest of the haematological and biochemical parameters were within normal limit. Clinically, a provisional diagnosis of acute appendicitis was made and appendicectomy was done. An inflamed appendix with attached mesoappendix was found. No perforation was noted. The postoperative period was uneventful, and patient recovered well.
Grossly, specimen of appendix with mesoappendix measuring 6.5 cm in length was received in 10% buffered formalin [Table/Fig-1a]. The serosa showed focal exudates and congestion. On cut section, lumen filled with faecal matter was identified. Mucosa showed ulceration and focally purulent areas. Multiple sections were made and routinely processed.
a) Gross image of resected specimen of appendix (cut section showing the lumen); b) Section showing ulcerated mucosa, focal lymphoid hyperplasia (H&E, 10X); c) Photomicrograph revealing numerous trophozoites of Entamoeba histolytica with single nucleus and vacuolated cytoplasm, few showing erythrophagocytosis (H&E, 40X); d) Periodic acid schiff stain positivity confirming the organisms are amoebic trophozoites (PAS, 40X).
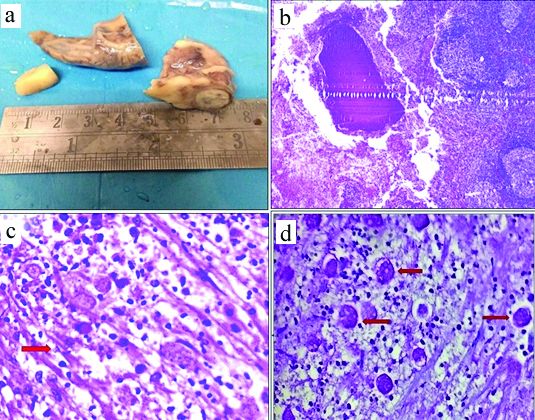
Examination of section showed extensive areas of mucosal ulceration and focally preserved mucosa along with focal lymphoid hyperplasia and mixed inflammatory infiltrate comprising of neutrophils, eosinophils and few lymphocytes [Table/Fig-1b]. Numerous, single and small groups of trophozoites of Entamoeba histolytica were also noted in the ulcerated lumen [Table/Fig-1c]. Most of the trophozoites showed evidence of erythrophagocytosis. The wall of the appendix also showed mixed acute and chronic inflammatory infiltrates along with eosinophils. No evidence of periappendicitis was noted. The trophozoite forms were highlighted using special stains, Periodic Acid Schiff (PAS) [Table/Fig-1d]. A final diagnosis of “Acute Amoebic Appendicitis” was given.
Discussion
Acute appendicitis is the most common surgical emergency noted in patients who come with acute pain abdomen [1]. The usual cause is obstruction due to fecolith which acts as inciting factor of inflammation. Rarely, parasitic infections can lead to acute appendicitis [1,2]. Though, the exact pathogenesis is not determined but it is thought that these parasites lead to mucosal invasion and luminal obstruction [2,3].
Various parasites which can cause appendicitis are Enterobius vermicularis, Entamoeba, Ascaris, Taenia, Schistosomiasis, Trichuris [2]. The pinworm, also known as Enterobius vermicularis is most common parasite causing appendicitis. Its incidence in resected appendicectomy specimen is 1-4%, but all cases do not show evidence of inflammation. Its exact role is debatable as it may be an incidental finding [1-3].
Entamoeba histolytica appendicitis is very rare and reported only in 0.5-2% of appendicitis cases in young adults and that too in an endemic zone [4]. A very few cases of acute amoebic appendicitis have been reported in literature. It is also noted in paediatric age group [4,5]. Guzmán-Valdivia G, noted a higher rate with 2.3% in their large series [5].
Acute appendicitis is found in places with poor hygiene which leads to ingestion of parasite in cyst form which thereafter changes into trophozoites [2,4]. These trophozoites form initially remain localised in the lumen and then invade the wall and form ameboma, a chronic inflammatory focus. This may cause acute pain abdomen which resembles acute appendicitis. Sometimes, these trophozoites can reach to liver and other organs through portal vein [3-5].
Laboratory investigations which help in diagnosis of amoebiasis are stool examination, serological tests, culture and imaging studies. However, the gold standard diagnostic modality is the demonstration of haematophagous trophozoites of Entamoeba histolytica in histological sections of appendix [2-6]. Patient in the present study did not present with diarrhoea, which represents the rare form of amoebic appendicitis as it was confined only to the appendix. Histological sections taken from proximal part of appendix did not show any trophozoite.
The treatment of choice is surgical removal of appendix with appropriate antimicrobials [5-7]. In the present case, patient was immediately started on ‘metronidazole tablet’, after the diagnosis of amoebic appendicitis, recovered uneventfully. As, appendicectomy removes the focus of parasitic infection in cases where infection is localised to appendix only, morbidity was much less [6-7].
Conclusion
The present case highlights the importance of histopathological examination and identification of amoebic trophozoite, as one of the rare causative agents of acute appendicitis. Appendicectomy along with timely use of antimicrobials can reduce the incidence of septic complication in the patient. To conclude, it is the combined clinicopathological approach which help in identifying this rare cause of appendicitis and hence, managing the patient properly.
[1]. Yildirim S, Nursal TZ, Tarim A, Kayaselcuk F, Noyan T, A rare cause of acute appendicitis: parasitic infectionScand J Infect Dis 2005 10:757-59.10.1080/0036554051001216116191896 [Google Scholar] [CrossRef] [PubMed]
[2]. Chamisa I, A clinicopathological review of 324 appendices removed for acute appendicitis in Durban, South Africa: a retrospective analysisAnn R Coll Surg Engl 2009 91:688-92.10.1308/003588409X1248616752167719909612 [Google Scholar] [CrossRef] [PubMed]
[3]. Akbulut S, Tas M, Sogutcu N, Arikanoglu Z, Basbug M, Ulku A, Unusual histopathological findings in appendectomy specimens: a retrospective analysis and literature reviewWorld J Gastroenterol 2011 15:1961-70.10.3748/wjg.v17.i15.196121528073 [Google Scholar] [CrossRef] [PubMed]
[4]. Singh NG, Mannan AA, Kahvic M, Acute amoebic appendicitis: report of a rare caseIndian J Pathol Microbiol 2010 53:767-68.10.4103/0377-4929.7208021045411 [Google Scholar] [CrossRef] [PubMed]
[5]. Guzmán-Valdivia G, Acute amebic appendicitisWorld J Surg 2006 30:1038-42.10.1007/s00268-005-0104-z16736334 [Google Scholar] [CrossRef] [PubMed]
[6]. Zardawi IM, Kattampallil JS, Rode JW, Amoebic appendicitisMed J Aust 2003 178:523-24.10.5694/j.1326-5377.2003.tb05335.x12741945 [Google Scholar] [CrossRef] [PubMed]
[7]. Ito D, Hata S, Seiichiro S, Kobayashi K, Teruya M, Kaminishi M, Amebiasis presenting as acute appendicitis: Report of a case and review of Japanese literatureInt J Surg Case Rep 2014 5:1054-57.10.1016/j.ijscr.2014.10.03525460473 [Google Scholar] [CrossRef] [PubMed]