“Head Over Heels” Position of Duodenum-A Unique Congenital Anomaly
Satheesha B Nayak1, Sudarshan Surendran2, Prakashchandra Shetty3, Surekha D Shetty4
1 Professor, Department of Anatomy, Melaka-Manipal Medical College (Manipal Campus), Manipal Academy for Higher Education, Manipal, Karnataka, India.
2 Associate Professor, Department of Anatomy, Melaka-Manipal Medical College (Manipal Campus), Manipal Academy for Higher Education, Manipal, Karnataka, India.
3 Associate Professor, Department of Anatomy, Melaka-Manipal Medical College (Manipal Campus), Manipal Academy for Higher Education, Manipal, Karnataka, India.
4 Assistant Professor, Department of Anatomy, Melaka-Manipal Medical College (Manipal Campus), Manipal Academy for Higher Education, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satheesha B Nayak, Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal Academy for Higher Education, Madhav Nagar, Manipal, Udupi-576104, Karnataka, India.
E-mail: nayaksathish@gmail.com
Knowledge of congenital anomalies of duodenum and biliary apparatus is useful in radiological diagnosis and surgical procedures of upper abdominal region. We present concurrent variations of duodenum, bile duct and coeliac trunk in this report. The first part of the duodenum descended downwards in front of the head of the pancreas. At the lower end of the head of the pancreas, it ascended upwards along the right border of the head of the pancreas until the first lumbar vertebra. At the level of first lumbar vertebra, it continued to the left as its third part. The third and fourth part passes behind the head, neck and the body of the pancreas (and also behind superior mesenteric vessels). On the left side of the second lumbar vertebra, the duodenum continued as jejunum at the duodenojejunal flexure. The common bile duct coursed down in front of the head of the pancreas, being surrounded by a few pancreatic acini in the lower part of its course. It terminated at the hepatopancreatic ampulla, which opened into the first part of the duodenum. The coeliac trunk passed through the body of the pancreas before it divide into its terminal branches.
Bile duct, Coeliac trunk, Intestine, Pancreas
Case Report
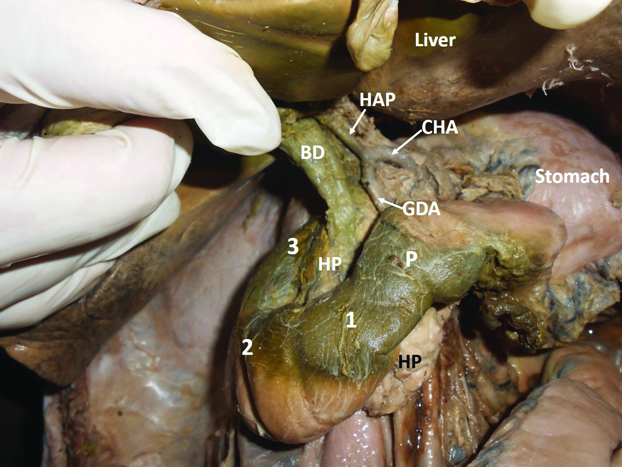
A cadaveric dissection class was conducted for medical undergraduates and during that a unique congenital anomaly of the duodenum in relation to the pancreas was observed and we would like to call this as “head over heels” position of duodenum. This variation was noted in a South Indian male cadaver aged approximately 70 years. The stomach was normal in terms of size and position. Its pyloric end was situated over the neck of the pancreas. The first part of the duodenum descended downward and to the right over the head of the pancreas. After reaching the lower end of the head of the pancreas (at the level of third lumbar vertebra), it ascended upwards along the right border of the head of the pancreas until the first lumbar vertebra. At the level of first lumbar vertebra, it turned downward and to the left and continued as its third part. The second part was slightly dilated. The third and fourth parts ran obliquely downward and to the left, behind the head, neck and the body of the pancreas (and also behind superior mesenteric vessels). On the left side of the second lumbar vertebra, the duodenum continued as jejunum at the duodenojejunal flexure. Thus, the upper border of the pancreas was related to the third part, lateral border to the second part and the inferior border was related to the first part of the duodenum. The common bile duct coursed down in front of the head of the pancreas, being surrounded by a few pancreatic acini in the lower part of its course. It terminated at the hepatopancreatic ampulla, which opened into the first part of the duodenum, adjacent to the pyloroduodenal junction. Thus, the bile duct was not covered by any part of the duodenum. The coeliac trunk passed through the body of the pancreas before it divided into its terminal branches. The variations observed have been shown in [Table/Fig-1,2 and 3].
Dissection of the upper abdomen showing the relationship of the duodenum with the pancreas.
1-First part of the duodenum; 2-Second part of the duodenum; 3-Third part of the duodenum; P-Pyloric part of the stomach; HP-Head of the pancreas; CHA-Common hepatic artery; HAP-Hepatic artery proper; BD-Bile duct; GDA-Gastroduodenal artery
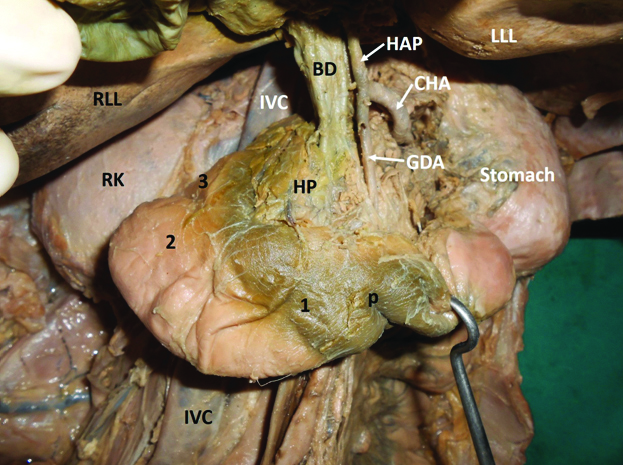
Pyloric part of the stomach has been pulled down to show the head of the pancreas and the parts of duodenum.
RLL-Right lobe of liver; LLL-Left lobe of liver; RK-Right kidney; IVC-Inferior vena cava; 1-First part of the duodenum; 2-Second part of the duodenum; 3-Third part of the duodenum; P-Pyloric part of the stomach; HP-Head of the pancreas; CHA-Common hepatic artery; HAP-Hepatic artery proper; BD-Bile duct; GDA-Gastroduodenal artery
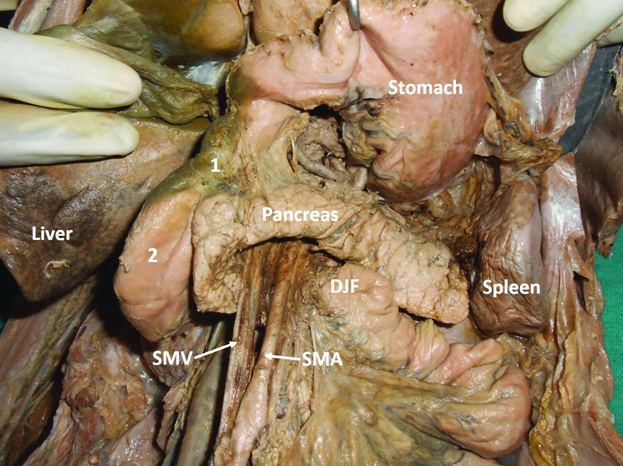
Stomach has been pulled upwards to show the pancreas and duodenojejunal flexure.
1-First part of the duodenum; 2-Second part of the duodenum; SMV-Superior mesenteric vein; SMA-Superior mesenteric artery; DJF-Duodenojejunal flexure
Discussion
Duodenum, pancreas and coeliac trunk are closely associated with each other anatomically, functionally and developmentally, but the combined congenital anomalies of all the three are extremely rare. Annular pancreas is one of the congenital anomalies where the head of the pancreas surrounds the second part of the duodenum like a ring. This ring of pancreatic tissue may be complete, partial or double [1-3]. Atresia or stenosis of duodenum may occur independently or in association with annular pancreas. Duplication and malrotation of the duodenum are two other known variations of the duodenum [4]. Developmental anomalies of the common bile duct are very few. It may be absent or duplicated [5,6]. Coeliac trunk shows many variations in its origin and branching pattern, but it rarely passes through the pancreas.
Developmental anomalies of duodenum and pancreas may cause severe problems at any stage of life. Knowledge of developmental anomalies is not only useful in diagnosis and treatment of the problems caused by the anomaly, but also crucial in avoiding iatrogenic injuries. Most of the anomalies of gastrointestinal tract can be detected radiologically. The retroperitoneal position of the third part of the duodenum is considered as the indicator of normal gut rotation by radiologists but in some types of malrotations of intestine also the third part of the duodenum might be retroperitoneal [7,8]. Reports on duodenal variation are scanty. One of the reports published recently describes the serpent like coiling of midgut segment of the second part of the duodenum [9]. The present case of complete “head over heel” position of duodenum is quite unique and first to be included in the literature. The second part of duodenum in the present case was ascending upwards and the third part was passing behind the head, neck and body of pancreas obliquely. Probably, due to the sustained compressive effect of pancreas on the third part, the second part was dilated. Usually duodenal loop falls to the right and loses its dorsal mesentery due to zygosis. The embryological reason for this anomaly could be the fall of duodenal loop in forward and downward direction during its development. This forward and downward fall of the loop would have brought the first part down and the third part up.
The common bile duct is formed by the union of cystic duct and common hepatic duct, just below the porta hepatis. It passes through the right free margin of the lesser omentum, behind the first part of duodenum and head of the pancreas. It joins with the pancreatic duct to form the hepatopancreatic ampulla, which in turn opens into the second part of the duodenum. In the present case, the common bile duct passed in front of the third part of the duodenum and head of the pancreas. The hepatopancreatic ampulla opened into the first part of the duodenum. This is another unique feature of the present case. There is one earlier report on opening of the bile duct into the pyloric ring [10]. But there are no reports on a case similar to the one presented here.
There are reports on pancreatic tissue surrounding the coeliac trunk and portal vein. However, coeliac trunk being completely embedded in the body of pancreas is rare. In the present case, the coeliac trunk passed through the body of the pancreas. Thus, the present case is a combination of the three rare anomalies in the same cadaver.
Conclusion
In the present case, the position of the duodenum might misguide the radiologist as it is a rare variation. Visualisation of first and second parts in the present case may be difficult because of the downward course of the first part of the duodenum. The first and second part in this case are overlapped by the coils of jejunum. Hence, the classic “duodenal cap” of radiologist should also be absent. For the surgeons, the case could prove to be challenging due to the passage of coeliac trunk through the pancreas and the anteriorly placed bile duct. Usually, the cancer of the head of the pancreas leads to obstructive jaundice due to the compression on bile duct. But in the present case, due to the anteriorly placed bile duct, obstructive jaundice might not develop. The knowledge of this variation could be useful during procedures like gastroscopy, gastrojejunostomy, pancreatic surgeries and many other radiological procedures.
[1]. Nayak BS, Yooi OM, A classic case of annular pancreas and its clinical implicationsInt J Morphol 2011 29(2):559-61.10.4067/S0717-95022011000200043 [Google Scholar] [CrossRef]
[2]. Nayak BS, Kumar N, Sirasanagandla SR, Swamy RS, Surendran S, Half annular pancreas-a cadaveric case reportEL Mednifico Journal 2014 2(4):01-02.10.18035/emj.v2i4.346 [Google Scholar] [CrossRef]
[3]. Nayak S, Pamidi N, George BM, Guru A, A strange case of double annular pancreasJOP 2013 14(1):96-98. [Google Scholar]
[4]. Yan X, Fan Y, Wang K, Zhang W, Song Y, Duodenal duplication manifested by abdominal pain and bowl obstruction in an adolescent: a case reportInt J Clin Exp Med 2015 8(11):21710-14. [Google Scholar]
[5]. Mittal T, Pulle MV, Dey A, Malik VK, Congenital absence of the common bile duct: a rare anomaly of extrahepatic biliary tractJ Minim Access Surg 2016 12(3):281-82.10.4103/0972-9941.18129227279403 [Google Scholar] [CrossRef] [PubMed]
[6]. Chin JL, Sengupta S, Morrin MM, Murray FE, Patchett SE, Common bile duct duplication: double bile ducts, double troubleGastrointest Endosc 2017 85(4):855-56.10.1016/j.gie.2016.05.00527179690 [Google Scholar] [CrossRef] [PubMed]
[7]. Menten R, Reding R, Godding V, Dumitriu D, Clapuyt P, Sonographic assessment of the retroperitoneal position of the third portion of the duodenum: an indicator of normal intestinal rotationPediatr Radiol 2012 42(8):941-45.10.1007/s00247-012-2403-522684229 [Google Scholar] [CrossRef] [PubMed]
[8]. Yousefzadeh DK, The position of the duodenojejunal junction: the wrong horse to bet on in diagnosing or excluding malrotationPediatr Radiol 2009 39(Suppl 2):S172-77.10.1007/s00247-008-1116-219308381 [Google Scholar] [CrossRef] [PubMed]
[9]. Lalwani R, Athavale S, Kotgirwar S, A rare anomaly of duodenum: a case reportActa Med Iran 2016 54(10):686-89.10.1016/j.jasi.2016.08.410 [Google Scholar] [CrossRef]
[10]. Kobayashi S, Hoshino H, Segami K, Koizumi S, Ooike N, Otsubo T, Incomplete annular pancreas with ectopic opening of the pancreatic and bile ducts into the pyloric ring: first report of a rare anomalyCase Rep Gastroenterol 2016 10(2):373-80.10.1159/00044729227721721 [Google Scholar] [CrossRef] [PubMed]