Dermatoglyphics and Alcohol-Tobacco Consumption
Goutham Gandham1, K Thajuddeen2
1 Junior Resident, Department of General Medicine, Kasturba Medical College, Mangaluru, Karnataka, India.
2 Associate Professor, Department of General Medicine, Kasturba Medical College, Mangaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. K Thajuddeen, Legacy Complex, Above Dominos Pizza, Bendoorwell, Kankanady, Mangaluru-575002, Karnataka, India.
E-mail: thajdr@yahoo.in
Introduction
Epidermal ridge patterns form early in foetal development which remains unchanged throughout life and hence they can be used to indicate genetic abnormalities. Several studies indicate that alcohol-tobacco consumption has a genetic component.
Aim
To compare the dermatoglyphic patterns in alcohol and/or tobacco consumers with non consumers and to identify dermatoglyphic patterns which are peculiar to alcohol and/or tobacco consumers if any.
Materials and Methods
In present study 250 cases of alcohol and/or tobacco use disorder individuals were studied for dermatoglyphic parameters such as ‘ATD’ angle and the patterns of fingerprints. These cases were compared with 250 non consumers and analysed for statistical significance. Quantitative variables (‘ATD’ angle) were analysed using Student’s t-test and qualitative variables (fingerprint patterns) by Chi-square test. A p-value less than 0.05 was considered as significant.
Results
In present study, there was a decrease in ‘ATD’ angle in both hands of male (p<0.001) and female (p<0.001) cases as compared to controls which was statistically highly significant. In our study we noticed that percentage of ulnar loops (p=0.020), arches (p=0.010) and composite patterns (p=0.005) are less among male cases compared to male controls, which was statistically significant. Percentage of whorls was more among male cases compared to male controls which was statistically highly significant (p<0.001). Percentage of radial loops was more among female cases compared to female controls, which wasstatistically significant (p=0.017).
Conclusion
In the present study an association was observed between palmar dermatoglyphics and alcohol-tobacco consumption. Dermatoglyphics by itself is not enough to diagnose alcohol-tobacco abuse individuals, but the results of this work may serve to strengthen the diagnostic criteria.
Alcohol use disorder, ATD angle, Tobacco use disorder
Introduction
The term “Dermatoglyphics” (from the Greek, derma = skin, glyphe= carving) was coined by Prof. Harold Cummins [1]. Dermatoglyphics is the analysis of dermal ridges and their configurations by studying prints of them [2]. Distortion in the alignment of dermal ridges due to abnormal growth processes which are the result of the action of abnormal genes or aberrations in chromosomes or due to unknown causes. Characteristic dermatoglyphic patterns that deviate from the normal patterns are due to the changes which occur before fourth foetal month [3].
Many authors reported the presence of peculiar dermatoglyphic patterns in genetic disorders, malignancies and some idiopathic disorders [4-7]. Dermatoglyphics is one such investigation which is cost effective, non invasive and easy but can predict possible future illnesses.
Alcohol and tobacco consumption is one of the major public health issue which impacts society at various levels. Directly or indirectly alcohol and tobacco abuse affects every community. Alcohol and tobacco use poses a significant threat to health. Worldwide alcohol and tobacco use is estimated to be two billion alcohol users and 1.3 billion tobacco users [8]. As everyone is not at equal risk to develop other chronic diseases, only a few people who use drugs will be addicted. Susceptibility of people to get addicted differs because they differ in developmental, genetic, social and environmental factors. Many environmental, social and genetic factors of a person determines his or her unique susceptibility of using drug initially, then sustaining drug use, and later brain undergoes progressive changes that characterise addiction [9].
This study of palmar dermatoglyphics and alcohol-tobacco consumption aims to be a ready reckoner to predict addiction prone individuals and measures can be offered to such individuals to prevent them from falling prey to addiction. There is need for early intervention at primordial level. Early detection is of great significance and hence the importance of this study, which could be a potential tool in the early detection or prediction of alcohol-tobacco, uses prone individuals. Early intervention in form of counseling, life style changes, behaviour therapy can be of immense help in reducing morbidity and mortality.
Prevention is better than cure; as the saying goes, this new field of scientific interpretation of fingerprints will predict many diseases and their complications. The present study was undertaken for an immense wealth of information and it will add on to the existing knowledge.
Materials and Methods
A hospital based comparative case-control study was conducted from November 2014 to August 2016. Sample population was selected from outpatient and inpatient clinics of Kasturba Medical College teaching hospitals, Mangaluru, Karnataka, India. A sample size of 500, with 250 cases and 250 controls was taken with a confidence level of 95% and power of 90%.
Sampling procedure was convenience sampling. Individuals age more than 18 years and less than 60 years with history of only alcohol or only tobacco or both alcohol and tobacco consumption and fit into DSM-V criteria for tobacco use disorder and/or alcohol use disorder after taking written informed consent, were included [10,11]. Control group consisted of age and sex matched (±2 years) individuals without present or past history of alcohol or tobacco consumption. Patients who have either traumatic or exfoliative lesions which can mask the palm creases were excluded from the study.
Approval from Institutional Ethical Committee was taken before starting the study. After wiping the hands clean, the patient places both his hands over the scanner screen and a digital image of the same was obtained [Table/Fig-1].

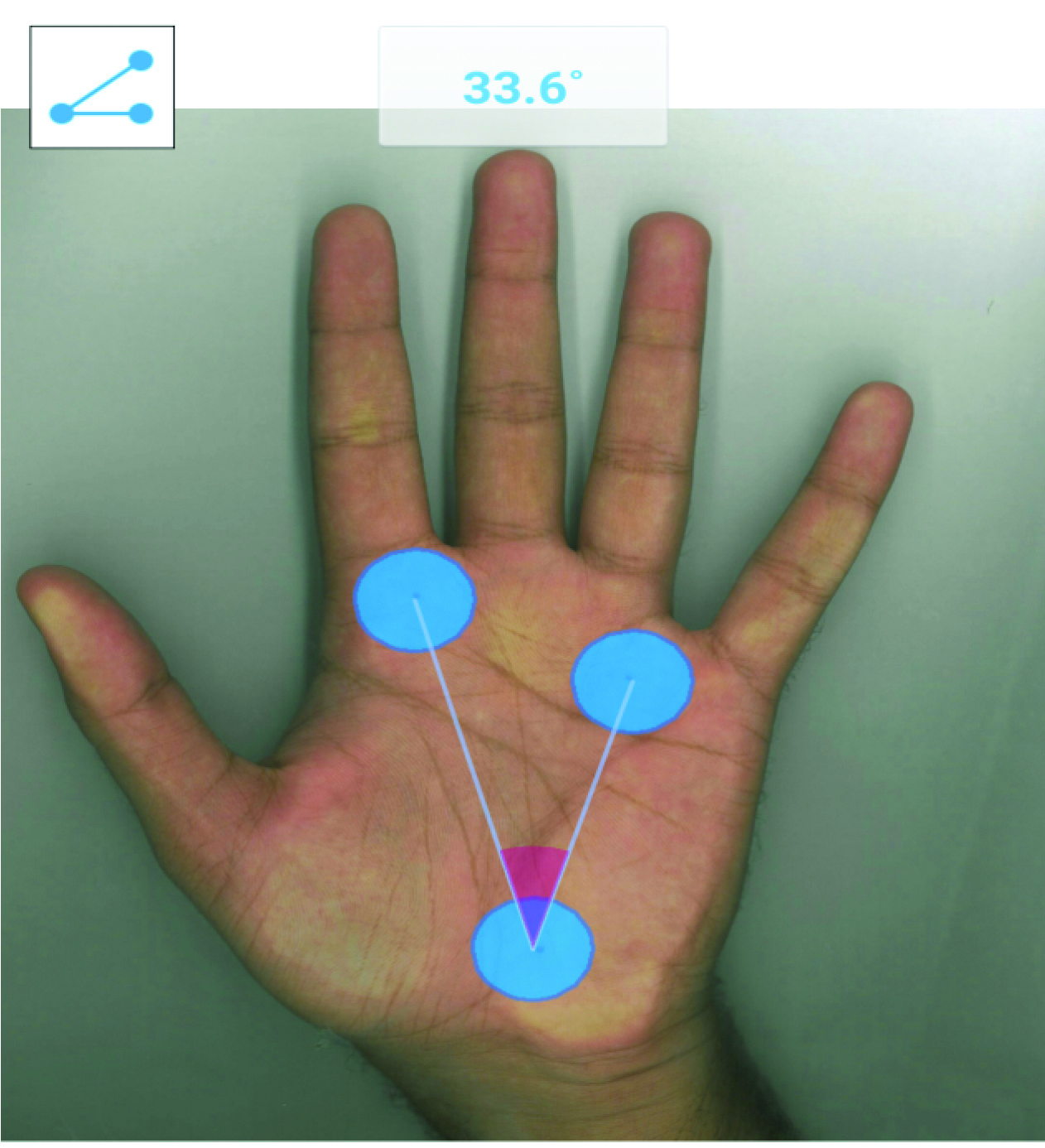
A separate image was obtained for the two thumbs. The images so scanned were stored for analysis. The patterns were read under direct visualisation. The ‘ATD’ angle is calculated using the screen protractor software [Table/Fig-2].
‘ATD’ angle using screen protractor software.
The data were analysed based on qualitative and quantitative parameters. Quantitative parameter is measuring ‘ATD’ angle and qualitative parameters were the patterns of digital print namely radial loop, ulnar loop, arch, whorl, and composite.
Statistical Analysis
Data pertaining to the fingerprints were obtained and entered into an excel spread sheet and imported to statistical software SPSS version 16.0. Quantitative variables were analysed using Student’s t-test and qualitative variables by Chi-square test. A p-value less than 0.05 was considered as significant.
Results
A total of 250 cases and same number of controls were taken for the study. Out of 250 cases (males=175, females=75). Out of 250 controls (males=175, females=75).
In the present study on comparison of ‘ATD’ angle [Table/Fig-3] in male cases with controls, right mean ‘ATD’ angle was 36.232±1.173 among cases and 38.58±2.183 among controls which was statistically highly significant with p-value of <0.001. Left mean ‘ATD’ angle was 36.15±1.148 among cases and 38.87±1.987 among controls which was statistically highly significant with p-value of <0.001. On comparing ‘ATD’ angle in female cases with controls, right mean ‘ATD’ angle was 35.188±0.887 among cases and 40.485±1.659 among controls which was statistically highly significant with p-value of <0.001. Left mean ‘ATD’ angle was 35.24±0.903 among cases and 40.48±1.626 among controls which was statistically highly significant with p-value of <0.001. [Table/Fig-4] shows comparison of qualitative parameters of male and female cases with respective control by applying Chi-square test. A p-value less than 0.05 were considered as significant.
Comparision of ‘ATD’ angle of male and female cases with respective controls by applying Student’s t-test.
| Sex | Hand | Cases | Controls | p-value |
|---|
| Mean ‘ATD’ | SD | Mean ‘ATD’ | SD |
|---|
| Male | Right ‘ATD’ | 36.232 | 1.173 | 38.58 | 2.183 | <0.001 |
| Left ‘ATD’ | 36.15 | 1.148 | 38.87 | 1.987 | <0.001 |
| Female | Right ‘ATD’ | 35.188 | 0.887 | 40.485 | 1.659 | <0.001 |
| Left ‘ATD’ | 35.24 | 0.903 | 40.48 | 1.626 | <0.001 |
A p-value less than 0.05 was considered as significant.
Comparison of qualitative parameters of male and female cases with respective control by applying Chi-square test.
| Sex | Pattern | Percentage of fingerprint pattern within group | p-value |
|---|
| Cases | Controls |
|---|
| % (n) | % (n) |
|---|
| Male | Ulnar loop | 55.2% (966) | 58.6% (1026) | 0.020 |
| Radial loop | 3.2% (56) | 3.0% (53) | 0.385 |
| Whorl | 34.8% (609) | 28.3% (495) | <0.001 |
| Arch | 4.8% (84) | 6.6% (116) | 0.010 |
| Composite | 2.0% (35) | 3.4% (60) | 0.005 |
| Female | Ulnar loop | 55.6% (417) | 59.1% (443) | 0.087 |
| Radial loop | 5.6% (42) | 3.3% (25) | 0.017 |
| Whorl | 31.6% (237) | 29.7% (223) | 0.217 |
| Arch | 5.6% (42) | 5.9% (44) | 0.412 |
| Composite | 1.6% (12) | 2.0% (15) | 0.280 |
A p-value less than 0.05 were considered as significant.
Discussion
In present study 250 cases of alcohol and/or tobacco use disorder individuals were studied for dermatoglyphic parameters such as ‘ATD’ angle and the patterns of fingerprints. These parameters of cases were compared to those of 250 non consumers and analysed for statistical significance. Quantitative variables (‘ATD’ angle) were analysed using Student’s t-test and qualitative variables (fingerprint patterns) by Chi-square test. A p-value less than 0.05 was considered as significant.
In present study there was a decrease in ‘ATD’ angle in both hands of male (p<0.001) and female (p<0.001) cases as compared to controls which is statistically highly significant. In our study we noticed that percentage of ulnar loops (p=0.020), arches (p=0.010) and composite patterns (p=0.005) are less among male cases compared to male controls, which is statistically significant. Percentage of whorls is more among male cases compared to male controls which are statistically highly significant (p<0.001). Percentage of radial loops are more among female cases compared to female controls, which is statistically significant (p=0.017).
According to National Family Health Survey-4; prevalence of alcohol consumption in Karnataka state is 29.3% among males and 1% among females. Prevalance of tobacco consumption is 4.2% among females and 34.3% among males [12]. Studies have been done earlier in the field of dermatoglyphics pertaining to the conditions like diabetes mellitus, hypertension, and obesity. There were only few studies done so far to establish a direct connection between alcohol or tobacco consumption and dermatoglyphics [13,14]. Recent studies suggest that common genetic factors may make people vulnerable to both alcohol and tobacco addiction [15]. Clearly, both alcohol and nicotine dependence runs in families. Identical twins (who share 100 percent of their DNA) are twice as likely as fraternal twins (who, like all siblings, share 50 percent of their DNA) to be nicotine and alcohol dependent if the other twin is dependent [16,18]. The collaborative study on the genetics of alcoholism, the first study to examine the human genetic makeup (or genome) for regions that involve both alcohol dependence and smoking, has identified genes and regions of genes that may be involved in both alcohol and nicotine dependence [19]. This suggests that some overlap may exist between genes that code for sensitivity to alcohol and those that influence sensitivity to nicotine [20]. In a study done by Howard LA et al., on CYP2E1*1D regulatory polymorphism: association with alcohol and nicotine dependence the CYP2E1*1D genotype was associated with alcohol as well as nicotine dependence [21]. In a study done by True WR et al., suggests a common genetic vulnerability to nicotine and alcohol dependence in men [22].
The fingerprint patterns were obtained using a digital data scanner and a laptop computer on to which the digital images of palm were recorded directly. The images obtained were of good resolution and can be enlarged to simplify the analysis, an advantage over the conventional methods. In the present study, we observed a significant decrease in ‘ATD’ angle of both hands of male and female cases as compared to respective controls. Our observations regarding ‘ATD’ angle in cases were in contrast to study done by Devčić S et al., in Croatia on dermatoglyphics in alcoholic patients in which there was no connection between ‘ATD’ angles in the alcoholic and comparison groups [13]. Our observations regarding ‘ATD’ angle in tobacco consumers were similar as in a study done by Vijayaraghavan A and Aswath N, on palmar dermatoglyphics among smokeless tobacco users in Tamil Nadu where there was a decrease in mean ‘ATD’ angle (p<0.001) among smokeless tobacco users. In this study, it was observed that percentage of ulnar loops, arches and composite patterns were less among male cases compared to male controls, which was statistically significant [14]. Percentage of whorls were more among male cases compared to male controls which was statistically highly significant (p<0.001). Percentage of radial loops were slightly more among male cases compared to male controls, which was statistically not significant (p=0.385). Percentage of radial loops was more among female cases compared to female controls, which was statistically significant. In our study, we noticed that percentage of ulnar loops, arches and composite patterns were less among female cases compared to female controls, which was statistically not significant. Percentage of whorls were more among female cases compared to female controls which were statistically not significant. In this study, observations regarding fingerprint pattern in cases were in contrast to study done by Devčić S et al., in Croatia on dermatoglyphics in alcoholic patients in which there was no connection between fingerprint patterns in the alcoholic and comparison groups [13]. In this study observations regarding fingerprint patterns in cases were in contrast to study done by Vijayaraghavan A and Aswath N, on palmar dermatoglyphics among smokeless tobacco users in Tamil Nadu where it was found that there was predominance of loops (p<0.01) and arches (p=0.003) [14].
In the present study large sample size was taken which included 250 cases and 250 controls. Very few studies were done comparing dermatoglyphic patterns of alcohol or tobacco abuse individuals with normal subjects worldwide [13,14].
Limitation
Total finger ridge count and ab ridge count (other quantitative parameters) were not included in the study.
Conclusion
In conclusion, it has been observed that there were statistically significant differences in both qualitative and quantitative dermatoglyphic patterns in alcohol-tobacco consumers compared to normal population. The findings of this work demonstrate the association between some of the dermatoglyphic patterns and alcohol-tobacco abuse suggesting that dermatoglyphics can represent an anatomical, non invasive, inexpensive tool for screening high risk population and this facilitates early detection and management. This study is an eye opener and provides a new insight on genetic influence and thus demands the need for further study in this field. This difference may be attributed to the genotypic differences which exist in the different groups on whom this study was conducted. The present study can be used as a screening tool for the diagnosis of individuals who are more prone for alcohol and tobacco addiction.
A p-value less than 0.05 was considered as significant.
A p-value less than 0.05 were considered as significant.
[1]. Mavalwala J, Harold Cummins-and the birth, growth and development of dermatoglyphicsAm J Phys Anthropol 1975 42(2):177-81.10.1002/ajpa.1330420203123415 [Google Scholar] [CrossRef] [PubMed]
[2]. Williams PT, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Ferguson MWJ, Gray’s Anatomy 1995 Churrchill Livingstone [Google Scholar]
[3]. Johnson J, Dermatoglyphics-quantitative analysis in rheumatoid arthritisAnthropologist 2008 10(3):233-35.10.1080/09720073.2008.11891054 [Google Scholar] [CrossRef]
[4]. Woolf CM, Gianas AD, A study of fluctuating dermatoglyphic asymmetry in the sibs and parents of cleft lip propositiAm J Hum Genet 1977 29(5):503 [Google Scholar]
[5]. Oladipo GS, Olabiyi O, Oremosu AA, Noronha CC, Okanlawon AO, Paul CU, Sickle-cell anaemia in Nigeria: dermatoglyphic analysis of 90 casesAfr J Biochem Res 2007 1(4):54-59. [Google Scholar]
[6]. Boroffice RA, Down’s syndrome in Nigeria: dermatoglyphic analysis of 50 casesNiger Med J 1978 8(6):571-76. [Google Scholar]
[7]. Seltzer MH, Plato CC, Fox KM, Dermatoglyphics in the identification of women either with or at risk for breast cancerAm J Med Genet 1990 37(4):482-88.10.1002/ajmg.13203704122260593 [Google Scholar] [CrossRef] [PubMed]
[8]. World Health Organization, Global status report, Substance abuse, Facts and Figures. http://www.who.int/substance_abuse/facts/global_burden/en/ [accessed on 30 august 2016] [Google Scholar]
[9]. Volkow ND, Koob GF, McLellan AT, Neurobiologic advances from the brain disease model of addictionN Engl J Med 2016 374(4):363-71.10.1056/NEJMra151148026816013 [Google Scholar] [CrossRef] [PubMed]
[10]. National Institute on Alcohol Abuse and Alcoholism, NIH Publication No. 13–7999 Reviewed July 2016, https://pubs.niaaa.nih.gov/publications/dsmfactsheet/dsmfact.pdf. [accessed on 30 august 2016] [Google Scholar]
[11]. American Psychiatric Association; Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Arlington, VA, American Psychiatric Association, 2013. Page no 571, Tobacco Use Disorder10.1176/appi.books.9780890425596 [Google Scholar] [CrossRef]
[12]. Government of India, Ministry of Health and Family Welfare. National Family Health Survey 4, 2015-16, State Fact Sheet, Karnataka, page4, Karnataka key indicators. http://rchiips.org/NFHS/pdf/NFHS4/KA_FactSheet.pdf (accessed on 30 august 2016) [Google Scholar]
[13]. Devčić S, Mihanović M, Miličić J, Glamuzina L, Comparative study on dermatoglyphics in alcoholic patientsColl Antropol 2009 33(4):1311-18. [Google Scholar]
[14]. Vijayaraghavan A, Aswath N, Qualitative and quantitative analysis of palmar dermatoglyphics among smokeless tobacco usersIndian J Dent Res 2015 26(5):48310.4103/0970-9290.17204226672417 [Google Scholar] [CrossRef] [PubMed]
[15]. National Institute of Alcohol Abuse and Alcoholism, National Institute of Health, US Department of Health and Human Services, Alcohol Alert, Alcohol and Tobacco, Number 71, January 2007, Genetic Factors, https://pubs.niaaa.nih.gov/publications/aa71/aa71.htm. [accessed on 30 august 2016] [Google Scholar]
[16]. Carmelli D, Swan GE, Robinette D, The relationship between quitting smoking and changes in drinking in World War II veteran twinsJ Subst Abuse 1993 5(2):103-16.10.1016/0899-3289(93)90055-G [Google Scholar] [CrossRef]
[17]. Enoch MA, Goldman D, The genetics of alcoholism and alcohol abuseCurr Psychiatry Rep 2001 3(2):144-51.10.1007/s11920-001-0012-3 [Google Scholar] [CrossRef]
[18]. Swan GE, Carmelli D, Cardon LR, Heavy consumption of cigarettes, alcohol and coffee in male twinsJ Stud Alcohol 1997 58(2):182-90.10.15288/jsa.1997.58.1829065896 [Google Scholar] [CrossRef] [PubMed]
[19]. Grucza RA, Bierut LJ, Co-occurring risk factors for alcohol dependence and habitual smoking: update on findings from the collaborative study on the genetics of alcoholismAlcohol Res Health 2006 29(3):172-79. [Google Scholar]
[20]. Davis TJ, de Fiebre CM, Alcohol’s actions on neuronal nicotinic acetylcholine receptorsAlcohol Res Health 2006 29(3):179-85. [Google Scholar]
[21]. Howard LA, Ahluwalia JS, Lin SK, Sellers EM, Tyndale RF, CYP2E1*1D regulatory polymorphism: association with alcohol and nicotine dependencePharmacogenetics 2003 13(6):321-28.10.1097/00008571-200306000-0000312777962 [Google Scholar] [CrossRef] [PubMed]
[22]. True WR, Xian H, Scherrer JF, Madden PA, Bucholz KK, Heath AC, Common genetic vulnerability for nicotine and alcohol dependence in menArch Gen Psychiatry 1999 56(7):655-61.10.1001/archpsyc.56.7.65510401514 [Google Scholar] [CrossRef] [PubMed]