Neck pain has been defined by the Bone and Joint Decade 2000-2010 Task Force on neck pain and Its Associated Disorders, as an unpleasant subjective experience [1]. The prevalence of neck pain was estimated at 4.9% globally and has been associated with functional limitations [2]. Potential goals of therapeutic interventions include pain alleviation, reduction in disability, improvements in function and health related quality of life. Nonspecific neck pain often resolves; however, there is a 10% chance that the neck pain will reoccur and persist, which would in turn lead to further disability [3,4].
Emerging evidence from the published literature suggests that patient characteristics and psychosocial factors can predict or explain pain and disability [5,6]. Clinicians have different approaches to identify sources or modifiers of neck pain and to develop a treatment plan [7]. Short-term training of deep and superficial neck muscles has been shown to reduce self-reported pain and disability levels [8]. Previous studies have shown that anxiety and depression are correlated with self-reported disability and pain intensity in patients with chronic neck pain. Identifying predictors can also help clinicians to provide a more accurate prognosis or target specific types of interventions [7,9]. Therefore, the objective of the present study was to determine the contribution of psychological and health factors for patients with chronic neck pain and neck disability.
Materials and Methods
Participants and Study Procedures
The Ethical Approval for this cross-sectional study was secured through the Scientific Committee of the Department of Physiotherapy of the Technological Educational Institute of Western Greece. We invited patients who ranged from 18-65 years of age, and with idiopathic nontraumatic chronic neck pain to take part in this cross-sectional study conducted in Patras, Greece. To recruit patients, notifications were sent and advertisements were also posted in local rehabilitation centers hospitals and social meeting places across the greater area Achaia, Greece. Patients were eligible to take part in the present study who were presented with:
i) Neck pain for at least three months,
ii) A score of at least 5/50 on the (NDI), Greek version.
Patients were excluded from the present study if:
i) Had a history of previous neck surgery or cervical radiculopathy or myopathy,
ii) Had systemic diseases or pathological conditions of the central nervous system,
iii) Were pregnant,
iv) Had participated in any form of physiotherapy training program in the last six months.
Patients provided signed consents, complete an assessment form which included personal information, a brief medical history, and demographic features. Lastly, patients were required to complete four patient-reported outcomes including the NPRS, NDI, SF-12 and HADS. Participants were requested to complete three different NPRS scales by describing their “current” pain intensity, the “worst” pain and the pain at their “best”.
Patient Reported Outcomes
The NPRS is an 11-point scale that measures pain from 0 (no pain) to 10 (worst imaginable pain) based on patients ratings. The measurement properties of NPRS has shown documented and reported in the literature as a reliable and responsive tool in patients with neck pain [10]. More specifically, test-retest reliability Intraclass Correlation Coefficient (ICC)=0.76; 95% CI, 0.51-0.87 and the area under the curve was 0.85 (95% CI, 0.78-0.93).
The NDI is a commonly used patient reported outcome measure that is intended for people with neck pain [11]. It includes ten items: pain intensity, personal care, lifting, work, headaches, concentration, sleeping, driving, reading, and recreation, with each question measured on a six-point scale with 0 (no disability) to 5 (full disability) [11]. The numeric responses from all the ten items are added for an NDI score which can range from 0-50, with higher scores representing higher disability. The study by Trouli MN et al., demonstrated that the Greek version of NDI is a reliable, valid tool [12]. Cronbach alpha was found 0.85, test-retest ICC=0.93 (95% CI 0.84-0.97) and Standard Error of Measurement (SEM) and Minimum Detectable Change (MDC) were calculated as 0.64 and 1.78 respectively [12].
The SF-12 is a 12-item health status questionnaire which provides a shorter alternative to SF-36 [13]. It includes two summary score components: physical and mental health. The physical health represents the physical functioning, role, bodily pain and general health subscales, whereas the mental health includes the vitality, social functioning, role-emotional and mental health subscales [13]. It is scored on a scale of 0-100, with higher scores indicating better health. The psychometric properties of the Greek version of SF-12 have been established and proved to be valid [14]. Concurrent (criterion) validity was supported by effect size differences between SF-36 and SF-12 overall scores which were found small (<0.2).
The HADS was originally developed by Zigmond AS and Snaith RP [15]. It is used to measure the patient’s anxiety and depression symptoms. The HADS is a 14-item questionnaire with seven question pertaining to anxiety and the remaining seven to depression [15]. Each question is scored on a 4-point scale. The numeric responses for anxiety and depression components are added separately, and scores 0-7 represent “normal”, 8-10 “borderline abnormal”, and 11-21 “abnormal” for each component. The Greek version of the HADS has been shown to be reliable and valid [16]. Cronbach’s alpha coefficient was 0.88 (0.82 for anxiety and 0.84 for depression) and test-retest ICC=0.94. The Greek HADS demonstrated high concurrent validity with the Beck Depression Inventory (BDI) and the State-Trait Anxiety Inventory (STAI) were found high (0.72-0.74).
Statistical Analysis
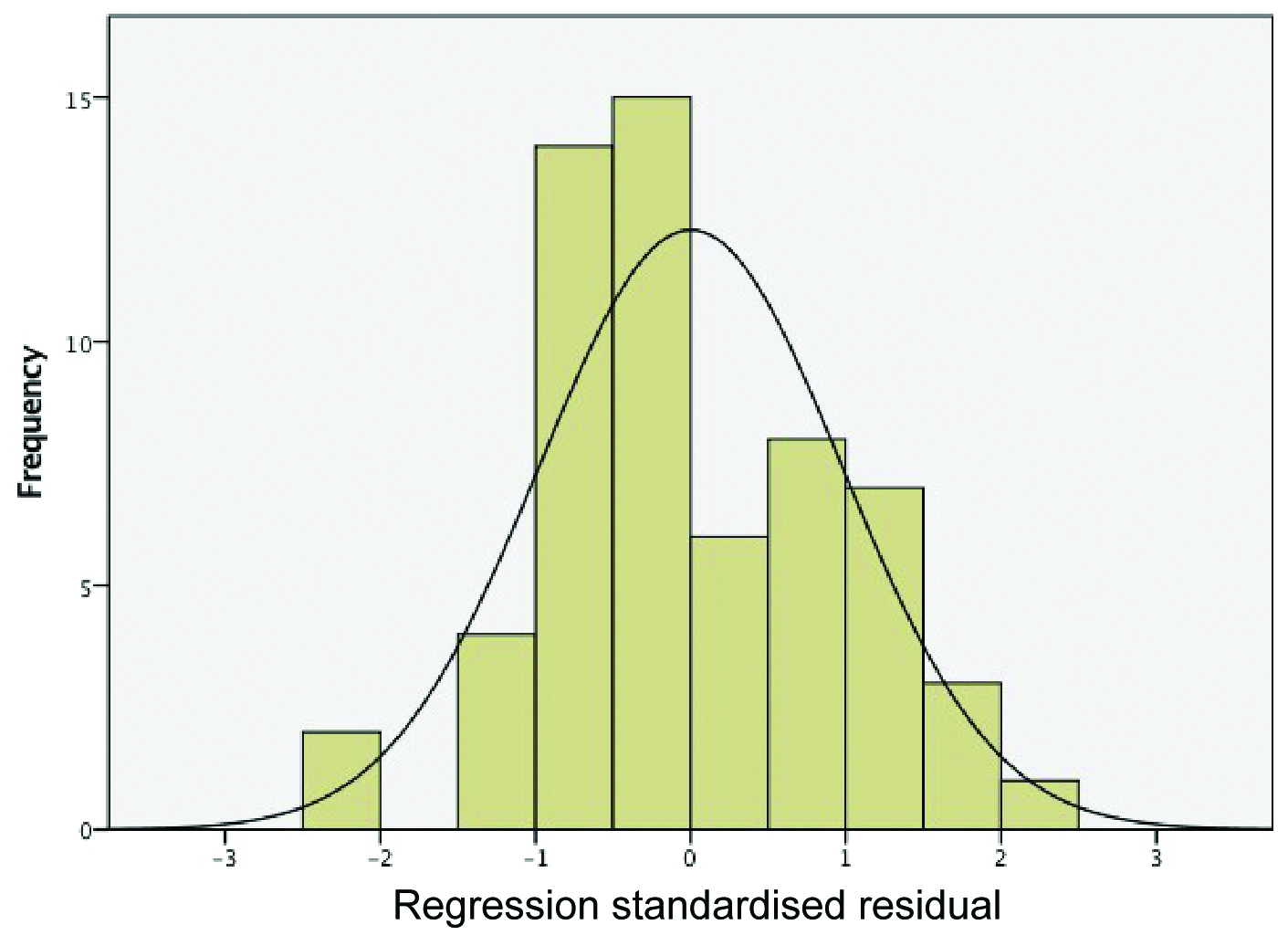
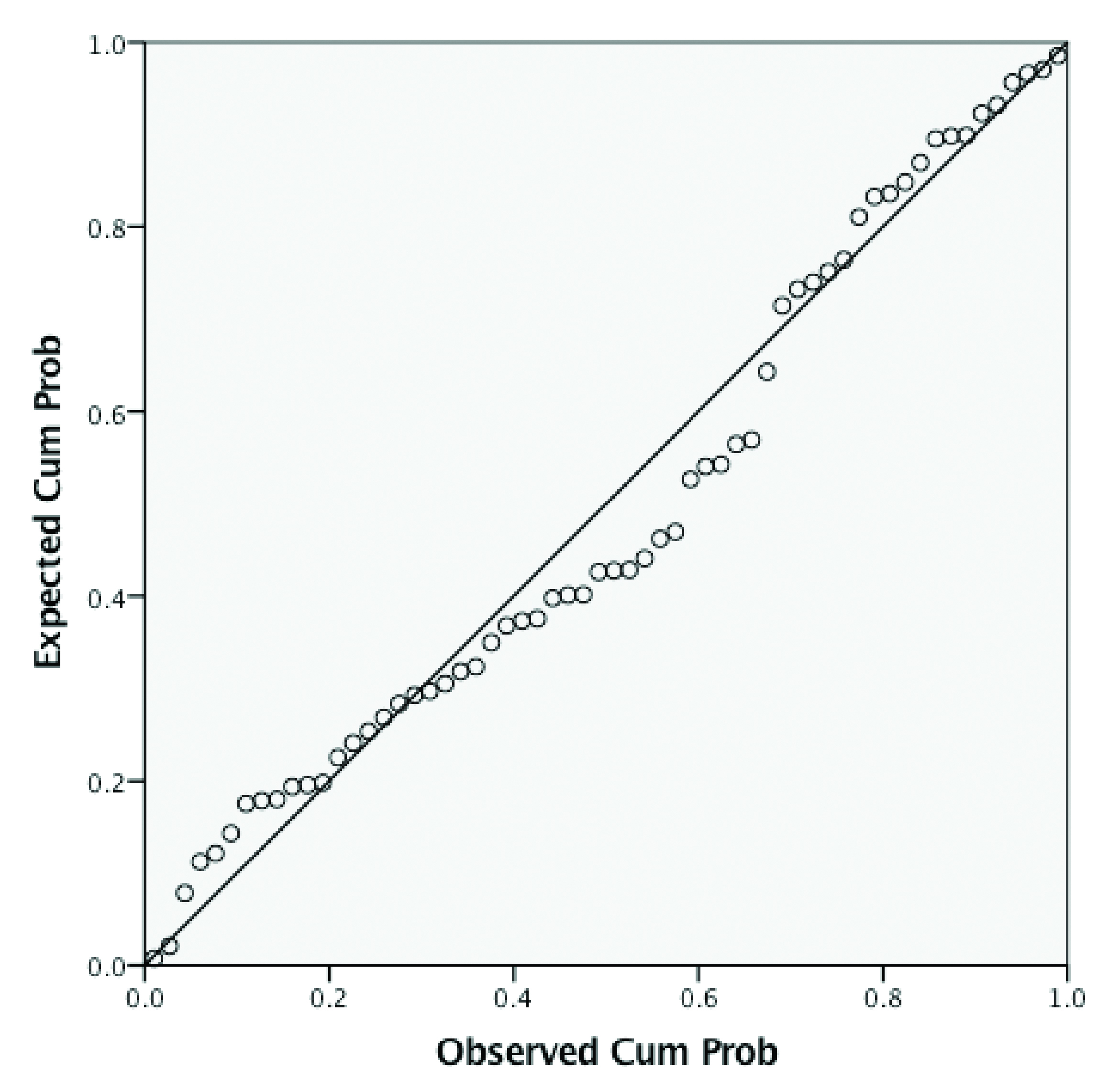
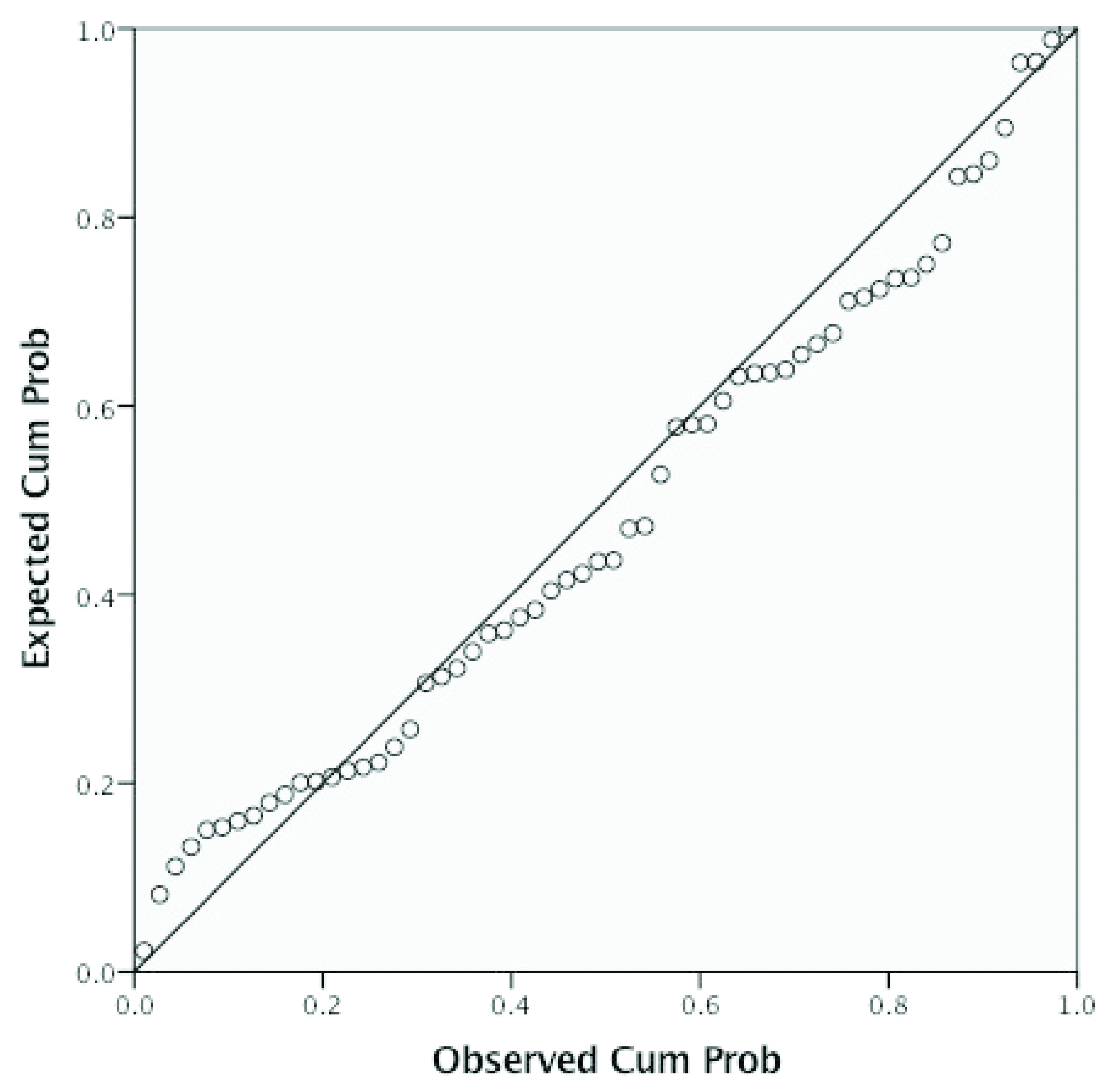
Descriptive statistics were calculated. We conducted the tests of normality, heteroscedasticity, multicollinearity, and linearity to make sure that all the assumptions of multiple regression were met prior to our analysis. Histograms and Q-Q plots were utilised for normality tests and are presented in [Table/Fig-1,2,3 and 4]. Two separate multiple regression analysis were performed with the “Enter” method to determine what levels of anxiety, depression, health status could contribute to pain and disability levels. The pain variable was a pooled of all numeric rating of pain scales (at “worst”, at “best” and “current” pain); disability was represented by the NDI. The independent variables that entered in each model were: the SF-12 physical and mental components, HADS anxiety and depression scores. We did not include into the regression model the total HADS score because it was highly correlated with anxiety and depression subscales and therefore, it was excluded as a redundant variable. A post hoc statistical power analysis was performed using 60 patients, with a total of three predictors, and we set the minimum observed R-squared value at 0.25. We performed our analysis using IBM SPSS Statistics software version 22.0 and a significance level of p-value ≤0.05 was considered statistically significant.
Normality test-histogram of neck disability levels.
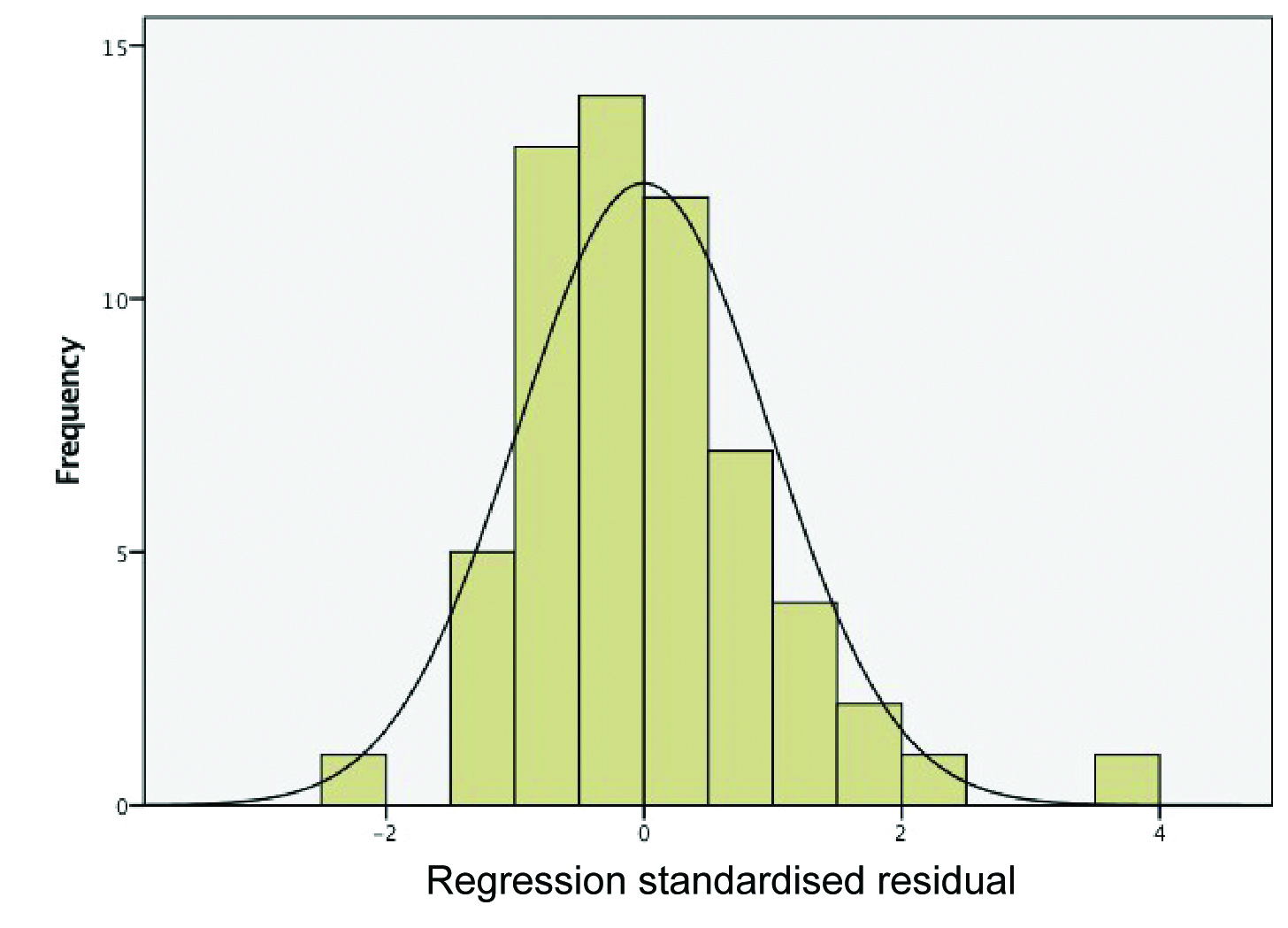
Normality test-histogram of pain intensity levels.
P-P plot of regression standardised residuals of pain intensity levels view.
P-P Plot of regression standardised residuals of neck disability levels.
Results
Sixty patients (13 males and 47 females, 39.45±12.67 years) completed the present study. The prevalence of symptoms was more than 12 months for 80% of the sample size. Forty-three patients (72%) reported that their symptoms started gradually. Almost 90% of the participants had higher education training (university degree) and most them (70%) reported that were living in suburban areas [Table/Fig-5]. The pain scores indicated a mean±SD moderate pain level of 3.91±1.76, and a low mean level of disability NDI=13.26±6.54 which indicates mild disability [17]. The sample’s demographic information is summarised in [Table/Fig-5]. Health status was determined by using the SF-12, with mean±SD baseline scores of 46.46±8.11 and 45.95±10.03 for the physical and mental components respectively. The values from the SF-12 indicated lower scores on the physical and mental component from the normal values. Generally, the average mean SF-12 for the age between 35 to 44 years old has been reported 52.1 for the Physical Component of SF-12 (PCS) and 51.8 for the Mental Component of SF-12 (MCS) [18]. The HADS was used to determine patients levels of depression and anxiety, with mean±SD scores of 5.05±3.65 and 7.20±4.47 respectively. The HADS values suggest that the recorded levels of depression and anxiety are within the normal to borderline abnormal levels. Our results yielded a statistical power of 0.96.
Demographic characteristics of the patients with chronic neck pain.
| Demographics | Mean±SD |
|---|
| Numeric Pain Rating Scale (NPRS) | 3.911.76 |
| Neck Disability Index (NDI) | 13.26±6.54 |
| Anxiety (HADS) | 7.20±4.47 |
| Depression (HADS) | 5.05±3.65 |
| HADS Total | 12.25±7.21 |
| PCS (SF-12) | 46.46±8.11 |
| MCS (SF12) | 45.95±10.03 |
| Age (years) | 39.45±12.67 |
| Sex | n (%) |
| Female | 47 (80) |
| Male | 13 (20) |
| Residency |
| Urban | 14 (23) |
| Suburban | 42 (70) |
| Rural | 4 (7) |
| Education |
| Lower education | 2 (3) |
| Secondary education | 5 (8) |
| Higher education | 53 (89) |
| Onset of Symptoms |
| Sudden | 17 (28) |
| Gradually | 43 (72) |
| Duration of Symptoms |
| Three months | 3 (5) |
| Six months | 9 (15) |
| 12 months | 19 (32) |
| 24 months | 16 (27) |
| 48 months | 13 (21) |
PCS-Physical component of SF-12
MCS-Mental component of SF-12
HADS-Hospital anxiety and depression scale
Multiple Regression Analysis
For pain levels, the SF-12 physical component score was found to be the statistically significant independent variable in our first regression model. Together SF-12 and the HADS scores accounted for 40% of the variance in patients with chronic neck pain [Table/Fig-6]. For each one point increase in pain, the physical component of SF-12 will be reduced by 0.30 units. For disability levels, patients anxiety, SF-12 physical component score, and anxiety were shown to be the statistically significant independent variables in our second model. The SF-12 subscale components and the HADS subscales scores explained 50.00 % of the variance in patients disability levels [Table/Fig-7]. For each one point increase in neck disability index anxiety scores will be increased by 0.27 units while the physical components of SF-12 will be reduced by 0.35 units.
Predictors of pain intensity levels.
| Model | R2 | Unstandardised Coefficients | Standardised Coefficients | t | p-value |
|---|
| B | Standard Error | Beta |
|---|
| (Constant) | | 9.02 | 2.67 | | 3.37 | 0.001 |
| Anxiety (HADS) | 0.13 | 0.06 | 0.28 | 1.96 | 0.054 |
| Depression (HADS) | 0.05 | 0.08 | 0.09 | 0.67 | 0.504 |
| PCS-SF12 | -0.07 | 0.03 | -0.30 | -2.50 | 0.015 |
| MCS-SF12 | 0.398 | -0.03 | 0.02 | -0.15 | -1.08 | 0.281 |
PCS: Physical Component of SF-12
MCS: Mental Component of SF-12
HADS: Health Anxiety and Depression Scale
Predictors of disability levels.
| Model | R2 | Unstandardised Coefficients | Standardised Coefficients | t | p-value |
|---|
| B | Standard Error | Beta |
|---|
| (Constant) | | 22.29 | 7.58 | | 2.93 | 0.005 |
| Anxiety (HADS) | | 0.40 | 0.19 | 0.27 | 2.09 | 0.040 |
| Depression (HADS) | | 0.44 | 0.23 | 0.24 | 1.92 | 0.059 |
| PCS-SF12 | | -0.28 | 0.08 | -0.35 | -3.22 | 0.002 |
| MCS-SF12 | 0.501 | -0.01 | 0.08 | -0.03 | -0.23 | 0.817 |
PCS: Physical Component of SF-12
MCS: Mental Component of SF-12
HADS: Health Anxiety and Depression Scale
Discussion
The present study, showed that psychological factors such as anxiety and health status physical components may be the main contributors of chronic neck pain and disability. Generally, psychological predictors of chronic neck pain often reporting of both anxiety and depression [6]. Regarding, the measurements of depression levels were within the normal range (5.05±3.65) while anxiety was slightly higher but above the normal range and within the abnormal range (7.20±4.47). In the literature, it has been reported that individuals with chronic neck pain tend to have higher depression and anxiety levels [5]. The mean age of our sample was 39.45±12.67 years, which represents relatively young adults. This age group has been shown to report substantial psychological stress and this might be a potential explanation for the slightly increased anxiety levels [19]. The study results showed that even with depression levels within the normal range, anxiety and the physical components of health status may contribute to changes in pain and disability scales [Table/Fig-6,7].
Self-reported neck disability was measured with NDI and our multiple regression analysis showed that age, SF-12 physical component and the HADS scores, explained 50% of the variance in patients disability levels. A recent study from Elbinoune I et al., in 80 patients with symptomatic neck pain found that anxiety and depression were prevalent [20]. Talvari A et al., concluded that 200 elderly patients (<60 years old) with neck pain are associated with anxiety and depression [21]. Previous studies from Dimitriadis Z et al., and Young SB et al., showed that neck pain intensity and neck disability was significantly correlated with anxiety and neck disability [7,22]. Dimitriadis Z et al., reported a correlation of r value=0.32 between neck pain and anxiety and a correlation of r value=0.54 between anxiety and disability in a sample of 45 patients with idiopathic chronic neck pain [7]. Young SB et al., reported a correlation of r value=0.68 between disability NDI and psychological distress among a sample of n=61 (41 females and 20 males) with dominant neck pain [7]. In terms of anxiety levels as a significant contributor, these findings corresponded well with our results and confirm the available literature [23]. However, our analysis indicated that depression was not a significant contributor to pain and disability in the Greek population. This can be attributed to the different social life and different work environment in comparison with other countries. Also, the absence of a diagnostic test about chronic neck pain makes difficult to determine the prognostic factors.
The strengths of the present study were that we pooled three different categories of pain intensities and were investigated into relatively young adults (mean age 39.5 years old) of Greek population with idiopathic chronic neck pain. Also, we indicated the contribution of each prognostic factor and therefore, future clinical studies should aim to design preventative strategies to modify those psychological factors. More specifically, anxiety HADS subscale and the physical component of SF-12 were the main determinants of neck pain and disability. Further longitudinal studies with multiple follow ups are warranted.
Limitation
The present study has several limitations that need to be addressed. First, the proportion of females was large compared to males and therefore, we cannot generalise our results to chronic neck pain population. Second, we evaluated the determinants in only one evaluation time point and this design has limited value in terms of causation. Moreover, although the present study explained a large proportion of the variance, 50% of the pain and disability variable remained unexplained.
Conclusion
The self-reported anxiety of HADS and the physical health status of SF-12 were the two significant contributors of pain and disability levels for patients with chronic neck pain. Future studies should aim to conduct preventative interventions for people with idiopathic chronic neck pain with control groups and longer follow ups by taking into consideration the lifestyle, working conditions and family demands. More specifically, should test whether change in anxiety and depression are associated with change in neck disability and work role participation. Psychological factors and health status must always be considered in clinical practice for the assessment and the management of chronic neck pain and disability.
PCS-Physical component of SF-12
MCS-Mental component of SF-12
HADS-Hospital anxiety and depression scale