Dental caries is an infectious microbial disease of the calcified tissues of the teeth that results in localised dissolution and destruction of the organic substance. It is most prevalent worldwide and is the most common cause of tooth loss in any geographic location [1]. The prevalence of dental caries has been linked to the socioeconomic and demographic conditions of the population. Though, universally found, it tends to go untreated in underserved communities in both developing and industrialised countries [2].
There has been changing trends in the management of carious lesions. Conventional restorative approaches that involve the complete removal of carious tooth tissue followed by placement of an ideal restoration has been substituted by more biological and less invasive methods focussing on biofilm control and disruption of the cariogenic biofilm environment to arrest caries. The HT fits this philosophy which seals the cariogenic biofilm under the crown. An alternative biological treatment approach is ART which can provide curative care with minimised equipment. The essential aspects in the management of caries including both preventive strategy as well as the restorative step is fulfilled by ART and HT [3].
The ART is a noninvasive and viable approach that can be effective to control decay in a socioeconomically deprived community. This approach was originally introduced for economically less developed population. However, it has applications in introducing oral care to children, not previously exposed to dentistry and for patients with extreme fear and anxiety. ART is an alternative treatment for dental caries that involves removal of caries from those cavities that are accessible to hand instruments. As ART is painless, the need for anaesthesia is eliminated. Cavity is restored with an adhesive material like Glass Ionomer Cement (GIC) that bonds to the tooth structure and releases fluoride [2].
The HT is a minimally invasive restorative procedure using Preformed Metal Crown (PMC) cemented with no local anaesthesia, no caries removal and no tooth preparation. Carious primary molars have shown favourable outcomes following restoration with Hall PMC in terms of pulpal health and restoration longevity as compared to conventional restorations. PMCs are now being recommended as the optimum restoration by the British Society of Paediatric Dentistry for managing primary molar teeth where caries involve two or more surfaces or where teeth are badly broken down [4].
However, there are some concerns about this technique. The first is the time taken for each restoration. A second concern relates to how it involves no occlusal reduction before fitting the crown as this may be associated with premature contact causing an increase in the OVD. In order to address the dental care needs of the paediatric population in a better way, clinicians must continue to explore alternative strategies for caries management and restorative treatment. Since, pain has a direct influence on child’s behaviour, the discomfort reported during treatment will facilitate further assessment and procedural modification if needed. Simpler and more acceptable caries management strategies for primary teeth can enhance dental care among children in diverse settings. Hence, the present study was designed to compare the acceptability of ART vs. HT for treating occlusoproximal lesions among children residing in rural communities. This study compares the acceptance of treatments in terms of child reported discomfort, preference of either procedure in terms of aesthetics, assessing the OVD changes following restoration and time taken for each restorative procedure.
Materials and Methods
This randomised clinical study was carried out over a period of three months (June to August 2016) by recruiting participant children from a primary school located in rural area of West Godavari district, Andhra Pradesh. A total of 30 children in the age group of five to eight years with at least one occlusoproximal carious primary molar were randomly selected. Written consent was obtained from the parents/guardians for participation in the study. The study protocol was also approved by the Institutional Ethical Board.
The sample size was calculated based on the level of precision at ±5, the level of confidence at 95% and the desired level of confidence interval was taken as 95%. Hence, level of significance was considered to be 5% or 0.05.
The participant children were randomly allocated to either Group A (ART) or Group B (HT) for undergoing restorative treatment. The criteria for selection included children with good general health and presenting at least one occlusoproximal lesion in primary molars with caries extending to dentine and no obvious pulp exposure clinically. Lesions preferably accessible to hand instruments for ART were selected. Children with history of pain, presence of fistula or abscess near the selected tooth, any pulpal exposure or teeth exhibiting pathological mobility were excluded from the study.
The selected children were assigned by random allocation to have their tooth treated with ART or the HT. The randomisation was carried out using a chit-pull method. In cases where the child had more than one occlusoproximal cavity eligible for inclusion, only one cavity was selected for the study.
The children assigned for treatment using ART (Group A) had their cavities prepared and restored following the ART approach proposed by Frencken JE et al., [5] [Table/Fig-1]. The tooth to be treated was isolated using cotton wool rolls alongside and plaque removal was done using wet cotton pellets. Then the tooth surface was dried with dry cotton pellets and a dental hatchet was used to make the cavity entrance wider. Residual carious dentine was removed using excavator and the unsupported thin enamel was fractured off with the hatchet. Any soft caries near the pulp was removed carefully and cavity cleaned with wet cotton pellets. Then the cavity was dried using dry cotton pellets and a precurved matrix strip was placed between the teeth. A wedge was inserted to support the strip under the contact point.
Procedure for ART technique: a) armamentarium; b) checking for occlusal vertical dimension before treatment; c) isolation of tooth; d) caries excavation; e) restoration with GIC; f) checking for occluso vertical dimension post treatment.
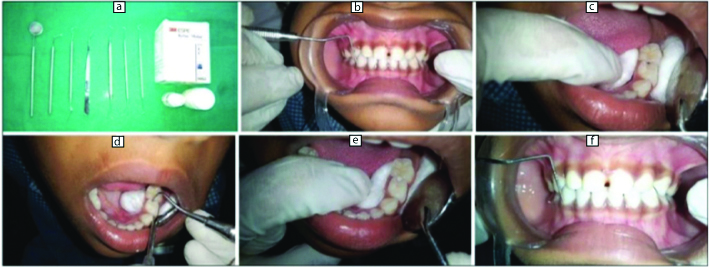
The cavity and adjacent fissures were then conditioned using a moist cotton pellet dipped in GC cavity conditioner liquid for 10-15 seconds. Finally, the cavity was washed with three sequences of wet cotton pellets and dried with three sequences of dry cotton pellets. After ensuring the tooth to be dry, cavity was restored with Fuji IX, GC glass ionomer restorative material.
The treatment of selected teeth for HT (Group B) was carried out according to the HT protocol of Innes NP et al., [Table/Fig-2]. No local anaesthesia was used as it was not required (no dentine was removed) and as per standard HT [6]. As per the protocol, orthodontic separators were placed during the first visit. This was done after assesing the tooth shape, contact points/areas and the occlusion. The use of orthodontic separators creates space for fitting a Hall crown. In order to protect the airway, the child must be sitting upright. Two lengths of dental floss were threaded through the separator. Then the separator was stretched and floss taught through the contact point briskly and firmly until the leading edge is only felt “popping through” the contact point. The floss is then removed and the patient was recalled after three to five days for the second appointment.
Procedure for Hall technique: a) checking for occlusal vertical dimension before treatment; b) separators placed; c) isolation of tooth; d) trial seating of stainless steel crown; e) post cementation of crown; f) checking for occlusal vertical dimension post treatment.
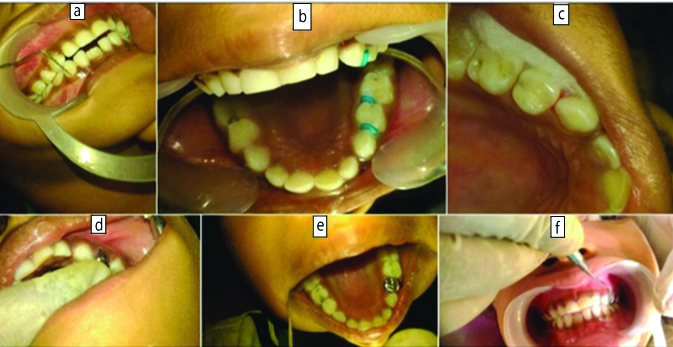
In the second visit, the separator was removed with an excavator. Any loose plaque and food debris was gently removed from the cavity. The child’s occlusion was assessed by measuring OVD with a millimeter probe using the distance between the most coronal points of the primary canines. This was done in order to assess the degree of overbite after mounting of the crown. The airway was protected by placing a gauze swab square between the tongue and the tooth to be crowned. The correct crown size was selected with the aim to fit the smallest size of crown which will seat so that it covers all the cusps and approaches the contact points, with a slight feeling of “spring back.”
The treatment area was kept free from saliva by isolating the tooth with cotton wool rolls. Then, the inside of the crown was dried with dry cotton pellets. The GIC Fuji I was mixed for 10 seconds, according to the manufacturer’s instructions and the crown was generously loaded with GIC (at least two-thirds full). Then the crown was placed over the tooth and seated by finger pressure or by asking the child to bite it into place. Then the crown position was checked, soon after it was fitted. Any excess GIC was wiped away with a cotton wool roll or the gauze swab used to protect the airway. A cotton wool roll was placed between the crown and the opposing tooth and the child was asked to bite firmly on the crown for another two to three minutes. The excess cement was removed by flossing between the contacts.
The buccal relationship of the crowned tooth with its opposing number was noted and if any displacing contact seen, resulting in a cross bite, then removal of entire crown was considered.
Children who underwent treatment were asked to evaluate their experience by completing the patient satisfaction form. Child reported discomfort was assessed using Wong-Baker Faces pain scale during and after treatment. The appearance of restoration was recorded if positive or negative as perceived by the patient. The general opinion regarding the technique was also noted whether the child was satisfied and would recommend the procedure or was not satisfied. To evaluate the perceptions and concerns related to the procedure per se, the parameters recorded included the OVD changes before and after treatment and overall time taken for the procedure. The assessment of OVD was performed according to a modified version of van der Zee V and van Amerongen WE [7]. The procedures were timed using a stopwatch started when the child has his/her mouth open and the operator is about to start the restorative treatment and stopped when the treatment is completed.
Statistical Analysis
The data obtained from all observations were entered into a data base and analysed using SPSS 11.5. OVD scores for both groups were compared using paired t-test. Chi-square with Yate’s correction and Mann-Whitney U test were used to investigate the primary outcome. Paired and independent t-tests were used to evaluate the dependent variables.
Results
There was a statistically significant difference with respect to aesthetic appearance. The results showed that patient reported aesthetical acceptability was maximal among the ART group compared to HT group [Table/Fig-3].
Comparison of two groups with respect to aesthetic appearance
| Appearance | ART | Percentage (%) | HT | Percentage (%) | Total |
|---|
| Yes | 15 | 100.00 | 3 | 20.00 | 18 |
| No | 0 | 0.00 | 12 | 80.00 | 12 |
| Total | 15 | 100.00 | 15 | 100.00 | 30 |
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
There was no statistically significant difference with respect to acceptance of technique among the groups compared. Patient satisfaction with the treatment was same for both the techniques [Table/Fig-4].
Comparison of two groups with respect to acceptance of technique
| Opinion of Technique | ART | Percentage (%) | HT | Percentage (%) | Total |
|---|
| Satisfied | 13 | 86.67 | 10 | 66.67 | 23 |
| Not Satisfied | 2 | 13.33 | 5 | 33.33 | 7 |
| Total | 15 | 100.00 | 15 | 100.00 | 30 |
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
The intergroup comparison showed a statistically significant difference with respect to pain. Child reported discomfort for ART was significantly high compared to the HT procedure [Table/Fig-5].
Comparison of facial pain scores among two groups during and after treatment.
| Groups | Treatment | Mean | Std.Dv. | Mean Diff. | SD Diff. | % of change | z-value | p-value |
|---|
| ART | During | 1.87 | 0.92 | | | | | |
| After | 0.00 | 0.00 | 1.87 | 0.92 | 100.00 | 3.1798 | 0.0015* |
| HT | During | 0.53 | 0.92 | | | | | |
| After | 0.00 | 0.00 | 0.53 | 0.92 | 100.00 | 1.8257 | 0.0679 |
*p ≤ 0.05 Significant
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
There was a statistically significant difference with respect to the recorded OVD. HT showed an increase in OVD following treatment, whereas the scores remained unchanged before and after treatment in the ART group [Table/Fig-6].
Comparison of occlusion vertical dimension scores in two study groups.
| Groups | Treatment | Mean | Std.Dv. | Mean Diff. | SD Diff. | % of change | Paired t | p-value |
|---|
| ART | Before | 9.33 | 1.91 | | | | | |
| After | 9.33 | 1.91 | 0.00 | -- | 0.00 | -- | -- |
| HT | Before | 9.63 | 1.54 | | | | | |
| After | 10.27 | 1.78 | -0.63 | 0.61 | -6.57 | -4.0119 | 0.0013* |
*p ≤ 0.05 Significant
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
The intergroup comparison showed a statistically significant difference with respect to time. HT took a longer time for the procedure compared to ART [Table/Fig-7].
Comparison of two groups with respect to time taken for procedure (seconds).
| Groups | mean | (±)SD | SE | t-value | p-value |
|---|
| ART | 624.00 | 196.13 | 50.64 | -5.9748 | 0.0001* |
| HT | 1052.00 | 196.22 | 50.66 | | |
*Independent t-test p<0.05
Atraumatic Restorative Treatment (ART), Hall Technique (HT), Standard Error (SE)
Discussion
A low utilisation of dental services among the rural dwellers dictates the need for outreach programmes aimed at providing dental care for rural population. This study was aimed to investigate the acquiescence of minimally invasive treatments like ART and HT among children when applied in a low technology setting.
The child’s age is an important factor as dental caries in young children has a unique pattern and poses new challenges. Primary teeth have thinner enamel and dentin and broader proximal contacts than permanent teeth leading to increased caries susceptibility and more rapid progression of caries to the pulp [8]. Hence, cavitated proximal lesions need restorative therapy to limit progression. Thus, treatment of occlusoproximal cavitations employing HT or ART was the main focus in the present research. The factors taken into consideration included child self-reported discomfort associated with treatment, OVD changes, general acceptance of the technique as well as acceptance related to dental appearance and the operator concern including the time factor.
Atraumatic restorative treatment involves the use of manual instruments to prepare cavities followed by placement of a high-viscosity GIC and this strategy for the management of caries has been tested in many settings with good outcomes for single surfaces [2]. Through complete tooth coverage, PMC offer protection to teeth and even caries progression would be arrested. A less invasive method is the use of HT where crowns are pushed over teeth without tooth preparation or caries removal [3].
One of the primary outcome of evaluation in the present comparative study was the assessment of discomfort which was done using the Wong-Baker FACES pain rating scale. It is an ordinal six point scale ranging from zero to five where score of zero shows a smiling face indicating no discomfort, whereas a score of five shows a crying and sad face indicating great discomfort [9]. The assessment was done during and after the treatments as well. Most of the children experienced pain during excavation and the reported discomfort was found to be high for ART. HT was rated to cause minimal discomfort and was highly acceptable to children. Around 80% reported pain with ART in contrast to only 20% with the HT. Since, there is no tooth preparation or caries removal involved in the procedure, HT tends to be more acceptable. Though, pain was reported when ART technique was used it was significantly less than the conventional restorative technique as observed by Rahimtoola S et al., in their comparative study [10]. The atraumatic perspectives of ART have been reported by Schriks MC and van Amerongen WE who stated that children treated with ART approach experienced less discomfort as compared to one treated with rotary instruments [11]. HT was assessed by general dental practitioners as causing significantly less discomfort compared with conventional restorative techniques [12].
Assessment of OVD was performed according to a modified version of van der Zee V and van Amerongen WE [7]. The OVD measurement in the present study was evaluated during and after the treatments. An increase in OVD was recorded for HT following treatment. Since, the technique involves no occlusal reduction before fitting the crown, it may be associated with a premature contact and subsequent increase in the OVD.
Hall technique was inevitably associated with a premature contact following cementation as reported by Innes NP et al., OVD for first primary molars was 2.3 mm and for second primary molars the value was a little higher that is 2.5 mm. Concerns about the increase in the OVD (i.e., opening up the bite) following placement of HT crowns have been alleviated [6]. However, the re-establishment of occlusion by itself within 15 to 30 days following placement of crown using HT has been reported. Follow up time varied from 15 days to one year [12].
Hall technique manipulates the plaque’s environment by sealing it into the tooth, separating it from the substrates it would normally receive from the host’s diet. Even though the plaque may continue to receive some nutrition from pulpal perfusion, caries may not progress if it is effectively sealed from the oral environment. By sealing in the caries, the actively cariogenic plaque biofilm is altered thus, isolating it from nutrients and arresting the caries process [8]. There is increasing evidence that caries can slow or even arrest if completely sealed. HT is an acceptable method of achieving that seal and managing carious primary molars [4].
In the present study, the patient reported aesthetical acceptability was found to be high for ART compared to HT. The unsightly metallic appearance of stainless steel crowns seemed to be less acceptable for children. However, comparison of ART and HT with respect to treatment satisfaction was same for both the techniques. Neither ART nor HT require local anaesthesia and hence can be easily preferred over conventional restorative methods.
Another concern pertaining to these two minimally invasive treatments in the present investigation is the time factor. HT being a technique sensitive procedure took a longer time compared to ART. Apart from the restorative treatment, the HT requires placement of orthodontic separators three to five days prior to the second appointment, wherein actual procedure is carried out.
Though, ART is considered as the treatment modality for communities with no access to dentists, preformed crowns have higher survival rate than amalgam, composite resin, and glass ionomer restorations [13]. Also, Stainless Steel Crowns (SSCs) may be more acceptable to families of lower socioeconomic status [14].
As previously reported, the PMC placed using HT showed better outcomes in terms of pulpal health and restoration longevity as compared to conventional restorations [12]. Moreover, the clinical and radiographic success of SSCs used to restore carious lesions in primary molars placed using both the traditional technique and the HT showed similar success rate [15]. A more recent longitudinal clinical trial that evaluated the clinical efficacy of various caries management options for occlusoproximal cavitated lesions in primary molars concluded that the HT for placing SSCs was significantly more successful clinically than the Non-Restorative Caries Treatment (NRCT) with cavity opening and fluoride application and Conventional Restortions (CR) after one year [16]. Though, it is ten years since the first paper on the HT was published and almost 20 years since the technique first came to notice, it is well accepted that transfer of any new healthcare intervention from research study to clinical practice can take many years [17].
Limitation
Though, patient satisfaction was evident in ART as well as HT, the present study has yielded the preliminary findings and there are some limitations. Additional clinical trials incorporating a larger sample size and replicating different contexts and groups are recommended to evaluate the long-term treatment outcome. This would ensure an improvement upon the evidence laid down by the present study.
Conclusion
Among the two restorative options for occlusoproximal lesions in primary molars, the following conclusions were drawn from the study. The HT was found to be a preferred choice of restoration for the occlusoproximal lesions in children that can be done in a low technology setting. The ART can be recommended as an aesthetic alternative owing to its satisfactory OVD and minimal time requirement for the procedure.
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
*p ≤ 0.05 Significant
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
*p ≤ 0.05 Significant
Atraumatic Restorative Treatment (ART), Hall Technique (HT)
*Independent t-test p<0.05
Atraumatic Restorative Treatment (ART), Hall Technique (HT), Standard Error (SE)