Treating Odontomes : Surgical Management with Plasma Rich Fibrin as New Front Foot
Keerti Chandail1, Satyam Dutt2, Punit Singh3
1 Private Practitioner, Department of Paediatric and Preventive Dentistry, MDS, Jammu, Jammu and Kashmir, India.
2 Private Practitioner, Department of Paediatric and Preventive Dentistry, MDS, Jalandhar, India.
3 Private Practitioner, Department of Paediatric and Preventive Dentistry, MDS, Jalandhar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Keerti Chandail, Surakhsha Vihar, Paloura Top, Jammu-180015, Jammu and Kashmir, India.
E-mail: keerti4548@gmail.com
Denticles, Maxillary central incisor, Odontogenic
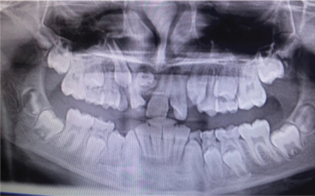
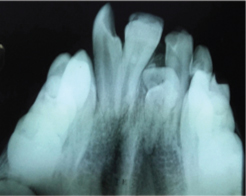
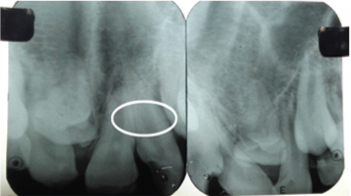
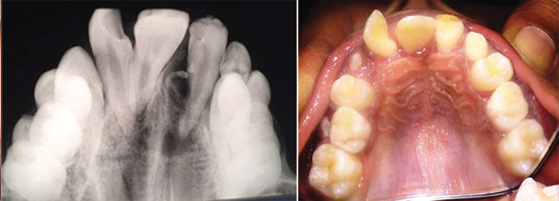
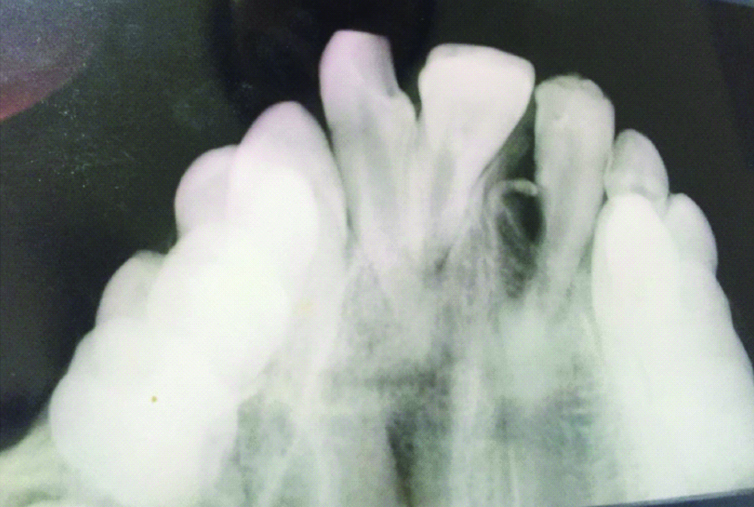
A 12-year-old child came to the Department of Paedodontics and Preventive Dentistry, Seema Dental College and Hospital, Rishikesh, Uttarakhand, India with the chief complaint of malaligned teeth in the upper front tooth region [Table/Fig-1]. On clinical examination, maxillary permanent right central incisor #11 was found to be missing. Various confirmatory radiological investigations were carried out i.e., Orthopantomogram (OPG), SLOB rule and occlusal radiograph. OPG revealed an impacted tooth-like structure in relation to #12 [Table/Fig-2] and maxillary occlusal radiograph revealed two radiopaque structures resembling a tooth near the root of the permanent lateral incisor i.e. #12. [Table/Fig-3] and SLOB rule [Table/Fig-4] confirmed the palatal location of these structures.
Malaligned teeth in upper front tooth region with missing central incisor #11.

OPG revealing impacted tooth i.r.t #12.
Occlusal radiograph showing two radiopaque structures resembling denticles near the root of permanent lateral incisor i.e., #12.
SLOB rule to confirm palatal location of denticles.
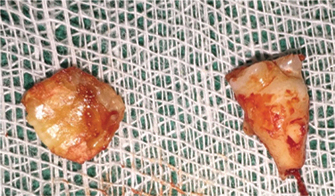
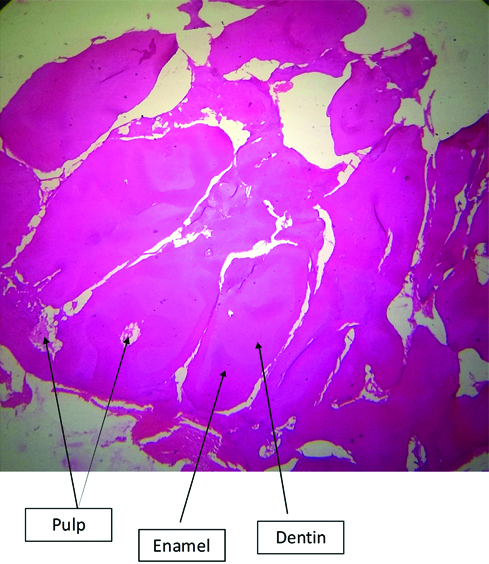
After confirming the diagnosis, surgery was planned out and routine blood investigations were carried out. Under aseptic conditions followed by the administration of lignocaine (1:80,000), crevicular incision was made on the palatal site from right first premolar to left first premolar [Table/Fig-5] and a full mucoperiosteal flap was elevated and bone drilling was done [Table/Fig-6]. Denticles were surgically removed and sent for histological investigations [Table/Fig-7]. Meanwhile, Plasma Rich Fibrin (PRF) was prepared using patient’s blood [Table/Fig-8] and was placed in the bony cavity for better results, [Table/Fig-9] followed by repositioning of flap and suturing. [Table/Fig-10] Uneventful healing was noticed after a follow up of three months [Table/Fig-11]. Formation of bone seen in the cavity after nine months [Table/Fig-12]. Histopathological slide contained well organised enamel, dentine and the pulpal space at the bottom under 40X magnification microscope and confirmed it to be compound odontome [Table/Fig-13].
Crevicular incision made on the palatal site from right first premolar to left first premolar.

Full mucoperiosteal flap elevated and bone drilled to expose.

Denticles removed after surgery.
PRF prepared from patient’s blood.

PRF placed in the bony cavity.
PRF- Plasma rich fibrin

Flap repositioned and sutured.

Follow up after three months.
Bone formation after follow up of nine months.
Histopathological slide exhibiting enamel and dentine along with pulpal space at the bottom under 40X Magnification.
Odontomas are the most common type of odontogenic benign jaws tumours. They are usually seen in patients younger than 20 years of age. These tumours are composed of enamel, dentin, pulp tissue and cementum [1]. According to the 2005 World Health Organization classification, two distinct types of odontomas are seen: complex and compound odontoma. In compound odontomas, dental tissues are arranged in numerous tooth-like structures known as denticles whereas in complex odontomas, all dental tissues are formed without an organized structure [1].
The etiology of odontomas is unknown, but it could be due to trauma during primary dentition, any inflammatory and infectious processes, hereditary anomalies, odontoblastic hyperactivity, or alteration of the genetic components which may be responsible for altered dental development. Slow growth and nonaggressive behavior are their characteristic features. Such lesions usually tend to be located between the roots of permanent erupted teeth or between the primary and permanent teeth. Most common locations included are anterior maxilla, followed by anterior mandible and posteroinferior regions [2].
Radiographically, odontomas appear as dense tooth like structures with prominent external margins surrounded by a thin radiolucent zone [3]. In the present case report, similar radiographic findings were noticed and the case was intitally diagnosed as denticles based on the radiographic findings which was later confirmed as compound odontome by histopathological investigation. The site was the anterior region of the maxilla, which, according to many researchers, is the most common location [3]. Hence, the location also confirmed the diagnosis of compound odontome in our case too.
The most preferred treatment for compound odontome is complete surgical removal along with associated soft tissues, if any. Recurrences do not occur usually [4]. That is why surgery was planned in the mentioned case with complete removal of the odontomes. Bony cavity was prepared for the removal of impacted denticles and for faster bone healing PRF was placed in it. According to Dohan DM et al., [5] PRF enhances the proliferation of various cell types, stimulates cellular differentiation and enhances the angiogenesis and also aids in bone regeneration. A follow up of nine months showed healthy bone formation.
Abnormal eruption or delayed eruption of teeth is a common finding nowadays, however, significant deviations from established norms should alert the clinician to further investigate the patient’s health and development. There is always a high association between odontomas and impacted teeth and to prevent the adverse effects of disturbances in tooth eruption, routine orthopantomogram should be carried out for early diagnosis and correct treatment planning. After confirming the diagnosis, odontome should be surgically extracted for normal eruption of all the permanent teeth.
[1]. Kramar IRH, Pindporg JJ, Shear M, Histological Typing of Odontogenic Tumours, World Health OrganizationInternational Histological Classification of Tumours 1992 2nd editionBerlin, GermanySpringer10.1007/978-3-662-02858-2_2 [Google Scholar] [CrossRef]
[2]. Helena S, Pedro M, Compound odontoma-Case reportRev Port Estomatol Med Dent Cir Maxilofac 2013 54:161-65. [Google Scholar]
[3]. Sreedharan S, Krishnan IS, Compound odontoma associated with impacted maxillary incisorsJ Indian Soc Pedod Prev Dent 2012 30:275-78.10.4103/0970-4388.10502523263436 [Google Scholar] [CrossRef] [PubMed]
[4]. Nelson BL, Thompson LDR, Compound odontomaHead Neck Pathol 2010 4(4):290-91.10.1007/s12105-010-0186-220533004 [Google Scholar] [CrossRef] [PubMed]
[5]. Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part I: Technological concepts and evolutionOral Surg Oral Med Oral Pathol Oral Radiol Endod 2006 101:e37-e44.10.1016/j.tripleo.2005.07.00816504849 [Google Scholar] [CrossRef] [PubMed]