Ankyloblepharon filiforme adnatum, Ankyloblepharon-ectodermal dysplasia-clefting syndrome, Hay-wells syndrome
A one-day-old male newborn was presented with the complaints of closed eyes since birth with no movements of eyelids. The baby was noted to have fused eyelids at birth [Table/Fig-1a,b]. The mother denied taking any drugs except iron and vitamin supplements. The antenatal, intranatal, and postnatal periods were uneventful. There was no history of any radiation exposure. The previous siblings, a five-year-old male and a three-year-old female were healthy. There was no family history of congenital anomalies or consanguinity. A detailed paediatric assessment revealed dystrophic thin, ridged nails [Table/Fig-1c] and cleft palate [Table/Fig-1d]. Eyelashes and scalp hair was sparse. Ophthalmic examination revealed that there were multiple, asymmetrical, broad and extensible adhesions present between the eyelids margins of the both eyes. These bands were clearly visible only after stretching the eyelids apart. The interpalpebral aperture was limited to less than 1 mm in both eyes. The case was diagnosed as Ankyloblepharon-Ectodermal Defects–Cleft lip/palate (AEC) syndrome. And all the bands of tissue were cut with blade (no. 15) following the anterior retraction with a muscle hook [Table/Fig-2a,b]. The procedure was accompanied by minimal oozing of blood from the lid margin and consequently shows separated eyelids with normal ocular structures [Table/Fig-2c]. Subsequent ocular examinations were normal including ocular motility, pupil reactions, anterior segment and fundus during follow up. The rest of the physical examination was unremarkable. Child was referred to Department of Paediatric surgery for the cleft palate repair.
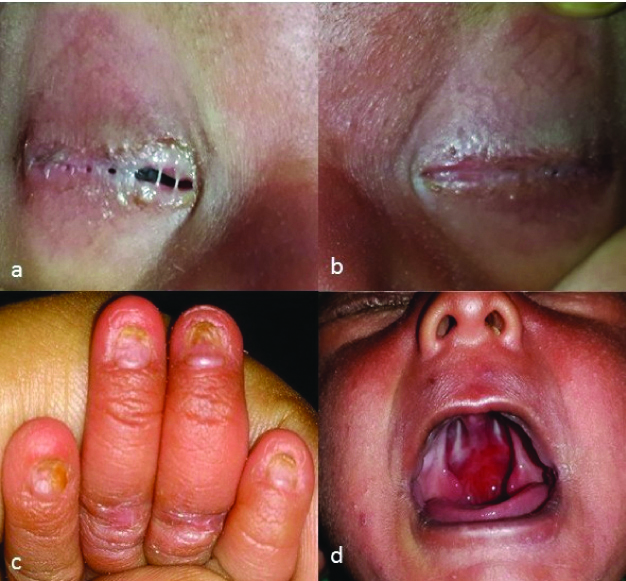
a,b) Photograph demonstrates multiple extensive thick and broad extensile bands of tissues connecting the eyelid margins of the right and left eye with sparse eyelashes and eyebrows; c) Photograph shows dystrophic thin, ridged fingernails with frayed distal edges; d) Bilateral AFA and cleft palate.
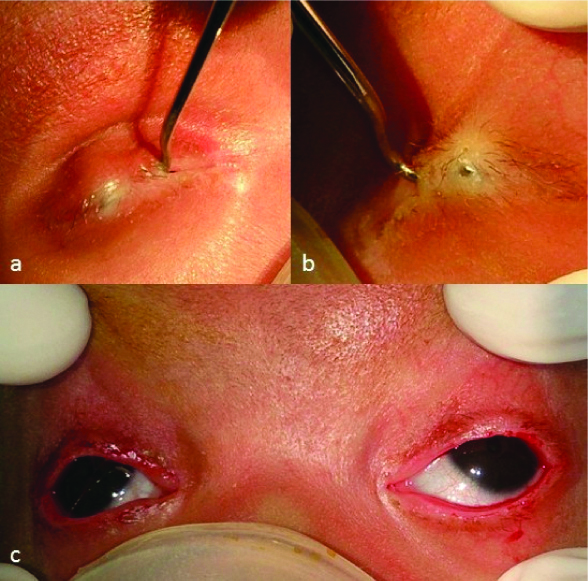
a,b) Photograph shows anteriorly retracted bands with strabismus muscle hook of the right and left eyelids; c) Demonstration of separated eyelids of both eyes following surgical procedure.
Ankyloblepharon Filiforme Adnatum (AFA) is a rare benign congenital abnormality. It refers to the eyelid disorder in which the upper and lower lids are joined by bands of tissue anywhere along the lids [1]. This entity was first described in 1881 by Von Hasner [1]. Further, Rosenman Y et al., have classified AFA into four subgroups (1-isolated, 2-associated with cardiac or central nervous system anomalies, 3-associated with ectodermal syndromes, 4-associated with cleft lip and/or palate) [2]. This entity may be present as an isolated finding or in association with other anomalies, or as part of a well-defined syndrome, particularly Hay-wells syndrome, also known as AEC syndrome [3,4]. It is a rare autosomal dominant disorder consists of ankyloblepharon, ectodermal dysplasia, and cleft lip and/or cleft palate, characterised by abnormal embryological development of ectodermally derived tissues such as skin, hair, teeth, nails, and exocrine glands [5]. The pathogenesis and aetiology of this entity is unknown and a number of theories have been proposed. Moreover, Hay RJ and Wells RS comment that AEC syndrome could be explained by a defective interaction of ectoderm and mesoderm, probably a fault in mesodermal tissues ability to organise ectoderm [3].
In conclusion, although AFA is a rare but it is a potentially amblyogenic congenital abnormality of the eyelids. Despite, the occurrence of other congenital anomalies or syndrome, treatment should be performed as early as possible to minimise any risk of amblyopia and enable complete examination of the eyes.
[1]. Von Hasner, Ankyloblepharon filiforme adnatumZ Kinderheilkd 1881 2:429 [Google Scholar]
[2]. Rosenman Y, Ronen S, Eidelman AI, Schimmel MS, Ankyloblepharon filiforme adnatum: congenital eyelid-band syndromesAm J Dis Child 1980 134(8):751-53.10.1001/archpedi.1980.021302000210087405912 [Google Scholar] [CrossRef] [PubMed]
[3]. Hay RJ, Wells RS, The syndrome of ankyloblepharon, ectodermal defects and cleft lip and palate: an autosomal dominant conditionBr J Dermatol 1976 94:277-89.10.1111/j.1365-2133.1976.tb04384.x946410 [Google Scholar] [CrossRef] [PubMed]
[4]. Guo S, Chen R, Xu Y, Mu Y, Chen L, Ankyloblepharon-Ectodermal Defects-Cleft Lip/Palate SyndromeJ Craniofac Surg 2017 28(4):e349-51.10.1097/SCS.000000000000360028230601 [Google Scholar] [CrossRef] [PubMed]
[5]. Bordin G, Valerio E, Cutrone M, Ankyloblepharon filiforme adnatum in a newbornAJP Rep 2015 5(1):e12-13. [Google Scholar]