Bilateral Isolated Nasal Cleft Management: A Facile Solution or a Treatment Conundrum?
Natarajan Chellappa1, Parit Ladani2, Hermann Sailer3
1 Observer, Department of Cleft and Craniofacial Surgery, Brahma Kumaris’ Global Hospital and Research Centre, Mumbai, Maharashtra, India.
2 Director, Department of Cleft and Craniofacial Surgery, Swiss Cleft and Craniofacial Center, Brahma Kumaris’ Global Hospital and Research Centre, Mumbai, Maharashtra, India.
3 Professor and Founder, Department of Cleft and Craniofacial Surgery, Cleft Children International Foundation, Zurich, Switzerland.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Natarajan Chellappa, 42 C, Kattabomman Street, Velandipalayam, Coimbatore-641006, Tamil Nadu, India.
E-mail: natarajan.balaji.c@gmail.com
Alar defects are usually secondary to trauma or nasal tumour excision. Congenital alar defects are rare of which isolated bilateral nasal clefts are extremely sparse. Reconstruction of these bilateral nasal clefts poses additional challenge due to lack of equivalent structural analogue on the opposite side to weigh against. Myriad of strategies are available for management of these clefts ranging from intelligible rotation flaps to more complex grafting procedures. Here we present a case report of bilateral isolated nasal cleft management in a 17-year-old male patient and the hurdles involved in achieving the desired results. It is important for an astute surgeon to provide an aesthetically appealing result on the most dominant structure defining the mid face.
Alar defects, Reconstruction, Rotation flaps
Case Report
A 17-year-old male patient was brought to our department by his father with complaint of unaesthetic appearance of his nose. A detailed perinatal history was recorded. There was no history of previous infection, trauma or surgery to the nose. Family history revealed no such deformity in the family members. On examination, a bilateral cleft in the middle third of the Lower Lateral Cartilage (LLC) was noted extending towards the lateral nasal bone on either side, measuring approximately 15×15 mm on both sides. Apart from the bilateral alar defect there was no bifiding of dorsum, tip, columella and septum and all were normal. A Computed Tomography (CT) of face was advised to rule out any latent deformities and was normal.
Assessing the cleft size it was decided to use the local tissues for reconstruction. A bilateral Z-plasty, with downward rotation and anterior advancement was planned. As patient’s physical and laboratory examinations were within normal limits he was admitted for surgical correction of the alar cleft under general anaesthesia. Surgical procedure performed in this patient is in accordance with the ethical standards of the institution and a written informed consent was obtained for the procedure. The incision on the left side alar cleft was designed as shown in the [Table/Fig-1]. The surgical principle of unequal-angled Z-plasty was implemented for the correction of the nasal cleft in our case [Table/Fig-2,3]. A full thickness chondrocutaneous lateral alar flap was raised keeping the incision in the crease between the LLC and Upper Lateral Cartilages (ULC). The flap was then rotated downwards and anteriorly till the medial edge of the flap reaches the anterior tip of the columella. The transpositional flap from the medial side was raised and rotated laterally to close the secondary defect due to downward rotation of the alar flap on the lateral side of the nose. The flaps were placed in position and closed in two layers, nasal mucosa and skin. Similar procedure was carried out on the right side alar cleft [Table/Fig-4]. Care was taken to achieve symmetry in form, shape and contour between the alar rims on both sides. Post-operative recovery was uneventful [Table/Fig-5] and patient was discharged on the third post-operative day. Patient was followed up after seven days and after one month and three months. The result achieved was satisfactory with good symmetry between both the alar rims and a well concealed scar [Table/Fig-6].
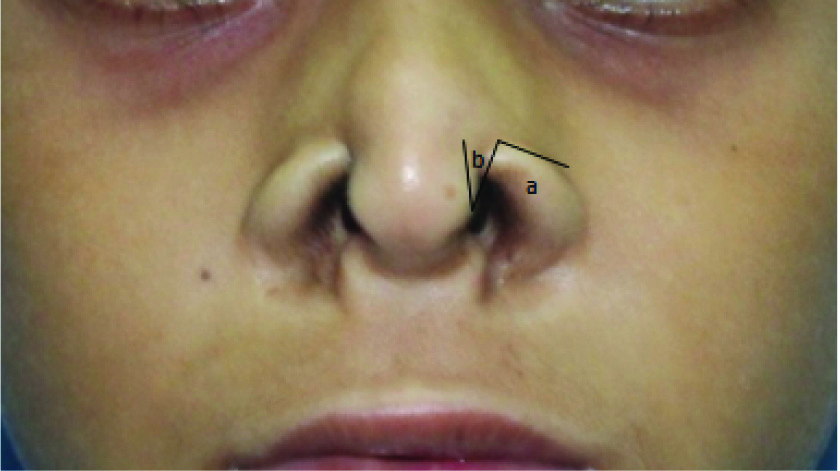
Incision markings.
a. Chondrocutaneous full thickness alar flap
b. Medial transpositional flap
c. Alar crease between upper and lower lateral cartilage

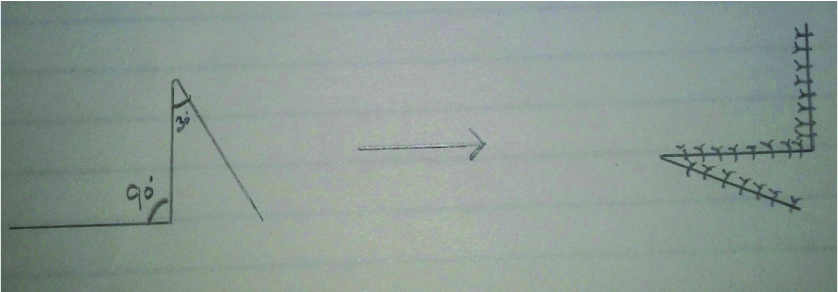
Schematic representation of unequal angled Z-plasty.
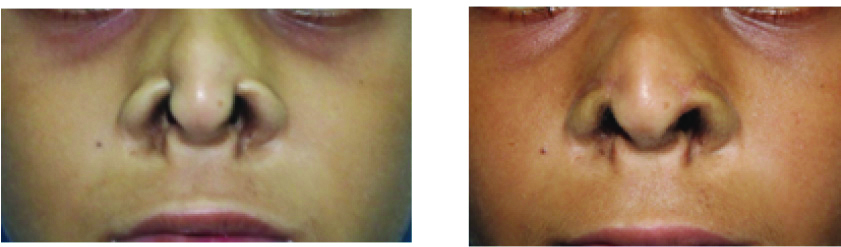
Bilateral correction of alar cleft-immediate post-operative.

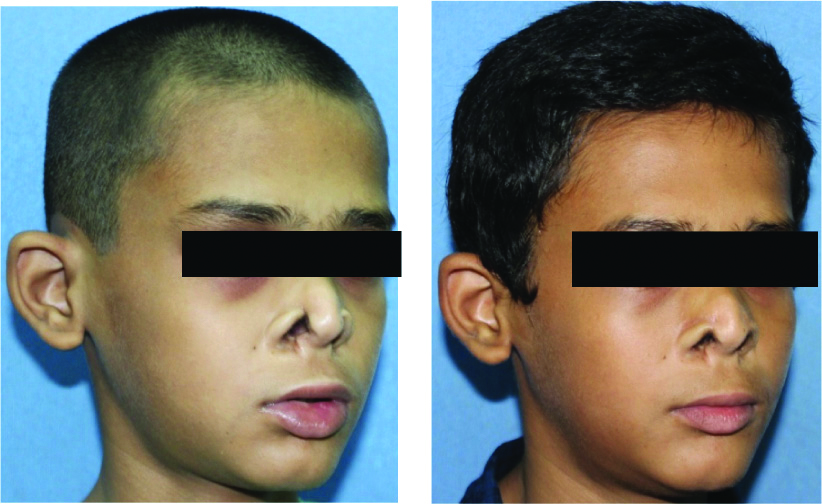
Post-operative at four months.
Good symmetry between the alar rims with no tissue hyperpigmentation and well concealed scar in the alar crease.
Discussion
Primitive face develops from five prominences and nose develops from the fronto-nasal process. Faulty development and/or fusion of lateral nasal process or absence of mesodermal penetration may cause cleft deformities. Brown in 1964, first hypothesised that isolated nasal cleft could occur in the absence of obvious cleft lip alveolus due to a primary defect in the alar cartilage [1]. Sushruta, considered as father of Indian surgery was the pioneer in reconstructive nasal surgery having described more than 15 nasal reconstruction methods [2].
Burget GC and Menick FJ gave the subunit approach, in which nose was divided into nine topographical subunits viz., tip, dorsum, columella and paired sidewalls, alar lobules and soft triangles and when more than 50% of a subunit is missing, replacing the entire subunit is required for better aesthetic results [3].
Surgical intervention of nasal clefts varies widely depending on the pattern and complexity of the deformity. The literature is replete with numerous cumbersome staged reconstructive procedures which includes but not limited to alar transposition with composite chondrocutaneous grafts, nasal dorsum rotation advancement flaps, forehead flaps, reconstruction with resorbable sheets, etc [4-7].
Ghareeb FM et al., gave a combined prospective and retrospective study describing different patterns of congenital nasal clefts and a treatment algorithm for management of different types of nasal clefts [8]. However, their work did not annotate the modifications of Z-plasty technique needed for nasal cleft reconstruction.
The principle of Z-plasty is one of the most versatile concepts in reconstructive surgery. The basic concept of Z-plasty was described as early as 1800s by Fricke, Horner, Serre and Denonvelliers [9]. But the geometric principles of Z-plasty were first elucidated by Limberg in late 1920s who insisted on the term ’transposed triangular flaps’ [Table/Fig-3]. The technique that is used in our case was that of unequal-angled Z-plasty. The two triangles formed here are of two different angles. The alar chondrocutaneous flap which was raised is approximately at right angle, while the medial transpositional flap is raised at a more acute angle, approximately 30°. The flap with more acute angle is pivoted in a greater arc than that of the larger angled flap. Designing a flap with very narrow angulations can adversely affect the outcome due to compromised blood supply. Any trans-positional flap with less than 30° angulation generally should be avoided for concern of vascularity of narrow triangular flaps created by these acute angles.
The main purpose of this kind of design is to restrict the incisions from encroaching into nearby anatomical subunits and at the same time to transpose the acute angled flap to a more desirable position.
The advantage of this kind of reconstruction is that the alar subunit as a whole is transposed including the inner mucosal lining and the lower lateral cartilage. This type of reconstruction provides with tissue and skin colour that is in perfect harmony with the adjacent subunits. The tissue hyperpigmentation associated with other chondrocutaneous graft technique is circumvented in this method [4]. This kind of incision design also provides a well concealed scar in the alar crease.
This simple yet versatile Z-plasty technique can be a superior alternative to other cumbersome flaps and multistage procedures, provided the size of the cleft is limited only to alar subunit and the adjacent tissues are normal with no tissue hypoplasia.
Bilateral isolated nasal cleft is a rare entity with no available data on their incidence. These clefts foster an astute surgeon to provide aesthetically appealing results. This technique provides a simple solution for these peculiar deformities provided there is little soft tissue deficit and the basic geometric principles of Z-plasty are acknowledged.
Conclusion
The application of unequal-angled Z-plasty principle and transposing the alar subunit as a whole makes this a novel technique for correction of isolated nasal cleft deformities. The virtues of this procedure viz. being a single staged procedure, transpositioning the whole alar chondrocutaneous subunit, not encroaching upon other anatomical sub units, well concealed scar within the alar crease, clearly supersede other commonly followed procedures in isolated nasal cleft management.
[1]. Brown RF, A reappraisal of the cleft-lip nose with the report of a caseBr J Plast Surg 1964 17:168-74.10.1016/S0007-1226(64)80025-4 [Google Scholar] [CrossRef]
[2]. Ralph GW, Watkinson CJ, History of head and neck surgeryIn Stell and Maran’s: Textbook of head and neck surgery and oncology 2012 5th edHodder Arnold:01-05.Watkinson CJ, Gilbert WR, editors10.1201/b13389-222020696 [Google Scholar] [CrossRef] [PubMed]
[3]. Burget GC, Menick FJ, The subunit principle in nasal reconstructionPlast Reconstr Surg 1985 76:239-47.10.1097/00006534-198508000-000104023097 [Google Scholar] [CrossRef] [PubMed]
[4]. Agrawal KS, Shende NK, Khare N, Deshpande ON, A novel technique for correction of congenital cleft of alaJ Cleft Lip Palate Craniofacial Anomalies 2014 1(2):2014-16.10.4103/2348-2125.137913 [Google Scholar] [CrossRef]
[5]. Reddy SG, Reddy RR, Obwegeser J, Mommaerts MY, Options for the nasal repair of non-syndromic unilateral Tessier no. 2 and 3 facial cleftsIndian J Plast Surg 2014 47(3):340-45.10.4103/0970-0358.14658825593418 [Google Scholar] [CrossRef] [PubMed]
[6]. Ramanathan M, Sneha P, Parameswaran A, Jayakumar N, Sailer HF, Reconstruction of nasal cleft deformities using expanded forehead flaps: A case seriesJ Maxillofac Oral Surg 2014 13(4):568-74.10.1007/s12663-013-0549-926225030 [Google Scholar] [CrossRef] [PubMed]
[7]. Bütow KW, Engelbrecht H, Tessier 2 nasal cleft: Reconstruction with a resorbable sheetBr J Oral Maxillofac Surg 2014 52(1):93-94.10.1016/j.bjoms.2013.05.14823777894 [Google Scholar] [CrossRef] [PubMed]
[8]. Ghareeb FM, Farghaly AS, Al Barah AM, El Sheikh YM, Raheim Fawzy HA, Patterns and management of congenital nasal cleftsMenoufia Med J 2015 28(1):99-106.10.4103/1110-2098.155960 [Google Scholar] [CrossRef]
[9]. Frodel LJ, Pawar SS, Wang DT, Z-plastyIn Baker: Local flaps in facial reconstruction 2014 3rd edElsevier/Saunders:317-38.Baker RS, editor [Google Scholar]