Ureteric Obstruction due to Aberrant Vessel Masquerading as Retrocaval Ureter
Sunirmal Choudhury1, Pritesh Jain2, Dilip Kumar Pal3
1 Assistant Professor, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
2 Resident, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
3 Professor and Head, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dilip Kumar Pal, Professor and Head, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata-700020, West Bengal, India.
E-mail: urologyipgmer@gmail.com, sunir09@gmail.com
Aberrant vessels, although rare, may extrinsically compress ureter which on imaging may masquerade as retrocaval ureter. The exact cause of obstruction in such atypical cases can be confirmed intraoperatively. We are presenting a case which on basis of radiological features was diagnosed as a case of retrocaval ureter, however, intraoperatively it was found to be a case of ureteric obstruction due to an aberrant vessel. Thus, whenever on imaging an atypical feature of retrocaval ureter is found, differential diagnosis of aberrant vessels should also be kept in mind.
Blood vessels, Urogenital abnormalities, Ureteral disease
Case Report
A 42-year-old female presented to the outpatient clinic with complaints of dull aching, intermittent pain in right loin region from last two years. She was a known case of recurrent urinary tract infection.
General physical examination was unremarkable. Urine examination revealed 3-5 pus cells per High-power Field (HPF) and occasional red blood cells per HPF. Biochemical indices including urea, creatinine, and electrolytes were within normal limits. Ultrasound of Kidney Ureter Bladder (KUB) region showed right sided hydronephrosis with dilated upper ureter. She was further evaluated with Computed Tomography (CT) urography, which showed hydronephrosis in right kidney and proximal part of right ureter was dilated and deviated medially. Ureter appeared to pass posterior to lower Inferior Vena Cava (IVC) at the L3-L4 vertebra and come out laterally at L5 and S1 vertebral junction [Table/Fig-1]. Retrocaval ureter was strongly suspected on the basis of imaging and absence of other abnormal findings. Thus, an open retroperitoneal approach was planned for her.
CT urogram images depicting right side hydronephrosis with ureter showing typical ‘S’ shaped proximal ureter suggestive of a type-1 retrocaval ureter.

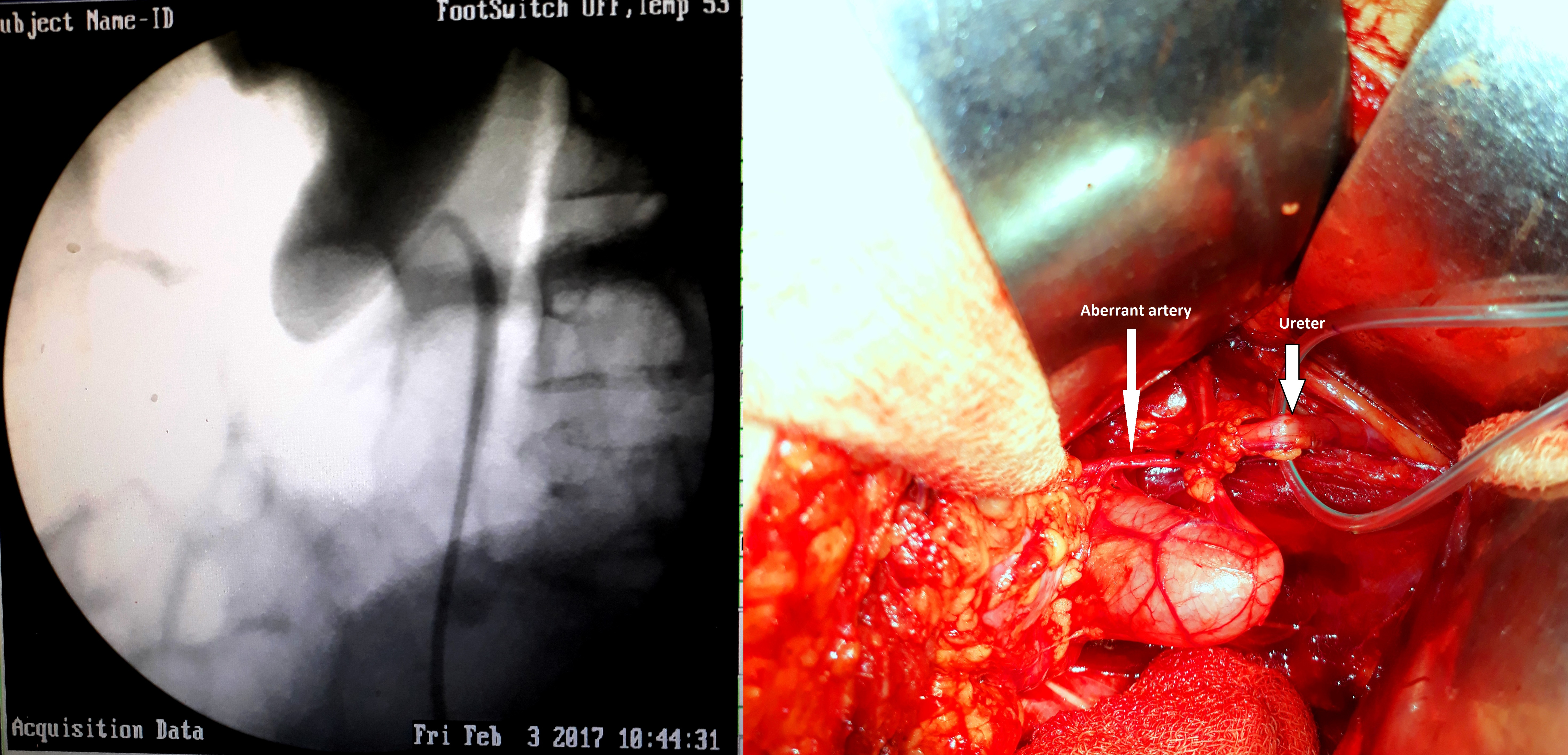
On the operation table, Retrograde Pyelogram (RGP) revealed looping and extrinsic compression of upper ureter, about 4 cm distal to ureteropelvic junction. Intraoperative findings revealed an aberrant vessel originating from aorta which was obstructing the upper ureter [Table/Fig-2]. The ureter was severely narrowed at constriction site. The narrow part of ureter was excised and pyeloureterostomy was done over ureteric stent, after repositioning of ureter in front of the aberrant vessel.
a) On operating table, retrograde pyelogram depicting angulation and looping of upper ureter; b) Intraoperative image showing aberrant vessel obstructing upper ureter. (Images from left to right)
Recovery of the patient was uneventful. Follow up excretory urogram showed normalisation of renal and ureteral anatomy.
Discussion
Kidneys ascent from sacral region to definitive lumbar location during embryological development. During this ascent, kidney receives blood supply from the aorta in a ladder-like pattern. As vessels are gained superiorly, those more inferiorly are shed. Unfavourable ureterovascular relationship may occur if there is an interruption in the normal process. This may lead to extrinsic compression of pelviureteric junction or rarely ureter. Besides intrinsic aetiology, aberrant vessels have a potential role in aetiology of ureteropelvic junction and ureteric obstruction. In normal kidneys, these aberrant vessels are found in about 20% of cases whereas in cases of ureteropelvic junction obstruction, they have been noted in 63% cases [1]. Error in the embryogenic development of IVC may lead to a rare congenital anomaly called retrocaval ureter or preureteral vena cava with reported incidence of 1 in 1500 with a 2.8- fold male predominance [2,3].
The IVP and RGP were commonly used to diagnose this condition; however, spiral CT is now considered an investigation of choice for diagnosis of retrocaval ureter and other IVC abnormalities [4-6]. According to the new classification, retrocaval ureter is of two types based on radiologic imaging [7]. In the present case imaging revealed a typical ‘S’ shaped type-1 deformity of the ureter with point of obstruction placed at the level of third lumbar vertebra. Intraoperatively, the cause of ureteric obstruction was found to be aberrant vessel arising from the aorta. Aberrant vessels may obstruct upper, mid or even lower ureter [8]. To identify such crossing vessels numerous modalities have been used like angiography, endoluminal ultrasound, doppler ultrasound, CT scan, and magnetic resonance imaging [9]. Out of these, helical CT scan with three-dimensional reconstruction seems most suitable in preoperative assessment of crossing vessels [10].
Preoperative diagnosis of presence of aberrant vessel although does not change the management modality, however, it helps in precisely planning and selecting appropriate surgical approach which ultimately would lead to significant reduction in intraoperative complications.
Conclusion
Ureteric obstruction due to aberrant vessels may masquerade as preureteral vena cava on imaging. Aberrant vessels may have a profound effect on treatment outcome, thus it should not be ignored as a differential diagnosis in cases of preureteral vena cava. Preoperative identification of aberrant vessels is of utmost significance as it may influence treatment approach, intraoperative complications and clinical outcome.
[1]. Richstone L, Seideman CA, Reggio E, Bluebond-Langner R, Pinto PA, Trock B, Pathologic findings in patients with ureteropelvic junction obstruction and crossing vesselsUrology 2009 73:716-19.10.1016/j.urology.2008.10.06919193425 [Google Scholar] [CrossRef] [PubMed]
[2]. Heslin JE, Mamonas C, Retrocaval ureter: report of four cases and review of literatureJ Urol 1951 65(2):212-22.10.1016/S0022-5347(17)68477-5 [Google Scholar] [CrossRef]
[3]. Kenawi MM, Williams DI, Circumcaval ureter: a report of four cases in children with a review of the literature and a new classificationBr J Urol 1976 48(3):183-92.10.1111/j.1464-410X.1976.tb10197.x779921 [Google Scholar] [CrossRef] [PubMed]
[4]. Bissi A, Rigatti P, L’uretere circumcavaleChir Arch Trim 1977 :41 [Google Scholar]
[5]. Bass FE, Redwine MD, Kramer LA, Huynh PT, Harris JH, Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findingsRadiographics 2000 20:639-52.10.1148/radiographics.20.3.g00ma0963910835118 [Google Scholar] [CrossRef] [PubMed]
[6]. Singh DD, Sanjeev P, Sharma RK, Spiral CT evaluation of circumcaval ureter (retrocaval ureter)Ind J Radiol Imag 2001 11:83-84. [Google Scholar]
[7]. Bateson E, Atkinson D, Circumcaval ureter: a new classificationClin Radiol 1969 20:173-77.10.1016/S0009-9260(69)80166-2 [Google Scholar] [CrossRef]
[8]. Kurimoto S, Kitamura T, Ueki T, Moriyama N, Tajima A, Obstruction of the lower ureter caused by an aberrant vesselBr J Urol 1997 80:355-56.10.1046/j.1464-410X.1997.00292.x9284224 [Google Scholar] [CrossRef] [PubMed]
[9]. Mitterberger M, Pinggera GM, Neururer R, Peschel R, Colleselli D, Aigner F, Comparison of contrast-enhanced color doppler imaging (CDI), computed tomography (ct), and magnetic resonance imaging (MRI) for the detection of crossing vessels in patients with ureteropelvic junction obstruction (UPJO)Eur Urol 2008 53:1254-60.10.1016/j.eururo.2007.11.03118037558 [Google Scholar] [CrossRef] [PubMed]
[10]. Rouviere O, Lyonnet D, Berger P, Pangaud C, Gelet A, Martin X, Ureteropelvic junction obstruction: use of helical CT for preoperative assessment-comparison with intraarterial angiographyRadiology 1999 213:668-73.10.1148/radiology.213.3.r99dc2266810580937 [Google Scholar] [CrossRef] [PubMed]