Vertebro-Subclavian Trunk: A Rare Aortic Arch Anomaly
CS Rameshbabu1, Vinay Sharma2, Arjun Kumar3, Muhammad Qasim4, Om Prakash Gupta5
1 Associate Professor, Department of Anatomy, Muzaffarnagar Medical College, Muzaffarnagar, Uttar Pradesh, India.
2 Associate Professor, Department of Anatomy, Muzaffarnagar Medical College, Muzaffarnagar, Uttar Pradesh, India.
3 Postgraduate Student, Department of Medical Anatomy, Rama Medical College, Ghaziabad, Uttar Pradesh, India.
4 Consultant Radiologist, Department of Radiology, Dr. O.P. Gupta Imaging Centre, Bacha Park, Meerut, Uttar Pradesh, India.
5 Consultant Radiologist, Department of Radiology, Dr. O.P. Gupta Imaging Centre, Bacha Park, Meerut, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vinay Sharma, Associate Professor, Department of Anatomy, Muzaffarnagar Medical College, N.H.-58, Begrajpur Industrial Area, Muzaffarnagar-251203, Uttar Pradesh, India.
E-mail: vinay_sharma1979@yahoo.com
Introduction
Variations in the branching pattern of the arch of aorta are not uncommon. The common trunk of origin of left vertebral and left subclavian arteries from the arch of aorta, named as the Vertebro-Subclavian Trunk (VST), is a very rare aortic arch branching anomaly sporadically reported in the literature.
Aim
To assess the aortic arch branching anomalies especially the presence of the VST.
Materials and Methods
Contrast Enhanced Computed Tomographic (CECT) scans of chest of 410 patients were analysed and interpreted by two radiologists.
Results
The VST was noted in three male patients with an estimated incidence of 0.73%. In one male patient the VST was associated with the presence of a common stem of origin of brachiocephalic trunk and left common carotid artery (so called bovine arch). Thus, there were two common trunks originating from the arch.
Conclusion
Careful observation of aortic arch branching pattern has revealed the presence of origin of left vertebral artery from the root of left subclavian artery just above the arch, the common trunk designated as VST. Catheterisation of left vertebral artery in such cases may be difficult and adequate pre-procedural knowledge can help in successful accomplishment of interventional procedures.
Arch of aorta, Bovine arch, Left subclavian artery, Left vertebral artery
Introduction
Traditionally, variations in the branching pattern of Aortic Arch (AA) were considered as ‘normal variants’ since, many of these variants did not cause any significant clinical symptoms and as such received scant attention in the imaging literature [1]. The advent of several surgical and endovascular interventional procedures on supra-aortic branches have revived interest in the study of AA branching variations. Precise knowledge of the anatomical variations of AA branches is of crucial importance before undertaking any interventional and surgical procedures in chest and neck to avoid any complications. Normally, the AA is left sided and gives three branches, the Brachiocephalic Trunk (BCT), Left Common Carotid Artery (LCCA) and Left Subclavian Artery (LSA). This three branched pattern, called normal pattern (Type-I), is observed in 71%-96.6% of patients in radiological studies [2-5]. The most common variation of branching pattern is the presence of a common trunk of BCT and LCCA, the so called “bovine arch” (Type-II) with a prevalence of 2.6%-27.4% [1,6-8]. The second most common variant branch is the direct AA origin of Left Vertebral Artery (LVA) (Type-III) with a reported incidence of 2.8% to 6.6% [1,4,9]. Several other types of AA branching pattern variations have been reported including aberrant retroesophageal right subclavian artery, bicarotid trunk, bilateral brachiocephalic trunks and anomalies like double aortic arch and right AA [1-4,6,7].
The occurrence of VST, indicating the common trunk of origin of LSA and LVA from the AA, was sporadically reported in several cadaveric studies [10-13]. Cetin I et al., reported VST in a patient undergoing cardiac catheterisation [14]. Only one radiological investigation involving 2287 patients observed the common trunk of LSA and LVA in 0.3% cases [9]. The presence of VST was not reported by several radiological studies on a large number of patients suggesting its rarity and probable ethnic variation [1,4,6,7]. Yazar F et al., reported two common trunks, the first common trunk of BCT and LCCA and the second common trunk of LSA and LVA arising from the AA in a female cadaver for the first time [15]. We recently reported what we believed to be the second case in English literature, the origin of two common trunks, in a male cadaver [16]. The present study was undertaken with a view to specifically assess the variable origin of LVA from the VST in subjects who underwent CECT of thorax.
Materials and Methods
We retrospectively reviewed CT scans of 410 patients referred to Dr. O. P. Gupta Imaging Centre, Meerut, for CECT of the thorax for suspected pathologies of lungs and mediastinum during the period September 2015 to March 2016. Before conducting the study, the clearance was taken from the Institutional Ethical Committee. The study population included 245 males and 165 females (age ranging from six months to 86 years, mean age 51.28±17.70 years). The scans of the patients with malignancies likely to distort the anatomy of AA, poorly enhanced scans and those with thoracic aortic disease were excluded from the study.
All patients underwent contrast enhanced Multi-Detector Computed Tomography (MDCT) by a 64 channel scanner (GE Optima 660, 2011, Tokyo, Japan) and received 90-100 mL of non-ionic iohexol contrast (Omnipaque 350 mg I/mL; GE Healthcare, Shanghai, China) at the rate of 5 mL/s intravenously. A written informed consent was obtained by the diagnostic centre from each patient before contrast injection. Sections of 0.625 mm thickness were obtained from lower part of the neck to upper part of abdomen and analysed in a separate work station (GE: AW Volume share 4.5). After analysing axial, coronal and sagittal scans, Volume Rendered (VR) and Maximum Intensity Projections (MIP) were obtained. We specifically looked for the presence of common trunk of origin of LSA and LVA, the VST.
Results
The normal branching pattern of BCT, LCCA and LSA arising from the AA was observed in 306 (74.63%) patients and variations in 104 (25.37%) cases. Direct AA origin of LVA was noted in 29 (7.07%) cases and in two of these cases common trunk of BCT and LCCA was also present. A common trunk of BCT and LCCA (so called bovine arch) was observed in 69 (16.82%) cases. The estimated prevalence of VST was 3 (0.73%) out of 410 cases . In two male patients, the arch gave rise to three branches-BCT, LCCA and VST [Table/Fig-1,2]. The LVA was arising from the posteromedial aspect of the common VST 4 mm above the arch in one case and 9.2 mm above the arch in the second case [Table/Fig-1]. The AA of the third patient gave origin to two common trunks, first the common trunk of BCT and LCCA (bovine trunk) and the second common trunk of LSA and LVA (VST) [Table/Fig-3,4].
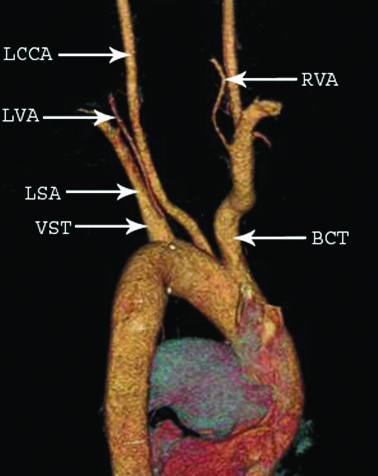
Volume rendered image of arch of aorta (posterior view) of a 59-year-old male patient showing vertebrosubclavian trunk (VST) arising as the third branch giving rise to Left Vertebral Artery (LVA) and Left Subclavian Artery (LSA). Right Vertebral Artery (RVA) has normal origin. BCT- Brachiocephalic Trunk, LCCA- Left Common Carotid Artery.
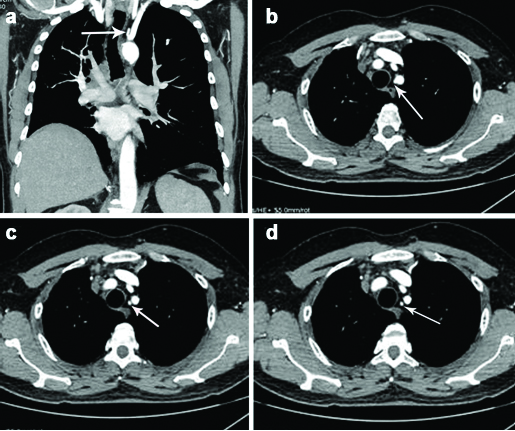
Coronal section (a) and serial axial sections; (b-d) showing the origin of left vertebral artery (arrow) from the root of left subclavian artery in a 59-year-old male patient.
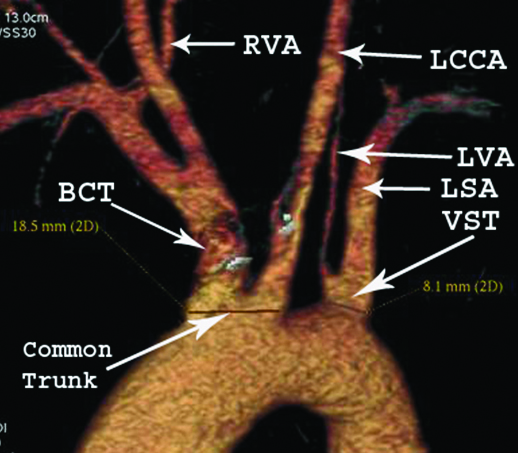
Volume rendered image of arch of aorta (anterior view) of a 34-year-old male patient showing origin of two common trunks, first common trunk of Brachiocephalic (BCT) and Left Common Carotid (LCCA) and the second, Vertebrosubclavicn Trunk (VST) giving rise to Left Vertebral (LVA) and Left Subclavian Arteries (LSA). Right Vertebral Artery (RVA) has normal origin.
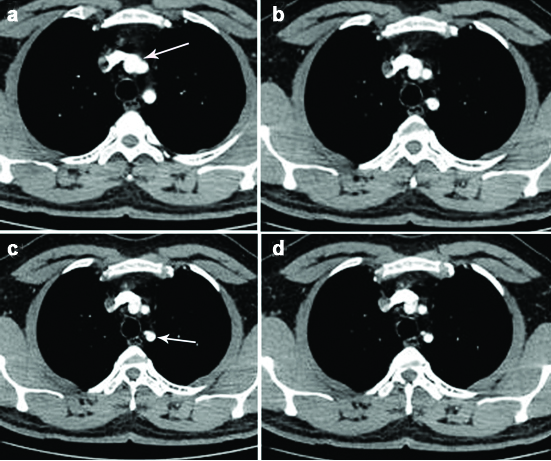
Serial axial sections (a-d) showing two common trunks. In axial section a, common bovine trunk (arrow) and in axial section c, the vertebrosubclavian trunk (arrow) are shown.
Discussion
Isolated variations in the branching pattern of AA are usually asymptomatic and are detected incidentally during autopsy or radiological investigations and hence, did not attract much attention in imaging literature. Recognition of the variants and anomalies of the branching pattern of AA has diagnostic and therapeutic implications [1]. A pattern different from what is observed in majority of the population and not causing any clinical symptom is defined by Rea G et al., as an anatomical ‘variant’ and a pattern with a marked deviation from the normal due to congenital or hereditary defects and causing symptoms is termed an anomaly [3]. Berko NS et al., suggested that any variation occurring in less than 1% of the population should be considered as an ‘anomaly’ irrespective of its clinical significance [1].
Normally each vertebral artery originates from first part of the corresponding subclavian artery in the root of the neck but may have an aberrant origin. After analysing 171 available literature case reports, the aberrant origin of LVA was found to be more common than that of the RVA (94 versus 47cases) and bilateral variable origin was reported in 30 cases [17]. The LVA has a variable origin directly from the arch of aorta between the origins of LCCA and LSA or from the arch distal to the origin of LSA or has a dual origin. Such an aberrant origin may be associated with atheroscleorsis, increased susceptibility to dissection and altered haemodynamics resulting in intracranial complications [17].
The present study revealed the presence of VST, a very rare anomaly of branching pattern of AA, in three male patients with an estimated prevalence of 0.73 %. This common trunk of origin of LSA and LVA was sporadically reported mainly in cadaveric studies [10-13,18,19]. Some cadaveric studies described this variant trunk as LVA origin from LSA in the superior mediastinum or as LVA originating from arch of aorta at the junction of origin of LSA [20-22]. Gluncic V et al., observed an atypical three branched pattern of bicarotid trunk (common trunk of both common carotids), VST and retroesophageal right subclavian artery in a cadaver and claimed that common trunk of LSA and LVA has not been reported till that time [23]. Uchino A et al., recently reported VST with an incidence of 0.3% after analysing CT angiographic scans of 2287 Japanese patients [9].
Yuan comprehensively reviewed pertinent literature on aberrant origin of vertebral artery in a cohort of 1286 cases and noted the presence of common trunk of LVA and LSA in 1.6% cases [24]. Features of the VST reported in the literature are summarised in [Table/Fig-5] [9-16,18-23,25].
Earlier reports of the vertebro-subclavian trunk.
| S. No. | Author and Year | Modality | Number of cases with VST (Total number) | Gender and Age | Ethnicity/Country | Other associated anomalies, if any |
|---|
| 1 | Gluncic V et al., [23] | Cadaveric dissection | 1 | Female 67 years | Croatia | Bicarotid trunk (common trunk of both carotid arteries), RVA from RCCA,Retroeophageal RSA |
| 2 | Nelson ML and Sparks CD [10] | Autopsy | 2(193 autopsies) | Male | Japanese-American | |
| 3 | Yazar F et al., [15] | Cadaveric dissection | 1 | Female 25 years | Turkey | (Associated with common trunk of BCT and LCCA. Two common trunks from the arch.) |
| 4 | Cetin I et al., [14] | Cardiac Catheterization | 1 | | Turkey | |
| 5 | Ogeng’o JA et. al., [11] | Cadaveric dissection | 1 (113 cases. 0.9%) | ------- | Kenyan | |
| 6 | Alsaif HA and Ramadan WS [18] | Cadaveric dissection | 1(36 cases- 11.0%) | | Saudi Arabia | |
| 7. | Bayat PD et al., [20] | Cadaver / MRA | 1 | Female 70 years | Iran | (Described by authors as origin of LVA from LSA in the superior mediastinum) |
| 8 | Kumar S et al., [19] | Cadaveric Dissection | 2(30cases- 6.66%) | | Indian | |
| 9 | Ottone NE et al., [12] | Cadaveric dissection | 2(51 cases-3.92%) | | Caucasians Argentina | |
| 10 | Rekha P and Senthilkumar S [21] | Cadaveric Dissection | 2(110 cases- 1.8%) | | Indian | (Described by authors as LVA originating from the arch of aorta at upper angle of the junction of LSA) |
| 11 | Uchino A et al., [9] | CT Angiography | 8(2287 cases-0. 3%) | Males (4)Females (4) | Japanese | |
| 12 | Pillai TJ et al., [22] | Cadaveric dissection | 1(12 cases) | Male | Indian | (Described by authors as LVA originating from the arch of aorta at upper angle of the junction of LSA) |
| 13 | Sateesha BN et al., [13] | Cadaveric dissection | 1 | Male65 years | Indian | |
| 14 | Reddy Nune GK et al., [25] | Cadaveric dissection | 1 | Male | Indian | (Associated with common trunk of BCT and LCCA) |
| 15 | Ramesh Babu CS and Sharma V [16] | Cadaveric Dissection | 1 | Male | Indian | (Associated with common trunk of BCT and LCCA- Two common trunks from the arch) |
| 16 | Present Study, 2017 | CECT- Thorax | 3(410 cases 0.73%) | Males | Indian | (One case associated with common trunk of BCT and LCCA- Two common trunks from the arch) |
In the present study, VST was observed in three male patients as the last branch of the arch of aorta giving origin to LVA from its posteromedial aspect. More frequently, LVA takes origin directly from AA in between the origins of LCCA and LSA which is the second most common variant branching pattern. Awareness of anomalous origin of LVA is crucial prior to cerebral angiography for assessment of posterior circulation because LVA is preferably used for catheterisation [7]. Interventional procedures on LVA arising from VST will be technically difficult and may result in complications. It is believed that the proximal part of vertebral arteries is prone to atherosclerotic changes close to their origin. Variations of LVA are associated with higher incidence of spontaneous dissection due to congenital defects in the arterial wall or altered cerebral haemodynamics that can result in cerebral dysfunctions [1].
Incidentally, in a male subject, we have also observed the origin of two common trunks, the first common trunk of BCT and LCCA and the second common trunk of LSA and LVA. A literature search has indicated that such a rare anomalous branching pattern was reported twice earlier, first in a female Turkish cadaver and second in a male Indian cadaver [15,16]. The occurrence of two common trunks, the vertebro-subcavian and the bovine or brachiocarotid trunk, to the best of our knowledge, is the first radiological case to be reported. Reddy Nune GK et al., noted the origin of LVA from LSA near the arch of aorta in a cadaveric heart which also presented the common trunk of BCT and LCCA, but did not describe this condition as two common trunks [25]. In the present study, the common trunk of BCT and LCCA was noted in 16.82% cases only. Celikyay ZR et al., preferred the term “bovine type arch” to denote this variant because in cattle a single trunk arising from the arch gives rise to both subclavian arteries and then continues as a common bicarotid trunk [7]. Vasovic LJ et al., used the term ‘brachiocarotid trunk’ for the common trunk of origin of BCT and LCCA [17]. Two subtypes of this variant can be distinguished, one with a long bovine trunk described as LCCA arising from BCT (type-A) and one with a short bovine trunk described as the common origin of LCCA and BCT (type-B). The present case belongs to type-B. The clinical significance of the common trunk of BCT and LCCA lies in the fact that three branches from this trunk (left and right common carotids and right vertebral from right subclavian) supply a major portion of the brain and occlusive disorders of this trunk can precipitate catastrophic cerebral ischaemia.
Embryologically, the arch of aorta and its branches are the derivatives of six pairs of pharyngeal arch arteries. Normally, the left third arch artery connected to the left horn of the aortic sac elongates to form LCCA and the left horn of aortic sac itself will form that part of the arch of aorta between the origins of BCT and LCCA. The right horn of aortic sac will develop into BCT. The common trunk of origin of BCT and LCCA may be due to the regression or slower growth rate of left horn of aortic sac such that the Left Third Arch Artery (LCCA) gets connected to the right horn of aortic sac (BCT). The aortic arch origin of LVA is explained by the persistence of sixth intersegmental artery and regression of dorsal branch of seventh intersegmental artery which normally develops into V-1 segment of the vertebral artery [24]. Incorporation of the proximal left seventh intersegmental artery into the developing arch of aorta could also result in LVA originating directly from the aortic arch [10]. It is suggested that persistence of sixth intersegmental artery and absorption of a portion of left fourth arch artery into the developing LSA could result in the origin of LVA from the root of LSA, the so called VST [10]. The causative factors producing the branching pattern anomalies of the AA are not known. A study on 66 patients with isolated AA anomalies of laterality or branching pattern, without any associated intra-cardiac defects, revealed that 24% of patients have deletion of chromosome 22 q11 [26].
The importance of recognition and appreciation of AA anatomy and anomalous branching pattern cannot be overlooked as it allows accurate surgical planning, successful accomplishment of various interventional procedures and prevention of potential complications. Difficulties will be encountered while performing left vertebral angiography or other interventional procedures if the presence of VST remains unrecognised. There is an increased risk of neurological complications in patients having AA anomalies [27,28]. After examining the imaging data of 556 patients with the thoracic aortic disease, Dumfarth J et al., suggested that the atypical branching pattern of AA may be considered as a potential anatomical marker for future development of thoracic aortic disease [29].
Limitation
Main limitation of this study is a smaller sample size of the population and not including the cases of neurological complications of posterior cerebral circulation to correlate the association of anomalous origin of LVA with the presence of atherosclerosis or dissection. Future studies on a larger sample size are desired. The present study has indicated that prior knowledge of the anomalous origin of LVA is desirable before undertaking any interventional or operative procedures. Since, MDCT provides exquisite anatomical details of variant branching pattern of AA noninvasively, it can be used as the imaging modality of choice before undertaking any interventional radiological and surgical procedures on supra-aortic branches to avoid any complications.
Conclusion
The present study has provided evidence for the occurrence of the VST with an incidence of 0.73% while specifically looking for it. Prior knowledge of such rare anomalies has greatly enhanced the ability to identify and record them. For successful performance of radiological and surgical interventional procedures thorough anatomical knowledge of variant AA branching pattern is essential. Recent evidence has suggested that anomalous AA branching pattern may increase the risk of neurological complications and act as potential markers for future development of thoracic aortic disease.
[1]. Berko NS, Jain VR, Godelman A, Stein EG, Ghosh S, Haramati LB, Variants and anomalies of thoracic vasculature on computed tomographic angiography in adultsJ Comput Assist Tomogr 2009 33:523-28.10.1097/RCT.0b013e318188834319638843 [Google Scholar] [CrossRef] [PubMed]
[2]. Ergun E, Simsek B, Kosar PN, Yilmaz BK, Turgut AT, Anatomical variations in branching pattern of arcus aorta: 64 slice CTA appearanceSurg Radiol Anat 2013 35:503-09.10.1007/s00276-012-1063-323271166 [Google Scholar] [CrossRef] [PubMed]
[3]. Rea G, Valente T, Iaselli F, Urraro F, Izzo A, Sica G, Multi-detector computed tomography in the evaluation of variants and anomalies of aortic arch and its branching patternItalian J Anat Embryol 2014 119:180-92. [Google Scholar]
[4]. Vucurevic G, Marinkovic S, Puskas L, Kovacevic I, Tanaskovic S, Radak D, Anatomy and radiology of the variations of aortic arch branches in 1266 patientsFolia Morphol 2013 72:113-22.10.5603/FM.2013.0019 [Google Scholar] [CrossRef]
[5]. Sunitha V, Rao BN, A study on the anatomical organization of the aortic arch anomaliesJ Clin Diagn Res 2012 6:1127-31. [Google Scholar]
[6]. Boyaci N, Dokumaci DS, Karakas E, Yildiz S, Cece H, Kocarslan A, Multidetector computed tomography evaluation of aortic arch and branching variantsTurk Gogus Kalp Dama 2015 23:51-57.10.5606/tgkdc.dergisi.2015.10290 [Google Scholar] [CrossRef]
[7]. Celikyay ZR, Koner AE, Celikyay F, Deniz C, Acu B, Firat MM, Frequency and imaging findings of variations in human aortic arch anatomy based on multidetector computed tomography dataClin Imaging 2013 37(6):1011-19.10.1016/j.clinimag.2013.07.00823938139 [Google Scholar] [CrossRef] [PubMed]
[8]. Uchino A, Saito N, Okada Y, Kozawa E, Nishi N, Mizukoshi W, Variation of the origin of the left common carotid artery diagnosed by CT angiographySurg Radiol Anat 2013 35:339-42.10.1007/s00276-012-1038-423129264 [Google Scholar] [CrossRef] [PubMed]
[9]. Uchino A, Saito N, Takahashi M, Okada Y, Kozawa E, Nishi N, Variations in the origin of the vertebral artery and its level of entry into the transverse foramen diagnosed by CT angiographyNeuroradiology 2013 55:585-94.10.1007/s00234-013-1142-023344682 [Google Scholar] [CrossRef] [PubMed]
[10]. Nelson ML, Sparks CD, Unusual aortic arch variation: distal origin of common carotid arteriesClin Anat 2001 14:62-65.10.1002/1098-2353(200101)14:1<62::AID-CA1012>3.0.CO;2-# [Google Scholar] [CrossRef]
[11]. Ogeng’o JA, Olabu BO, Gatonga PM, Munguti JK, Branching pattern of aortic arch in a Kenyan populationJ Morphol Sci 2010 27:51-55. [Google Scholar]
[12]. Ottone NE, Casola L, Cirigliano V, Oloriz L, Blasi ED, Medan CD, Two cases of left vertebral artery emerging from a trunk in common with the left subclavian artery from the aortic archInt J Morphol 2013 31:646-49.10.4067/S0717-95022013000200049 [Google Scholar] [CrossRef]
[13]. Sateesha BN, Sirasanagandla SR, Surekha DS, Deepthinath R, Sudarshan S, Raghu J, Variant origin of the left vertebral artery from a vertebro-subclavian trunk associated with an unusual branch arising from the brachiocephalic trunkJournal of Surgical Academia 2014 4:73-75. [Google Scholar]
[14]. Cetin I, Varan B, Orun UA, Tokel K, Common trunks of the subclavian and vertebral arteries: presentation of a new aortic arch anomalyAnn Vasc Surg 2009 23:142-43.10.1016/j.avsg.2008.02.01518423960 [Google Scholar] [CrossRef] [PubMed]
[15]. Yazar F, Yalcin B, Ozan H, Variation of the aortic arch branches: two main trunks originating from the aortic archGazi Medical Journal 2003 14:181-84. [Google Scholar]
[16]. Ramesh Babu CS, Sharma V, Two common trunks arising from arch of aorta: Case report and literature review of a very rare variationJ Clin Diagn Res 2015 9:AD05-AD07.10.7860/JCDR/2015/14219.625326393115 [Google Scholar] [CrossRef] [PubMed]
[17]. Vasovic Lj, Radenkovic G, Trandafilovic M, Dordevic G, Variable left and /or right vertebral artery in prevertebral part: A review of features in the postnatal periodMedicine and Biology 2015 17:1-25. [Google Scholar]
[18]. Alsaif HA, Ramadan WS, An anatomical study of the aortic arch variationsJKAU: Med Sci 2010 17:37-54.10.4197/Med.17-2.4 [Google Scholar] [CrossRef]
[19]. Kumar S, Haq I, Kathiresan K, Study of branching pattern of arch of aorta and its variationsNatl J Clin Anat 2012 1(4):176-80. [Google Scholar]
[20]. Bayat PD, Ghanbari A, Esmaeili S, Esmaeili K, Abnormal originating of vertebral artery in the superior mediastinum: A case reportEur J Anat 2011 15:117-20. [Google Scholar]
[21]. Rekha P, Senthilkumar S, A study on branching pattern of human aortic arch and its variations in south Indian populationJ Morphol Sci 2013 30:11-15. [Google Scholar]
[22]. Pillai TJ, Indira T, Ramadevi A, Sobhadevi T, Rajaram G, Sumalatha N, Abnormal origin and course of left vertebral arteryInt J Res Stud Biosc 2014 2:17-19. [Google Scholar]
[23]. Gluncic V, Ivkic G, Marin D, Percac S, Anomalous origin of both vertebral arteriesClin Anat 1999 12:281-84.10.1002/(SICI)1098-2353(1999)12:4<281::AID-CA8>3.0.CO;2-6 [Google Scholar] [CrossRef]
[24]. Yuan SM, Aberrant origin of vertebral artery and its clinical implicationsBraz J Cardiovasc Surg 2016 31:52-59.10.5935/1678-9741.2015007127074275 [Google Scholar] [CrossRef] [PubMed]
[25]. Reddy Nune GK, Patra M, Rama Rao K, Left common carotid artery arising from the brachiocephalic trunk: a case report seen in 4 heartsJ Evidence Based Med & Hlthcare 2014 1:428-34.10.18410/jebmh/2014/68 [Google Scholar] [CrossRef]
[26]. McElhinney DB, Clark BJ, Weinberg PM, Kenton ML, McDonald-McGinn D, Driscoll DA, Association of chromosome 22q11 deletion with isolated anomalies of aortic arch laterality and branchingJ Am Coll Cardiol 2001 37(8):2114-19.10.1016/S0735-1097(01)01286-4 [Google Scholar] [CrossRef]
[27]. Faggioli GL, Feri M, Freyrie A, Gargiulo M, Fratesi F, Rossi C, Aortic arch anomalies are associated with increased risk of neurological events in carotid stent proceduresEur J Vasc Endovasc Surg 2007 33:436-41.10.1016/j.ejvs.2006.11.02617240174 [Google Scholar] [CrossRef] [PubMed]
[28]. Komiyama M, Morikawa T, Nakajima H, Nishikawa M, Yasui T, High incidence of dissection associated with left vertebral artery of aortic originNeurol Med Chir 2001 41:8-11.10.2176/nmc.41.811218642 [Google Scholar] [CrossRef] [PubMed]
[29]. Dumfarth J, Chou AS, Ziganshin BA, Bhandari R, Peterss S, Tranquilli M, Atypical aortic arch branching variants: A novel marker for thoracic aortic diseaseJ Thorac Cardiovasc Surg 2015 149:1586-92.10.1016/j.jtcvs.2015.02.01925802134 [Google Scholar] [CrossRef] [PubMed]